





The Health of the Nation Outcome Scales for People with Learning Disabilities (HoNOS-LD) is a brief instrument that assesses functioning in people with intellectual development disorder and mental health problems/behaviour disorders. The aim of the present study was to examine the evidence on the validity of the scores based on the Spanish version of the HoNOS-LD.
Material and methodsThe study included 111 participants that were assessed by the Spanish version of the HoNOS-LD and other questionnaires that measured different variables related to the scale. Thirty-three participants were assessed by 2 examiners, and retested 7 days later, in order to study inter-examiner reliability and test–retest reliabilities.
ResultsBased on clinical and conceptual criteria, and on the results of the parallel analysis, a factorial solution with one factor was selected. Internal consistency was good (Omega coefficient of 0.87). Inter-examiner and test–retest reliabilities were excellent (intraclass correlation coefficients of 0.95 and 0.98, respectively). Correlations between sections of the HoNOS-LD and the related instruments showed the expected direction, and were highly significant (p<.001), and the HoNOS-LD score increased with the intensity of the support required by the participants. These results showed evidence of the validity of association with other external variables.
ConclusionsThe Spanish version of the HoNOS-LD is a brief, valid and reliable instrument, which will enable a routine assessment of functioning for different uses, including diagnosis and intervention.
La escala Health of the Nation Outcome Scales for People with Learning Disabilities (HoNOS-LD) fue creada para evaluar de forma breve el funcionamiento de las personas con trastorno de desarrollo intelectual y problemas de salud mental/trastornos de conducta. El objetivo del presente trabajo fue estudiar las evidencias sobre la validez de las puntuaciones obtenidas con la escala HoNOS-LD traducida al castellano.
Material y métodosLa muestra estaba formada por 111 participantes que fueron evaluados con la HoNOS-LD traducida al castellano y otros cuestionarios relacionados. Para estudiar la fiabilidad entre examinadores y la fiabilidad test–retest, 33 participantes fueron evaluados por 2 examinadores y reevaluados al cabo de 7 días.
ResultadosDe acuerdo con criterios clínicos y conceptuales, y con el resultado del análisis paralelo, se seleccionó una solución factorial con único factor. La consistencia interna fue buena (coeficiente omega de 0,87). Las fiabilidades entre examinadores y test–retest fueron excelentes (coeficientes de correlación intraclase de 0,95 y 0,98, respectivamente). Las correlaciones entre secciones de la HoNOS-LD y los instrumentos relacionados fueron en el sentido esperado y altamente significativas (p<0,001), y la puntuación HoNOS-LD aumentaba con el nivel de apoyos necesario de los participantes, resultados que aportaron evidencia sobre la validez de asociación con otras variables externas.
ConclusionesLa versión en castellano de la HoNOS-LD representa un instrumento breve, válido y fiable, que permitirá la evaluación rutinaria del funcionamiento con distintas finalidades, incluyendo el diagnóstico y la intervención.
