







Survival analysis of patients with prostate cancer (PCa) with adverse prognostic factors (APF) treated with radical prostatectomy (RP) and salvage radiotherapy (SRT) after biochemical recurrence (BR) or biochemical persistence (BP).
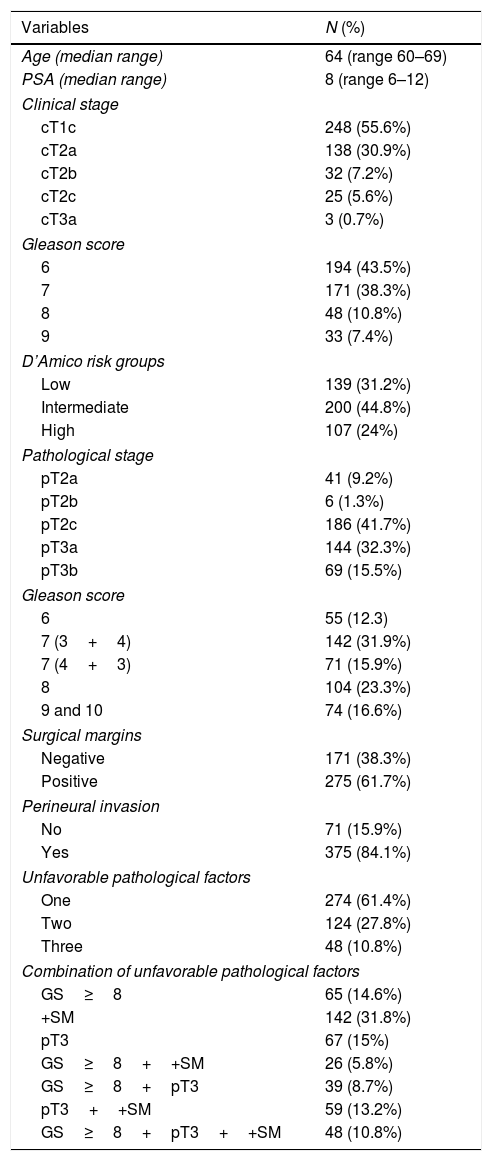
Materials and methodsRetrospective analysis of 446 patients with at least one of the following APF: Gleason score ≥8, pathologic stage ≥pT3 and/or positive surgical margins. BR criteria used was PSA level over 0.4ng/ml.
A survival analysis using Kaplan–Meier was performed to compare the different variable categories with log-rank test. In order to identify risk factors for SRT response and cancer specific survival (CSS) we performed univariate and multivariate analyses using Cox regression.
ResultsMean follow up: 72 (IQR 27–122) months, mean time to BR: 42 (IQR 20–112) months, mean PSA level at BR: 0.56 (IQR 0.42–0.96). BR was present in 36.3% of the patients. Biochemical response to SRT was observed in 121 (75.7%) patients.
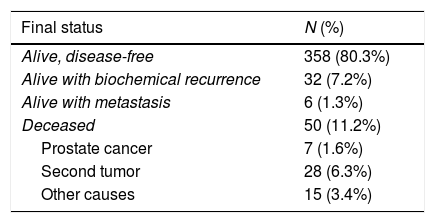
Recurrence-free survival (RFS) rates after SRT at 3, 5, 8 and 10 years were 95.7%, 92.3%, 87.9%, and 85%; overall survival (OS) rates after 5, 10 and 15 years was 95.6%, 86.5% and 73.5%, respectively. CSS rates at 5, 10 and 15 years were 99.1%, 98.1% and 96.6%.
