






The assessment of the vestibulo-ocular reflex (VOR) is one of the main steps in clinically evaluating patients with dizziness. It can be performed at the bedside with common head-impulse test in which eye position is analysed at the end of the head-thrust. It is an important test due to its high specificity but low sensitivity.
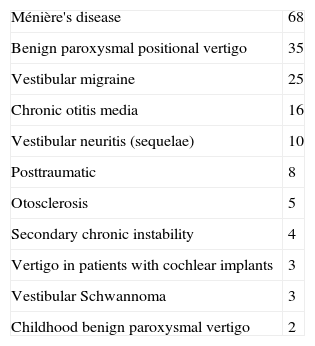
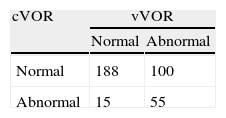
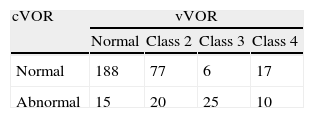
Material and methodsWe studied 179 patients with different types of balance-affecting disorders. The results were analysed in contingency tables. The clinical test was classified as normal or abnormal according to the absence or existence, respectively, of fixation saccades once the head-thrust was finished. The video head-impulse test (vHIT) was classified according to vestibulo-ocular reflex (VOR) gain and presence of fixation saccades. The speed of the slow phase of spontaneous nystagmus was also quantified, in addition to the caloric test results.
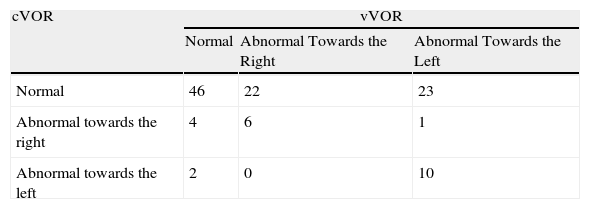
ResultsThere were significant differences (Chi-square test, P=.00) for the findings in the clinical evaluation and with the vHIT: 32.1% of the tests performed yielded different findings in both tests. In the vHIT, the differences were due to the finding of normal gain with saccades; in these patients, the mean canal paresis was significantly abnormal: 39%±10%.
ConclusionsThe distribution of findings for the VOR bedside examination and for that with the help of a video system are significantly different; as such, the video head-impulse examination is not simply an added VOR detection and registration system. The difference relies mainly on a vHIT response characterised as of normal gain but with fixation saccades. These have been considered as the cause for the low sensitivity of the bedside VOR examination and sometimes regarded as normal responses; we have demonstrated that these findings are abnormal according to the findings of higher canal paresis in the caloric test.
El estudio del reflejo vestíbulo-oculomotor (RVO) es uno de los pasos más importantes en la evaluación del paciente con cualquier alteración del equilibrio. Se puede realizar de forma clínica mediante impulsos cefálicos analizando la posición ocular final refleja y es una prueba de gran valor en la cabecera del paciente por su alta especificidad a pesar de su baja sensibilidad. En este trabajo vamos a comparar los resultados de esta valoración con los de una nueva metodología basada en el registro videoasistido del desplazamiento ocular inducido por el impulso cefálico.
Material y métodosEl trabajo se realiza en 179 pacientes con diferentes tipos de trastornos del equilibrio. Se hace un estudio por medio de tablas de contingencia de los resultados de los impulsos cefálicos a derecha e izquierda en cada paciente. Los resultados de cada prueba se clasifican en normales y anormales. El estudio clínico es anormal cuando se detectan sacadas de refijación al finalizar el impulso cefálico y el estudio videoasistido se clasifica de acuerdo a los parámetros de ganancia del reflejo y a la existencia de sacadas de refijación. Adicionalmente se estudia la intensidad del nistagmo espontáneo y el resultado en la prueba calórica.
ResultadosEn el 32,1% de las pruebas realizadas existe disparidad de resultados y esta diferencia es debida fundamentalmente a un patrón de respuesta analizada en el estudio videoasistido caracterizado por una ganancia normal y sacadas de refijación de moderada velocidad intermedias entre las encubiertas y las evidentes. Esto no es un patrón normal, toda vez que en la prueba calórica se observó que el valor promedio de la paresia canalicular es anormal: 39%±10.
ConclusionesLos hallazgos en este nuevo método de exploración amplían los del estudio clínico: no es un mero aditamento a la exploración clínica. La causa fundamental de la baja sensibilidad de la prueba clínica se basa en la incapacidad de detectar o, en dar como normal, pequeñas sacadas de refijación: representan la secuela de un daño vestibular precedente o actual y necesita una mejor caracterización.