According to the new diagnostic criteria of the DSM-5,1 intellectual development disorder (IDD) involves limitations both in intellectual functioning and in adaptive behaviour. Epidemiological studies indicate that the prevalence of psychiatric and behavioural disorders in people with IDD is the same if not greater than in the general population.2
The concept of dual or comorbid diagnosis means that clinicians must not only have sufficient clinical skills but also the necessary psychopathological tests to evaluate the entire range of mental illness and its different manifestations in people with IDD. However, the most relevant research into this phenomenon evidences a tendency to under diagnose mental disorders in this group. There are a great many people with IDD that do not receive an appropriate psychopathological diagnosis even when they present with a mental disorder. As a consequence, there is no specific treatment, and outcomes tend to be compromised.3 This phenomenon is further complicated in some cases that lack even a diagnosis to explain the learning disability; for example when the IDD is syndromic. A high proportion of people with IDD will have psychiatric and/or behavioural disorders, therefore genetic testing is recommended when we are faced with dysmorphic features in the context of a learning disability of unknown origin and behavioural or psychiatric alterations.4
These errors in diagnosis can be due to a known problem such as diagnostic overshadowing.5 This term refers to cases where IDD reduces the diagnostic significance of an accompanying behavioural problem: the symptoms of the mental illness are overshadowed in people with IDD. There are several explanations for this phenomenon. This is due in large part to the restricted ability of the patient to observe and describe their own behaviour and condition, as a consequence of cognitive impairment and its semiotics (limited reasoning capacity, linguistic and communication problems, etc.). Moreover, additional deficits such as severe sensory deficits or autistic spectrum disorder profiles associated with the IDD,6 impede the typical expression of the features of the disorder, resulting in diagnostic errors. Thus, for example, depression tends to manifest in the form of behavioural equivalents such as aggression, shrieking and/or self harm.7 In addition, it can be difficult to distinguish between some manifestations associated with certain stages of brain maturation (magical thoughts or invisible friends) and thought disorders in people of chronically advanced age but with clearly younger mental ages.8 Finally, in the population without disabilities mental health problems interfere with the most complex adaptive skills, which will not be possible to observe in people with IDD due to the level of cognitive impairment itself.9 Psychopathological assessment in the area of IDD must take all these particular considerations into account.
In line with the above, it is essential to study changes in the baseline functioning of the individual to identify the onset of mental illness in people with IDD. For example, people who require extensive support and who have little or no ability to communicate clearly have difficulty communicating their moods, therefore it is necessary to look out for the onset of behavioural changes (challenging behaviours essentially) and biological changes (impaired sleep and/or appetite).7 Monitoring functioning is also useful in evaluating the success or failure of an intervention. Efficient action should not only bring about a remission of the specific symptoms of the disorder, but it should improve the functioning of the individual in different areas including general health, adaptive skills and social relationships. Like the clinical aspects, functioning should be measured in a standardised way, with valid and reliable tools. Thus, consistent longitudinal measures that are sensitive to the onset of changes can be obtained, and the influence of individual features, types of intervention and adequacy of the health services can be studied.
The correct assessment of the functioning of people with IDD and mental health problems has not always received the attention it deserves. Authors such as Matson et al.10 stated that most pharmacological studies carried out on this group rarely evaluated the effects of medication beyond the symptoms of the disorder itself. To address this shortcoming, Roy et al.11 adapted a tool for assessing functioning in people from the general population with mental health problems (Health of the Nation Outcome Scales [HoNOS])12 for use in people with IDD. The new version was called Health of the Nation Outcome Scales for People with Learning Disabilities (HoNOS-LD).11
Like the original version, the HoNOS-LD is a brief instrument that determines general functioning taking into account various aspects, such as challenging behaviours, cognitive and physical impairment, psychiatric symptoms, adaptive skills and social relationships. In addition, and according to the findings of a study that used the original HoNOS scale on people with IDD over the age of 50 years,13 the HoNOS-LD scale covers challenging behaviours and cognitive and communication difficulties more specifically. There are no scales with the specificity features of the HoNOS-LD, because its design and content form a compendium of the various aspects associated with the clinical problems arising not only from the IDD itself, but also from the features of the cognitive impairment, psychiatric alterations and behavioural disorders. The HoNOS-LD covers areas in reality that other scales measure specifically. In this regard, it includes items to assess mental illness, resembling the Psychiatric Assessment Schedule for Adults with Developmental Disabilities,14 to assess adaptive skills, comparable to the Vineland Adaptive behaviour Scales,15 the presence of behavioural alterations, comparable to the Aberrant Behaviour Checklist (ABC),16 and social functioning, like the Social Functioning Scale for the Mentally Handicapped.17 In its validation study, the HoNOS-LD scale proved sensitive to change and obtained good psychometric indicators.11 Tenneij et al.18 compared the HoNOS and HoNOS-LD scales (Dutch versions) in a sample of people with IDD and mental health and/or behavioural problems. These authors concluded that the HoNOS-LD scale was the most suitable for evaluating people with IDD, since it had better psychometric properties and, on a qualitative level, examiners would prefer the operational definitions of the items of this scale. Finally, this instrument has been used in a significant number of studies to assess the efficacy of interventions,19–21 determine the quality of specialist IDD services,22–24 and compare people according to their clinical features.25
The general aim of this study was to study the evidence on the validity of the scores obtained using the HoNOS-LD scale translated into Spanish, studying the psychometric properties of its scores in a sample of people with IDD and mental health problems and/or behavioural disorders. More specifically, we aimed to analyse the internal structure of the scores achieved with the new tool, assess its internal consistency and its test–retest and inter-examiner reliability, as well as studying its association with other external variables (scores of other instruments used to measure related constructs – convergent validation – and level of support required by the participants – retrospective criterion validation). It was hypothesised that the internal structure of the scores obtained with the Spanish version of the HoNOS-LD scale would be similar to that of the original instrument, and that these scores would present good indices of internal consistency, test–retest reliability and interexaminer reliability. Furthermore, the scores significantly correlated with those of the other instruments that measure related constructs, and would vary significantly according to the level of support required by the participants.
