





This article presents the psychometric properties for the Portuguese population of a brief self-report scale for diagnosing anorexia nervosa (AN), bulimia nervosa (BN), and binge-eating disorder (BED): the Eating Disorder Diagnostic Scale (Stice et al., 2000).
MethodTo study the psychometric properties of EDDS, an exploratory factor analysis was done first, followed by a confirmatory factor analysis.
ResultsThe results of the exploratory factor analysis revealed the existence of three components and the confirmatory factor analysis showed a structure with three latent variables (Body and Weight Concerns, Binge Eating Behaviour and Compensatory Behaviours), with a second order variable (Eating Disorder Symptoms) with a good adjustment fit. The internal consistency and the test–retest correlations revealed an adequate reliability and the inter-correlations of the EDDS subscales with other measures of the same and different constructs, supported the convergent and discriminant validity of this measure.
ConclusionsSumming up, the EDDS seems to be a useful measure to assess eating disorders symptomatology in the Portuguese population.
En este artículo se presentan las propiedades psicométricas para la población portuguesa de una escala breve de autoinforme para el diagnóstico de la anorexia nerviosa, la bulimia nerviosa y el trastorno por atracones: la Escala de Diagnóstico del Trastorno Alimentario (EDTA; Stice, Telch y Rizvi, 2000).
MétodoPara estudiar las propiedades psicométricas de la EDTA se efectuó un análisis factorial exploratorio, seguido por un análisis factorial confirmatorio.
ResultadosLos resultados del análisis factorial exploratorio muestran la existencia de 3 componentes y el análisis confirmatorio evidencia una estructura con 3 variables latentes (preocupaciones sobre el cuerpo y el peso, comportamientos de ingesta por atracones y conductas compensatorias), con un factor de segundo orden (síntomas de trastornos de alimentación) con un buen ajuste. La consistencia interna y las correlaciones test-retest muestran una confiabilidad adecuada, y las intercorrelaciones de las subescalas de la EDTA con otras medidas del mismo y de diferentes constructos fortalecen la validez convergente y discriminante de la medida.
ConclusionesEn resumen, la EDTA parece ser una medida útil para evaluar sintomatología de trastornos de la alimentación en la población portuguesa.
Eating disorders are a serious health problem for adolescents and adults (Hoek & van Hoeken, 2003). The description of the aetiology, epidemiology and related diagnostic criteria for AN, BN and ED not otherwise specified (e.g., BED), are essential for a better understanding of the different manifestations of these disorders and for the development of fitted interventions.
Currently, eating disorders are widely recognized, being an important object of interest to the public and researchers, and a challenge to clinicians (Fairburn & Harrison, 2003). Underlying this interest is the prevalence of these disorders, which lies between 3 and 10% for young women considered at risk due to their age (between 15 and 29 years old) (Polivy & Herman, 2002). Even though the prevalence is higher in females (American Psychiatric Association, 2013), there has been an increase in males presenting body dissatisfaction and concerns with body weight and shape. Furthermore, it is known that these concerns represent for a significant number of young males the onset of problems in eating behaviour, which may contribute to the development of eating disorders (Ricciardelli & McCabe, 2004; Vo, Lau & Rubinstein, 2016).
Eating disorders meeting all specific diagnostic criteria are relatively rare in general population (Smink, van Hoeken & Hoek, 2012; Striegel-Moore & Cachelin, 2001). When using strict diagnostic criteria, estimates are approximate 0.3% for AN and 1% for BN (Hoek & van Hoeken, 2003). The so-called Eating Disorder Not Otherwise Specified (EDNOS), characterized by the significant features of eating disorder symptoms that do not meet the criteria for AN or BN (American Psychiatric Association, 2000), constitutes the most common eating disorder among those who seek for treatment, and are even more common among individuals with eating disorders within the community (Machado, Gonçalves & Hoek, 2013; Machado et al., 2007; Thomas, Vartanian & Brownell, 2009).
The mortality rates associated with eating disorders are considered to be high and, in some cases, higher than for other psychiatric disorders (Arcelus, Mitchell, Wales & Nielsen, 2011) which points for the necessity of an effective assessment aimed at preventing a poorer outcome.
The evaluation of binge eating remains one of the most difficult issues in the assessment of eating disorders. This fact has several implications because, although binge eating is one of the essential aspects of eating disorders, the definition of an episode is still not very clear with respect to its essential components as well as the accuracy of the estimation of food intake (Anderson, Lundgren, Shapiro & Paulosky, 2004). According to the DSM-IV-TR (APA, 2000), this disorder was characterized by recurrent episodes of dense food intake, eating more rapidly than normal when not physically hungry, until feeling uncomfortably full. These intakes are normally carried out alone, because of the shame associated with the exaggerated ingestion, and characterized by a lack of control, but without the compensatory behaviour present, as is the case in BN. This lack of control over eating, including a large amount of food intake in a limited period of time, clearly superior to what most people consume in a similar time period under the same circumstances, is usually followed by a feeling of anguish, self-disgust, depression, or guilt over the ingestion episode. In the cases where there were no criteria for Eating Disorder, these symptoms must be considered as an Eating Disorder Not Otherwise Specified (EDNOS).