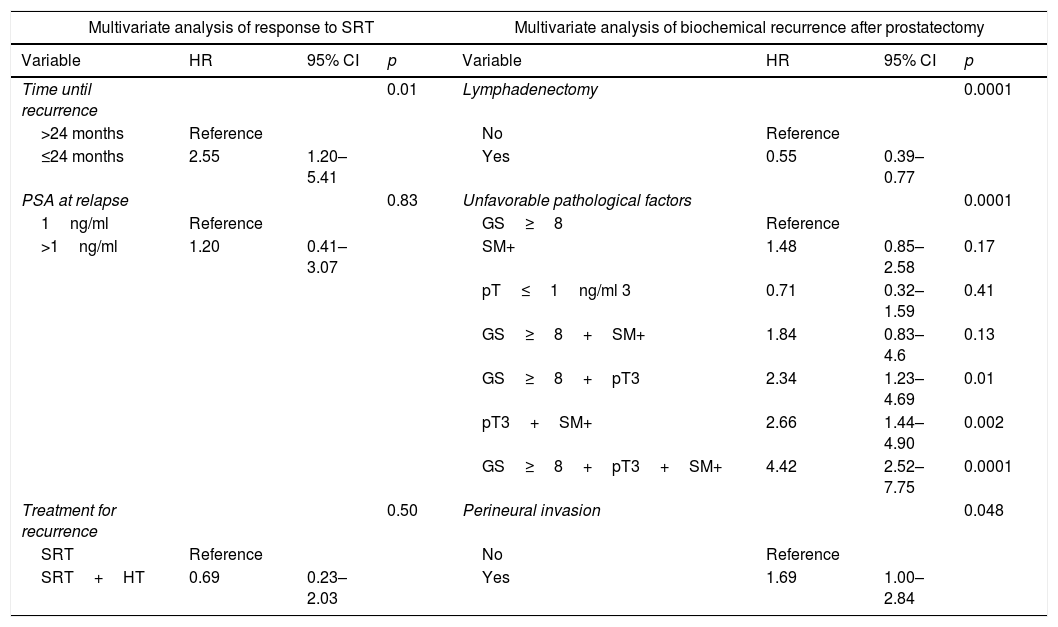
Only time to BR <24 months (HR=2.55, p=.01) was identified as an independent risk factor for RFS after SRT.
ConclusionsIn these patients, RP only controls the disease in approximately half of the cases. Multimodal sequential treatment (RP+SRT when needed) increases this control, achieving high CSS rates and biochemical control in over 87% of the patients. Patients with time to recurrence >24 months responded better to rescue treatment.
Analizar la supervivencia de los pacientes con cáncer de próstata (CP) con factores pronósticos desfavorables (FPD) tratados con PR y radioterapia de rescate (RTR) tras recidiva bioquímica (RB) y persistencia bioquímica (PB).
Material y métodoAnálisis retrospectivo de 446 pacientes con al menos uno de los siguientes FPD: score de Gleason ≥8, estadio patológico ≥pT3 y/o márgenes quirúrgicos positivos (MQ+). El criterio de RB fue la elevación del PSA por encima de 0,4ng/ml.
Evaluación de supervivencia mediante Kaplan-Meier y log-rank. Para identificar factores de riesgo con posible influencia en la respuesta a RTR y la supervivencia causa-específica (SCE) se usó análisis uni y multivariable (regresión de Cox).
ResultadosMediana de seguimiento: 72 (rango 37-122) meses, mediana de tiempo hasta RB: 42 (rango 20-112) meses. El 36,3% presentaron RB. Presentaron respuesta bioquímica a la RTR 121 (74,7%) pacientes.
La supervivencia libre de recaída (SLR) después de la RTR a los 3, 5, 8 y 10 años fue del 95,7, del 92,3, del 87,9 y del 85%, la SG a los 5, 10 y 15 años fue del 95,6, del 86,5 y del 73,5%. La SCE a los 5, 10 y 15 años fue del 99,1, del 98,1 y del 96,6%, respectivamente.
Solo el tiempo hasta la RB <24 meses (HR=2,55, p=0,01) se comportó como un factor predictor independiente de SLR después de RTR.
ConclusionesLa PR solo consigue control de la enfermedad a los 10 años en aproximadamente la mitad de los casos. El tratamiento multimodal secuencial (PR+RTR cuando precise) aumenta este control bioquímico hasta >87%, lográndose una larga SCE. Los pacientes con un tiempo hasta recidiva >24 meses respondieron mejor al tratamiento de rescate.