Material and methodsParticipantsNon-probabilistic convenience sampling was performed among the users of the Mental Health and Intellectual Disability Specialist Department (SESM-DI) of the Institut d’Assistència Sanitària (IAS) of Girona. One hundred and eleven adults (≥18 years) were included of both sexes, with IDD and diagnosed with a psychiatric and/or behavioural disorder. The DSM-51 criteria were used to diagnose IDD and the Diagnostic Criteria for Psychiatric Disorders for Use with Adults with Learning Disabilities26 for diagnosing dual disease. The sample comprised different levels of support according to the categories established in DSM-5. All the participants had to sign their informed assent or consent (according to whether they had legal protection) and the informed consent of the family member or legal representative was also necessary.
Participants with nervous system disorders not related to IDD were excluded from the study (for example, head trauma, cerebrovascular accident, brain tumour or multiple sclerosis), substance abuse or untreated diseases associated with a cognitive deficit (for example, hypothyroidism, vitamin B12 deficiency or diabetes mellitus).
ProcedureA validation study was undertaken using an observational, cross-sectional design. Firstly the scale was translated and then back-translated by 2 independent translators, related to the field of psychopathology and belonging to the SESM-DI (IAS, Girona) and the Department of Developmental and Educational Psychology (Faculty of Education, Complutense University of Madrid). The list for quality control of translation-adaptation of psychometric instruments was used for the translation.27 Once the Spanish version was obtained, an expert in psychopathology and research with broad experience of clinical evaluation was asked to revise it, also belonging to the SESM-DI (IAS, Girona). Tests were then performed on functioning using the translated version of the scale, applied by several professionals to 10 patients to confirm the suitability of the translation. The majority of the items were observed to function appropriately and only one grammatical change was necessary. Thus the translation process met the directives set by the International Test Commission.28
The data were collected in 2 sessions of approximately 45min. The data were gathered from the HoNOS-LD scale and from other instruments to complete the convergent validation (see the section on Instruments). To study the interexaminer reliability, 33 participants were assessed by the principal examiner and a second examiner, both specialists in the psychopathological evaluation of people with IDD. In addition, these 33 patients were reassessed under the same conditions 7 days later, to obtain data on the test–retest reliability. All the assessments were performed by psychologists who specialised in dealing with people with IDD and belonged to the SESM-DI, during the first hours of the morning and under appropriate conditions.
Potential participants were informed of the study and those that made up the final sample gave their informed consent/assent. The participants received no form of incentive for taking part in the study. Once they had been informed, most of the patients and their family members agreed to participate. Only 3 decided not to participate. The clinical history and all the questionnaires answered by the participants were coded to ensure their anonymity, complying with the Law on Data Protection. The progress of the study was supervised at all times by the principal researcher, ensuring compliance with the principles of the Declaration of Helsinki. The protocol was approved by the Clinical Research Ethics Committee of the IAS.