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) presents some changes regarding the classification of eating disorders aiming to clarify criteria from the previous manual and reduce the high proportion of EDNOS (Call, Walsh & Attia, 2013). The category is now named feeding and eating disorders, and includes pica, rumination and avoidant/restrictive food intake, as well as AN, BN and BED (APA, 2013). These disorders are characterized, according to the manual, by a “persistent disturbance of eating or eating-related behaviour that results in the altered consumption or absorption of food and that significantly impairs physical health or psychosocial functioning” (p.329).
Some studies (Allen, Byrne, Oddy & Crosby, 2013; Flament et al., 2015; Lindvall Dahlgren, Wisting & Rø, 2017; Machado et al., 2013) revealed that with the DSM-5 classification criteria, the proportion of EDNOS diminished and the proportion of prevalence rates for Eating Disorders increases. These results provide evidence for the clinical utility of the DSM-5 for the diagnoses of eating disorders and that the DSM-5 criteria provides more specific diagnoses for eating disorder patients (Erzegovesi & Bellodi, 2016; Fisher, Gonzalez & Malizio, 2014).
Well established diagnostic criteria for mental disorders are essential to correctly assess and treat patients. Eating disorders are not an exception and some recommendations were made by Anderson and Maloney (2001) to improve the effectiveness of eating disorder treatments. These authors suggested a greater use of assessment measures of cognitive self-control as well as caloric restriction when assessing dietary restraint, so that all the core domains of the eating disorders would be assessed. Likewise, other authors (e.g., Anderson et al., 2004) recommended the use of well-validated measures and standardized instruments in all phases of the treatment process for eating disorders, particularly because the clinical assessment of eating disorders can be problematic. They refer that the central symptom domains of interest in eating disorders are: body weight, binge eating and compensatory behaviour, over concern with shape and weight, dietary restraint, body image disturbance and affective disturbance.
Regarding research, one of the obstacles to the progress in the investigation of eating disorders is the lack of validated measures for their study (Stice, Telch & Rizvi, 2000). There are few structured psychiatric interviews, such as the Eating Disorder Examination (Cooper & Fairburn, 1987), the Structured Clinical Interview for DSM (Spitzer, Williams, Gibbon & First, 1990) or the Interview for the Diagnosis of Eating Disorders-IV (Kutlesic, Williamson, Gleaves, Barbin & Murphy-Eberenz, 1998), but the fact that the self-report measures, such as the Eating Disorder Examination – Questionnaire (Fairburn & Beglin, 1994) or the Questionnaire for Eating Disorder Diagnosis (Mintz, O’Halloran, Mulholland & Schneider, 1997) do not include diagnosis for BED is also detrimental (Stice et al., 2000).
Some of the most used instruments in research are indeed screening measures, as the Eating Attitudes Test (EAT; Garner & Garfinkel, 1979; Garner, Olmsted, Bohr & Garfinkel, 1982), the Bulimia Test-Revised (BULIT-R; Thelen, Farmer, Wonderlich & Smith, 1991), the Eating Disorders Inventory – 3 (EDI-3; Garner, 2004), or the Setting Conditions for Anorexia Nervosa Scale (SCANS; Slade & Dewey, 1986).
Other instruments are directed to specific symptoms that are usually present in eating disorders, and are used as diagnostic criteria, such as The Body Shape Questionnaire (BSQ; Cooper, Taylor, Cooper & Fairburn, 1987; Santos & Baptista, 2004), the Restraint Scale (RS; Herman & Polivy, 1980), the Three Factor Eating Questionnaire Cognitive Restraint Scale (TFEQ-R; Stunkard & Messick, 1985), as well as the Dutch Eating Behaviour Questionnaire (DEBQ; Van Strien, Frijters, Bergers & Defares, 1986) that assesses restrained, emotional, and external eating behaviours. Another category of measures has the purpose of treatment planning and evaluation, such as the self-monitoring or the Multifactorial Assessment of Eating Disorder Symptoms (MAEDS; Anderson, Williamson, Duchman, Gleaves & Barbin, 1999).
There are few eating disorder measures validated for the Portuguese Population. The most well known are the Three-Factor Eating Questionnaire (Moreira, Almeida & Sampaio, 1999; Moreira, Almeida, Sampaio & Almeida, 1997; Stunkard & Messick, 1985), the Eating Disorder Inventory (Garner, Olmstead & Polivy, 1983; Machado, Gonçalves, Martins & Soares, 2001), the Dutch Eating Behavior Questionnaire (Van Strien, Frijters, Bergers & Defares, 1986; Viana & Sinde, 2003) and, more recently, the Eating Disorders Examination Questionnaire (Fairburn & Beglin, 1994; Machado et al., 2014).