InstrumentsHealth of the Nation Outcome Scales for People with Learning Disabilities11This comprises 18 items grouped into different sections: (a) challenging behaviours (items 1–3); (b) cognition (items 4–7); (c) clinical problems (items 8–13), and (d) adaptive skills and social relationships (items 14–18). The mental health professional conducts the assessment in relation to the functioning observed during the last month with the help of an informer. Each item was scored from 0 to 4: “0” means the absence of functioning problems, while “4” means these problems are more severe. The scores of the scale range from 0 and 72 (the higher the score, the poorer the functioning). It is important to highlight that the scale does not attempt to evaluate the functioning “potential”, but rather the level of real functioning, bearing in mind the impact of the support received by the individual.
Aberrant Behaviour Checklist16A scale comprising a total of 58 items corresponding to 5 subscales: agitation, lethargy and social isolation, stereotyped behaviours, hyperactivity and loquacity (internal consistency indices of .92, .95, .92, .94 and .85, respectively). In the clinical area it is used to assess challenging behaviours and changes to these behaviours as the result of an intervention. The majority of the studies on the effects of treatments have shown this scale to be sensitive to behavioural changes.29
Kaufman Brief Intelligence Test30Intelligence test comprising 2 subscales, one assesses crystallised intelligence (vocabulary, internal consistency=.93, test–retest reliability=.98), and the other assesses fluid thinking (matrices, internal consistency=.94, test–retest reliability=.97). It also provides a global intelligence index (internal consistency=.94, test–retest reliability=.98). Its standard lowest score of 40 is one of the lowest of the brief tests that determine intelligence quotient.
Mini psychiatric assessment schedule for adults with developmental disabilities14,31A screening tool that assess the presence and severity of psychiatric symptoms in people with IDD who require limited or intermittent support and who have verbal language. It provides scores for 7 categories of mental disorders. Exceeding a certain cut-off point implies the potential presence of a disorder and advises a more detailed clinical assessment. The indices of the intraclass correlation coefficient (ICC) for the total scores and for the definition indices varied between .82 and .84. The interdiagnostic reliability was .62.
Diagnostic assessment for the severely handicapped-II32A screening tool that assessments psychopathology in adults with IDD with extensive or pervasive support needs. It is divided into 13 subscales that evaluate frequency, duration and levels of severity of different psychiatric disorders. The internal consistency ranged between .20 and .84 for the 13 subscales.
Adaptive behaviour scale-residential and community, second edition33Scale used to assess adaptive behaviour. The first part evaluates the skills needed to achieve personal independence and responsibility in daily living (internal consistency=.91). The second part evaluates social skills (internal consistency=.80). The skills in the first part are distributed into 10 domains and 21 subdomains, and those of the second part are grouped into 8 domains. Once the scale has been administered, the skills of each person in each domain are noted and their performance is compared with that of their normative group.
Data analysisThe demographic variables of the sample and the instrument scores were analysed using frequencies and percentages or quartiles (since the variables did not present normal distributions), according to whether they were of a categorical or quantitative nature. The internal structure of the HoNOS-LD scores was studied using an exploratory factor analysis by ordinary least squares. Given the ordinal nature of the items, the analysis was based on a matrix of polychoric correlations.34 The distributions of the scores of each of the items were visually inspected and their asymmetry and kurtosis indices calculated beforehand. Selection of the number of factors to retain was based on theoretical criteria and on the result of a parallel analysis.35 The internal consistency of the scores was assessed using the omega coefficient, which is appropriate for analysing variables based on Likert-type response scales.36 The interexaminer reliability and the test–retest reliability were calculated using ICC. The convergent validation was conducted using a series of Spearman's correlations between the scores of the different sections of the HoNOS-LD scale and the scores of the other instruments used to measure related constructs. From a clinical perspective, the scores of the subscales of the instruments used are more informative than the total scores. Nevertheless, the total scores generally quantify the different underlying constructs, and therefore are used to perform the correlations. To be specific, the scores of the sections of the HoNOS-LD, such as (a) challenging behaviours; (b) cognition; (c) clinical problems, and (d) adaptive skills and social relationships, were correlated with the total scores of the ABC, Kaufman Brief Intelligence Test, Mini Psychiatric Assessment Schedule for Adults with Developmental Disabilities/Diagnostic Assessment for the Severely Handicapped and Adaptive Behaviour Scale-Residential and Community, second edition, respectively. The criteria validation was analysed using the non-parametric Kruskal–Wallis test, with the level of support necessary for categorising the IDD (intermittent, limited, extensive, and pervasive) as the independent variable and the HoNOS-LD score as the dependent variable. The bilateral level of statistical significance used in all the tests was .05 (except when multiple comparisons were made and the level of statistical significance was adjusted using Bonferroni's correction) and the effect size was calculated using Pearson's correlation. The set of data from the study showed no lost value. The analyses were performed using SPSS 19 (SPSS Inc., Chicago, IL, U.S.A.). The factor structure and the internal consistency of the scores were analysed using FACTOR (Lorenzo-Seva).37
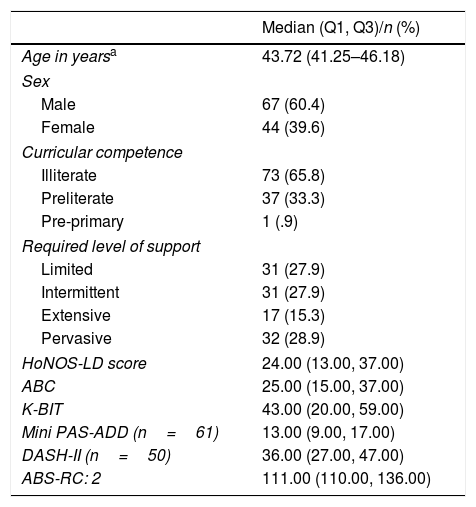
ResultsBasic description of the sample and scores of the scalesTable 1 shows the demographic variables and the quartiles of the overall scores of the tools used in this study.
Basic features of the sample (n=111).
| Median (Q1, Q3)/n (%) | |
|---|---|
| Age in yearsa | 43.72 (41.25–46.18) |
| Sex | |
| Male | 67 (60.4) |
| Female | 44 (39.6) |
| Curricular competence | |
| Illiterate | 73 (65.8) |
| Preliterate | 37 (33.3) |
| Pre-primary | 1 (.9) |
| Required level of support | |
| Limited | 31 (27.9) |
| Intermittent | 31 (27.9) |
| Extensive | 17 (15.3) |
| Pervasive | 32 (28.9) |
| HoNOS-LD score | 24.00 (13.00, 37.00) |
| ABC | 25.00 (15.00, 37.00) |
| K-BIT | 43.00 (20.00, 59.00) |
| Mini PAS-ADD (n=61) | 13.00 (9.00, 17.00) |
| DASH-II (n=50) | 36.00 (27.00, 47.00) |
| ABS-RC: 2 | 111.00 (110.00, 136.00) |
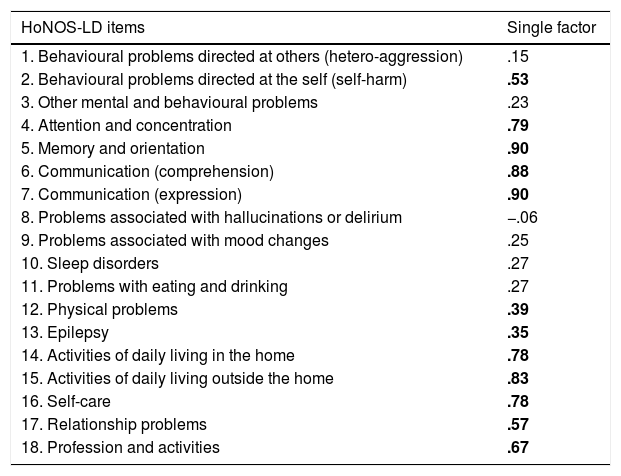