This lack of validated measures for the Portuguese population and the need for a measure that can assess both diagnostic criteria and eating disorder symptomatology was the starting point for the aim of the present study.
Based on DSM-IV (APA, 2000), the Eating Disorder Diagnostic Scale (EDDS; Stice, Fisher & Martinez, 2004; Stice et al., 2000) is a measure that assesses the existence of diagnostic criteria for AN, BN and BED. The EDDS generates diagnoses for the threshold and sub-threshold eating disorders, as well as for an overall eating disorder symptom total score (Stice et al., 2000). This scale was introduced as a brief self-report questionnaire to be useful for etiological research and to fulfil the need for measures of eating pathology, for instance in prevention. The EDDS also aims at being suitable for a clinical setting in order to identify individuals with eating pathology (Stice et al., 2004) and to provide relevant information to ascertain DSM-5 criteria (Flament et al., 2015). Several studies (Chen & Jackson, 2008; Krabbenborg et al., 2012; Lee et al., 2007; Thorsteinsdottir & Ulfarsdottir, 2008) have been developed to confirm the adequacy of the EDDS in different populations and an exploratory factor analysis by Lee and co-workers revealed four dimensions: body dissatisfaction, bingeing behaviours, bingeing frequency, and frequency of compensatory behaviours (Lee et al., 2007).
The aim of this research was to study the structure and psychometric properties of the Eating Disorder Diagnostic Scale for the Portuguese Population. First, an exploratory factor analysis of the structure of the EDDS was conducted, followed by a confirmatory factor analysis. Finally, the reliability and validity of the resulting dimensions were evaluated.
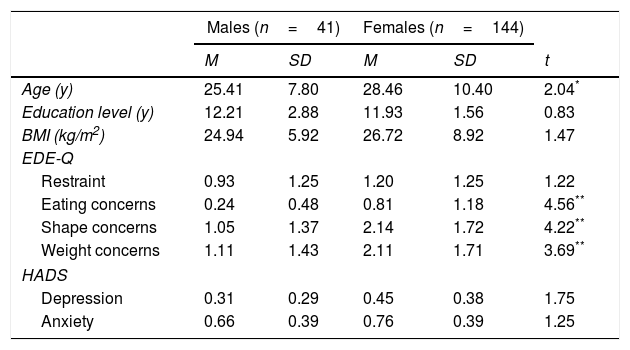
MethodParticipantsTo perform the Exploratory Factor Analysis (EFA), we used a sample of college students, who volunteered to take part in the study. There were a total of 185 participants, 144 females with a mean age of 28.46 (SD=10.40) and 41 males with a mean age of 25.41 (SD=7.80) years old. The mean body mass index (BMI) was of 26.72 (SD=8.92) for females and 24.94 (SD=5.92) for males. Participants with a BMI less than 17 were excluded from the sample.
Eating disorders, depression and anxiety symptoms were assessed. Women presented higher values of eating, shape and weight concerns. Nevertheless, the results did not present values of clinical disorders (see Table 1).
Means and standard deviations for age, body mass index, eating disorders, anxiety and depression symptoms (sample 1).
| Males (n=41) | Females (n=144) | ||||
|---|---|---|---|---|---|
| M | SD | M | SD | t | |
| Age (y) | 25.41 | 7.80 | 28.46 | 10.40 | 2.04* |
| Education level (y) | 12.21 | 2.88 | 11.93 | 1.56 | 0.83 |
| BMI (kg/m2) | 24.94 | 5.92 | 26.72 | 8.92 | 1.47 |
| EDE-Q | |||||
| Restraint | 0.93 | 1.25 | 1.20 | 1.25 | 1.22 |
| Eating concerns | 0.24 | 0.48 | 0.81 | 1.18 | 4.56** |
| Shape concerns | 1.05 | 1.37 | 2.14 | 1.72 | 4.22** |
| Weight concerns | 1.11 | 1.43 | 2.11 | 1.71 | 3.69** |
| HADS | |||||
| Depression | 0.31 | 0.29 | 0.45 | 0.38 | 1.75 |
| Anxiety | 0.66 | 0.39 | 0.76 | 0.39 | 1.25 |
BMI, Body Mass Index; EDE-Q, Eating Disorder Examination-Questionnaire; HADS, Hospital Anxiety and Depression Scale.
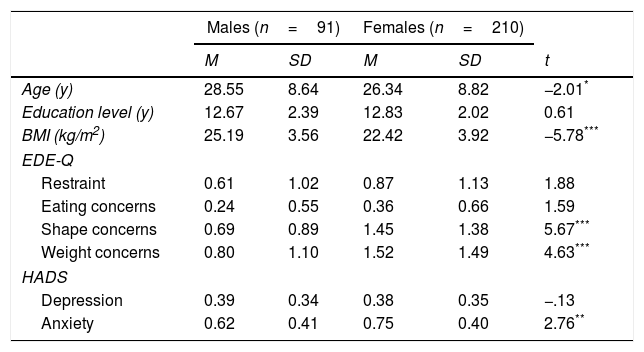
A second sample of 301 participants, also college students, was used to perform the Confirmatory Factor Analysis (CFA), with 91 males with a mean age of 28.55 (SD=8.64) years old and 210 females with a mean age of 26.34 (SD=8.82) years old. The mean BMI was 22.42 (SD=3.92) for females and 25.19 (SD=3.56) for males. Participants with a BMI under 17 were also excluded from this sample. Females presented more symptoms of shape and weight concerns as well as more symptoms of anxiety but, as for the first sample, those symptoms were not clinically relevant (see Table 3).
Both samples were part of a larger sample and the data was collected simultaneously. From the 486 initial participants, 185 were randomly selected to perform the EFA, allowing the fulfilment of EFA data selection criteria (Howard, 2016), as well as the recommendations of the Subjects-to-Variable Ratio 10:1 thumb rule. The rest of the sample was used to perform the CFA.
The two samples were compared in terms of the sociodemographic variables and there were statistically significant differences for the education level, t(482)=−2.90; p=.004, revealing that the participants in sample 2 presented a higher education level (M=12.78; DP=2.13) than participants from sample 1 (M=12.15; DP=2.65). No differences were found for the participants’ age, t(484)=0.87; p=.383, nor for gender distribution, χ2 (1)=3.77; p=.052.
MeasuresEating disorder symptoms. The Eating Disorder Diagnostic Scale (EDDS; Stice et al., 2000) is a measure, based on DSM-IV-TR (APA, 2000), which assesses the existence of diagnostic criteria for AN, BN and BED. It consists of 22 items with different response format, as follows: from question one to four individuals should respond in a seven-point response scale (0 – None to 6 – Extremely); questions 6, 7, 9, 10, 11, 12, 13, 14 and 22 are answered on a scale of dichotomous response (0 – No and 1 – Yes); question 7 is answered by the number of times a certain topic occurred; questions 8, 15, 16, 17 and 18 are answered by the number of times per week a certain topic occurred, questions 19 and 20 are open-response (weight and height), and item 21 is answered by the number of months in which a specific topic occurred. An overall eating disorder symptom score can be obtained by standardizing and summing up scores of all items (except for items assessing weight, height and birth control pill use). Higher scores are indicative of higher eating disorder psychopathology.
As for the psychometric properties, EDDS has a test–retest coefficient of .95 for the diagnosis of AN, and the total score of the scale has a value of .98. In the first week, the test–retest has a coefficient of .71 to BN and the total score a value of .91. The coefficient of test–retest was .75 for the diagnosis of BED and .89 for the total result of the value scale. Regarding the Internal Consistency of EDDS, Cronbach's alpha presented a value of .91 for the entire sample. Criterion validity revealed a coefficient reflecting agreement between the diagnosis done with the structured interview and EDDS, and was .93 for the AN, .81 for BN and .75 for the BED. Criterion validity was also assessed by agreement between the EDDS and the Eating Disorder Examination and the correlation between the two measures was .82 (Stice et al., 2004).
Anxiety and depression were assessed using the Anxiety Hospital Depression Scale (Zigmond & Snaith, 1983; translated and standardized to the Portuguese population by Pais-Ribeiro et al., 2007). This is a self-assessment measure, consisting of 14 items divided in two subscales: anxiety and depression. The score of the items is made with a response category of four points (0 to 3) with a maximum score of 21 for each scale. Values between 0 and 7 (in each scale) do not indicate anxiety or depression; results between 8 and 10 may be an indicator of mild anxiety or depression; values between 11 and 14 indicates moderate anxiety or depression; and values between 15 and 21 point to severe depression or anxiety. Regarding the psychometric qualities of the HADS, the scale presents high internal consistency, with a Cronbach's alpha of .76 for anxiety and .81 for depression. The temporal stability evaluated by test–retest method for an interval of one week, revealed Pearson coefficients of .75 for anxiety and depression (Pais-Ribeiro et al., 2007).
Eating disorders were evaluated using the Eating Disorder Examination Questionnaire (EDE-Q; Fairburn & Beglin, 1994). It is a self-assessment instrument, which measures the eating behaviours and their frequencies with respect to the last 28 days. It consists of 28 items, being the first 12 answered in a 7-point scale (0 – no day; 1 – 1–5 days; 2 – 6–12 days; 3 – 13–15 days; 4 – 16–22 days; 5 – 23–27 days; 6 – everyday). From the 13th up to the 18th item, responses are open. The 19th item is answered on a scale of 7 points (0 – no day; 1 – 1–5 days; 2 – 6–12 days; 3 – 13–15 days; 4 – 16–22 days; 5 – 23–27 days; 6 – every day), and the 20th item is answered according to a 6-point scale (0 – no to 6 – very). Finally, from the 21st to the 28th item we have a 6-point response format (0 – nothing to 6 – extremely). The EDE-Q assesses four dimensions: Restraint, Shape Concerns, Weight Concerns and Eating Concerns over the previous 28 days and a global score can be obtained by summing and averaging the subscale scores. Higher values are indicative of more eating disorder psychopathology. The temporal stability evaluated by test–retest method revealed coefficients ranging between .81 and .94. For the Portuguese population, in a high school sample Cronbach's alpha ranges from .72 for eating concern subscale to .94 for the global score, and for a college students’ sample, the internal consistency varies from .84 for weight concern to .97 for the global score. Results show it accurately discriminates between participants with and without an eating disorder (Machado et al., 2014).
ProcedureThe participants were informed that a study was taking place with the purpose of validating a measurement of Eating Behaviours and were asked if they would be available to participate in it as volunteers. They were informed that the protocol would take about 15–20min to complete. Participants who agreed to participate in the study were referred to a quiet place where they could fill in the questionnaires and the data was collected by the first author of the study. Participants were given an informed consent form, ensuring anonymity and data confidentiality, in accordance with the ethical standards of the Declaration of Helsinki. It was also referred that all data would be treated for statistical purposes at group level.
The instructions were given to the participants before filling the evaluation protocol and they were also asked some general socio-demographic questions (e.g., age). At the end of the study, they were thanked for their participation and any questions about the study were answered.
ResultsTo analyze the structure of the EDDS an EFA, for principal components method with Varimax rotation, was performed using SPSS Statistics (v 20). First, considering that the response format of EDDS is not the same for all items, we calculated the Z values. Subsequently, due to the existence of missing values, we created a database resulting from the correlation matrix. In addition, because the EDDS has different response formats, we computed the items in the Binge Eating Behavior Scale with dichotomic format (items 5, 6, 9,10,11,12,13,14) into a binge eating score (EDDS_BE) before carrying out the EFA.
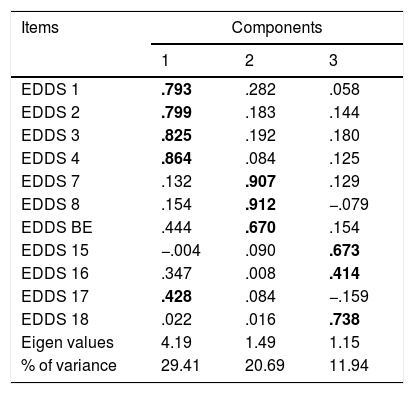
The results showed that for the total of the 11 items, three factors emerged (KMO=.746; p<.001) with eigenvalues >1, explaining 62.04% of the variance (see Table 2). The first component explained 29.41%, the second component explained 20.61% and the third component explained 11.94% of the total variance. Items loaded at least .79 for the first dimension (EDDS1-4) and evaluate body and weight concerns. In the second component (EDDS7-8 and EDDS-BE) items loaded from .67 to .91 and assess binge eating behaviours. The third and last component (EDDS 15, 16 and 18) had loadings from .41 to .71 and evaluated compensatory behaviours. Item EDDS 17's loading values suggest that this item belongs to the first component but the item content is related to the compensatory behaviours (third component). To clarify this result a Confirmatory Factor Analysis (CFA) was performed.
Exploratory factor analysis of the Eating Disorder Diagnostic Scale.
| Items | Components | ||
|---|---|---|---|
| 1 | 2 | 3 | |
| EDDS 1 | .793 | .282 | .058 |
| EDDS 2 | .799 | .183 | .144 |
| EDDS 3 | .825 | .192 | .180 |
| EDDS 4 | .864 | .084 | .125 |
| EDDS 7 | .132 | .907 | .129 |
| EDDS 8 | .154 | .912 | −.079 |
| EDDS BE | .444 | .670 | .154 |
| EDDS 15 | −.004 | .090 | .673 |
| EDDS 16 | .347 | .008 | .414 |
| EDDS 17 | .428 | .084 | −.159 |
| EDDS 18 | .022 | .016 | .738 |
| Eigen values | 4.19 | 1.49 | 1.15 |
| % of variance | 29.41 | 20.69 | 11.94 |
In bold, items assigned to each factor.
Means and standard deviations for age, body mass index, eating disorders, anxiety and depression symptoms (sample 2).
| Males (n=91) | Females (n=210) | ||||
|---|---|---|---|---|---|
| M | SD | M | SD | t | |
| Age (y) | 28.55 | 8.64 | 26.34 | 8.82 | −2.01* |
| Education level (y) | 12.67 | 2.39 | 12.83 | 2.02 | 0.61 |
| BMI (kg/m2) | 25.19 | 3.56 | 22.42 | 3.92 | −5.78*** |
| EDE-Q | |||||
| Restraint | 0.61 | 1.02 | 0.87 | 1.13 | 1.88 |
| Eating concerns | 0.24 | 0.55 | 0.36 | 0.66 | 1.59 |
| Shape concerns | 0.69 | 0.89 | 1.45 | 1.38 | 5.67*** |
| Weight concerns | 0.80 | 1.10 | 1.52 | 1.49 | 4.63*** |
| HADS | |||||
| Depression | 0.39 | 0.34 | 0.38 | 0.35 | −.13 |
| Anxiety | 0.62 | 0.41 | 0.75 | 0.40 | 2.76** |
BMI, Body Mass Index; EDE-Q, Eating Disorder Examination-Questionnaire; HADS, Hospital Anxiety and Depression Scale.
To accomplish the CFA we used the statistical program AMOS (v.7.0). To test the fit of the proposed model we analyzed the following fit indices: the chi-square (Bentler & Bonett, 1980), Comparative Fit Index, CFI (Bentler, 1988), the Root Mean Square Error approximation - RMSEA (Browne & Cudeck, 1993) and Goodness Index-of-fit-GFI (Jöreskog & Sörbom, 1996). The model fit would be confirmed if the χ2 value had an associated non significant p-value or if the ratio of the χ2 and degrees of freedom (χ2/df) were less than five and would also be considered adequate if the adequacy indicators of the theoretical models to the observed data, GFI and CFI, were higher than .90 (Kline, 1994) or if the RMSEA presented a value under .05 (Browne & Cudeck, 1993). All models were tested using covariance matrices and maximum-likelihood estimation methods.
The first model was based on the theory that sustains the diagnostic criteria for eating disorders (APA, 2000, 2013) and the results of previous studies (Lee et al., 2007). Although a four dimension model has been obtained in an exploratory analysis (Lee et al., 2007), the test of the factor structure of EDDS through a confirmatory factor analysis was based on the results of the EFA and in the DSM criteria. Lee and co-workers (2007) obtained four dimensions in their EFA: body dissatisfaction, bingeing behaviours, bingeing frequency, and frequency of compensatory behaviours. Based on these results and the content of the items, a three independent dimensions model with a Body and Weight Concerns subscale, a Binge Eating Behavior subscale and a Compensatory Behaviors subscale was proposed. It is our view that the two binge eating dimension (bingeing behaviours and bingeing frequency) corresponds to the same construct, hence only one binge eating dimension was proposed.
The first model tested represents the null model, which assumes there is a single underlying latent variable on which all of the eating symptoms load. This model was proposed to compare it to other models that reflect theoretically based hypothesis. Regarding the fit adjustment of the proposed model (see Fig. 1), the fit indices obtained (CFI=.50; GFI=.72; RMSEA=.22 and χ2=669.79, df=44, p=.230) indicate that this single latent model provides a poor fit for the data.
 of the Eating Disorder Diagnostic Scale.")
The second model tested considered the existence of three latent variables: Body and Weight Concerns, Binge Eating Behaviour and Compensatory Behaviours (see Fig. 2). The fit indices for this model gave values of CFI=.73; GFI=.82; RMSEA=.16 and χ2=385.85, df=44, p<.001. Although this represents a theoretically interpretable model, the three independent latent variables provide a poor fit for the data (χ2/df=8.77). These indicators suggest that changes should be performed into the second model (see Table 4). The covariance values revealed that some correlations should be taken into consideration and a third model was developed.
 of the Eating Disorder Diagnostic Scale.")
Model 3 tested the three latent variables considered in model 2, associated with a second order variable named Eating Disorder Symptoms (see Fig. 3). The model also incorporated the covariances between the errors of the items aggregated in the same dimension. Namely, in the Body and Weight Concerns dimension the errors of EDDS1 with EDDS2 (r=.63) and the errors of EDDS3 with EDDS4 (r=.70) were covariated. In the Binge Eating Behaviour dimension the errors of EDDS7 with EDDS8 (r=.61) were also covariated. No covariance between errors was performed for the Compensatory Behaviours dimension.
 of the Eating Disorder Diagnostic Scale with 2nd order factor.")
For this model of the EDDS all fit indices suggested an excellent fit: CFI=.99; GFI=.98; RMSEA=.02. When we investigated the tested models with scaled difference in chi-square tests (Brown, 2006; Satorra & Bentler, 1994), model 3 demonstrated significantly better fit, when compared with model 2, Δ χ2 (10, N=301)=346.13, p=.001 (see Table 4).
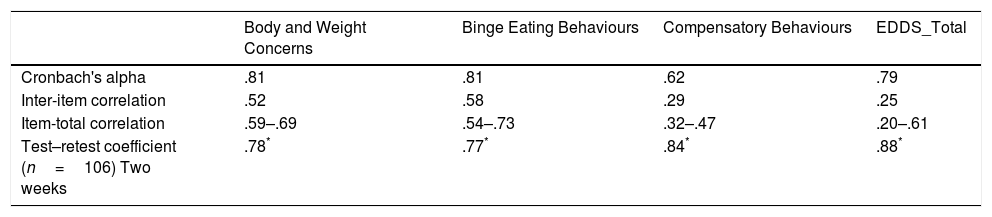
ReliabilityCronbach's alpha, inter-item correlations, and item-total scale correlations are presented in Table 5. Alpha coefficients were .79 for the total scale, and ranged from .62 to .81 for the subscales: .61 (Compensatory Behaviours), .81 (Binge Eating Behaviour) and .81 (Body and Weight Concerns). The inter-item correlations range from .25 for the total score of the EDDS to .58 for the Body and Weight Concerns subscale. In regards to the item-total correlations the results showed good homogeneity although some items revealed a lower relation than expected: .59 to .69 for Body and Weight Concerns, .54 to .73 for Binge Eating Behaviours, .32 to .47 for Compensatory Behaviours and .20 to .61 for the global score. These results suggest that the three subscales of the EDDS have good internal consistency.
Internal consistency and test retest reliability of the EDDS Subscales.
In order to confirm the temporal stability of the EDDS we performed a test–retest analysis. A Pearson correlation was performed over the results of 106 participants, tested with a two-week interval. The results ranged from .77, for the Binge Eating Behavior subscale, to .88, for the global score. Both results for internal consistency and for test–retest indicate that this is a measure with an adequate reliability.
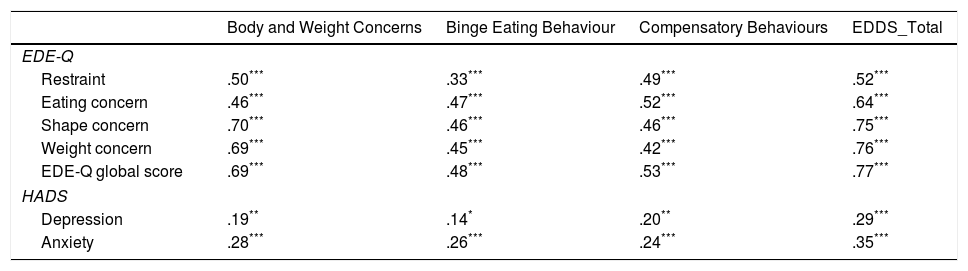
Convergent and discriminant validityTo evaluate the convergent and discriminant validity of the EDDS, we computed correlations between the EDDS subscales and other measures of eating disorders, anxiety and depression. The resulting correlations are presented in Table 6.
Intercorrelations between the EDDS Scales, the EDE-Q and HADS.
| Body and Weight Concerns | Binge Eating Behaviour | Compensatory Behaviours | EDDS_Total | |
|---|---|---|---|---|
| EDE-Q | ||||
| Restraint | .50*** | .33*** | .49*** | .52*** |
| Eating concern | .46*** | .47*** | .52*** | .64*** |
| Shape concern | .70*** | .46*** | .46*** | .75*** |
| Weight concern | .69*** | .45*** | .42*** | .76*** |
| EDE-Q global score | .69*** | .48*** | .53*** | .77*** |
| HADS | ||||
| Depression | .19** | .14* | .20** | .29*** |
| Anxiety | .28*** | .26*** | .24*** | .35*** |
EDDS, Eating Disorder Diagnostic Scale; EDE-Q, Eating Disorder Examination-Questionnaire; HADS, Hospital Anxiety and Depression Scale.
All the EDDS Total symptoms presented significantly moderate to high correlations with all the EDE-Q subscales scores (r>.59; p<.001) and a low correlation with anxiety (r=.35; p<.001) and depression (r=.24; p<.001). Similar results were found for the Body and Weight Concerns subscale with all the EDE-Q subscales (.46 to .70) and with anxiety (r=.28; p<.001) and depression (r=.19; p<.001), and for the Compensatory Behavior subscale with correlation results varying from .42 to .53 (p<.001) with the EDDS scales, and with depression (r=.20; p<.01) and anxiety (r=.24; p<.001). The Binge Eating Behavior scale was the one with significantly lower correlations with the EDDE-Q presenting values that range from .33 to .48 (p<.001), and with anxiety (r=.26; p<.001) and depression (r=.14; p<.05). In general, these results support the convergent and discriminant validity of the EDDS.
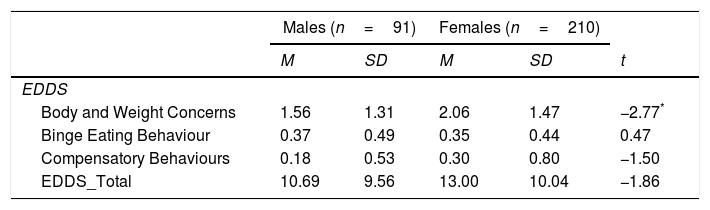
Normative dataTable 7 presents the means and standard deviations for the three subscales of the Eating Disorder Diagnostic Scale and the EDDS total symptoms score. An Independent-sample T test was performed in order to compare means between males and females, showing that women presented higher values of Body and Weight Concerns, t(299)=−2770; p<.01, than men. No differences were found for the other subscales between genders.
Means and standard deviations for the EDDS Scales.
| Males (n=91) | Females (n=210) | ||||
|---|---|---|---|---|---|
| M | SD | M | SD | t | |
| EDDS | |||||
| Body and Weight Concerns | 1.56 | 1.31 | 2.06 | 1.47 | −2.77* |
| Binge Eating Behaviour | 0.37 | 0.49 | 0.35 | 0.44 | 0.47 |
| Compensatory Behaviours | 0.18 | 0.53 | 0.30 | 0.80 | −1.50 |
| EDDS_Total | 10.69 | 9.56 | 13.00 | 10.04 | −1.86 |
EDDS, Eating Disorder Diagnostic Scale.
The purpose of this study was two-fold, to study the factorial structure and evaluate the psychometric properties of the Eating Disorder Diagnostic Scale for the Portuguese Population, and at the same time to analyze the theoretical constructs (latent variables) proposed by the authors of the Eating Disorders Diagnosis Scale and the validity of the measured items.
The EFA revealed that the EDDS can be organized into three logical dimensions: Body and Weight Concerns, Binge Eating Behaviour and Compensatory Behaviours. These results are partially in accordance with the ones found by Lee and colleagues (2007) which revealed four dimensions: body dissatisfaction, bingeing behaviours, bingeing frequency, and frequency of compensatory behaviours. In their study the authors presented two dimensions of binge eating whereas in the present study only one Binge Eating Behaviour scale was revealed. As we previously mentioned we consider that the two binge eating dimensions evaluate the same construct; hence only one binge eating dimension was taken into account.
In general, CFAs indicated that the factor structures of these EDDS scales are coherent with the literature on Eating Disorders and the content of the Eating Disorder Diagnostic Scale items. Thus, the model with three factors (Body and Weight Concerns, Binge Eating Behaviour, and Compensatory Behaviours) with a second order variable (eating disorder symptoms) was proven to be the one that better corresponded to our data. However, it should be noted that although the general pattern was good, some of the observed variables showed a weak relationship with the latent variables, and the variable Compensatory Behaviours revealed a low relationship with the second-order variable. The theory relates the different constructs as the cause for the maintenance of eating disorders (Fairburn, Marcus & Wilson, 1993), however, and more specifically regarding the Compensatory Behaviours variable, which refers to different methods (vomiting induction, laxatives/diuretics, fasting and physical activity), it might be interesting in future studies to consider each item as an observable variable of a second order and not as a set of observed variables to a latent variable.
The proposed three-factor model corresponds to the main categories of eating disorders, and it should be emphasized that the main goal of the EDDS is not only to diagnose eating disorders, but also to identify subclinical groups. In fact, the detection of people within a risk zone is very important, both for possibility of doing research studies with non-diagnosed participants, but principally for the opportunity of directing prevention interventions to these sub-clinical groups. In fact, validated measures and reliable instruments can be important not only to detect and diagnose clinical and sub-clinical groups, but also to follow possible improvements of interventions or treatment processes (c.f., Anderson et al., 2004). At the same time, research on eating disorders depends on the existence of reliable and valid measures (e.g., Stice et al., 2000), therefore an instrument like the EDDS is mostly valuable, and it is important to empirically test and validate it in different populations, as has been done with a Portuguese sample.
Finally, the fact that DSM-5 (APA, 2013) is now available should be taken into account and used as a reference for the eating disorders diagnostic criteria. Although EDDS was developed based on DSM-IV-TR and most of the criteria are identical for eating disorder in both manuals, some changes have in fact been made and should be taken into consideration for next studies. It is our purpose to adapt this EDDS version to the new diagnostic criteria and try to replicate the adequacy of the psychometric properties of the measure.
Conflicts of interestThe authors declare no conflicts of interest.