Some items of the HoNOS-LD scale presented scores with leptokurtic and asymmetric distributions towards the right. For these items, most of the participants had selected the lowest response options on the ordinal scale (equivalent to few problems with functioning). Bartlett's sphericity test – χ2 (153)=1009.70, p<.001 – indicated that the correlation between the scores of the items was sufficiently large, and the Kaiser–Meyer–Olkin index (.86), indicated that there was a good grade of joint relationship between the variables. Based on theoretical criteria and on the result of the parallel analysis, a single factor was extracted that, with an eigenvalue of 9.65, explained 38.6% of the variance. Table 2 shows the factor solution obtained. Two-thirds of the items had factor weights above the criterion of. 30.38 Items 1 (behavioural problems directed at others) and 8 (problems associated with hallucinations or delirium) had particularly low factor weights (.15 and −. 06, respectively). However, bearing in mind the importance of evaluating these aspects when determining the functioning of people with IDD and mental health problems, we opted to keep these 2 items. Finally, the value of the residual root mean square was. 16, above the criterion proposed by Kelley39 (in this case, .10), and the GFI index was .96, below the criterion of .95.40 Based on these values, the factor model fit cannot be considered good.
Factor structure of the Spanish version of the HoNOS-LD scale.
| HoNOS-LD items | Single factor |
|---|---|
| 1. Behavioural problems directed at others (hetero-aggression) | .15 |
| 2. Behavioural problems directed at the self (self-harm) | .53 |
| 3. Other mental and behavioural problems | .23 |
| 4. Attention and concentration | .79 |
| 5. Memory and orientation | .90 |
| 6. Communication (comprehension) | .88 |
| 7. Communication (expression) | .90 |
| 8. Problems associated with hallucinations or delirium | −.06 |
| 9. Problems associated with mood changes | .25 |
| 10. Sleep disorders | .27 |
| 11. Problems with eating and drinking | .27 |
| 12. Physical problems | .39 |
| 13. Epilepsy | .35 |
| 14. Activities of daily living in the home | .78 |
| 15. Activities of daily living outside the home | .83 |
| 16. Self-care | .78 |
| 17. Relationship problems | .57 |
| 18. Profession and activities | .67 |
The factor weights above .30 appear in bold.
The omega coefficient was .87, indicating good internal consistency.36 The ICC among the scores obtained by the 2 examiners was .95 (95% confidence interval .89–.97). The ICC between the scores obtained in the test and the retest was .98 (95% confidence interval .96–.99). These values indicate excellent interexaminer and test–retest reliability.
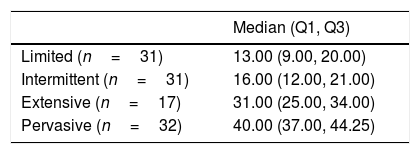
Validity of the relationship with other external variablesFig. 1 shows that the scores of the HoNOS-LD sections correlated in the expected direction with the scores of the other instruments that measure related constructs. Table 3 shows the quartiles of the HoNOS-LD score according to the level of support needed by the participants. Given that a higher score implies poorer functioning, it would be expected that the score would increase with the level of support. The Kruskal–Wallis test – H (3)=76.23, p<001 – and comparisons between pairs of groups using the Mann–Whitney U test confirmed the hypothesis: Us<57.00, ps<001, rs<−.56. The only comparison of means that was not significant was the one that involved the participants with limited levels of support and with intermittent levels of support: U=371.00, p=.12, r=−.20 (Table 3).

The aim of this paper was to find evidence of the validity of the scores obtained with the HoNOS-LD scale translated into Spanish, using a sample of people with IDD and mental health problems and/or behavioural disorders. The median HoNOS-LD score of this study's sample (24.00) is higher than the mean scores obtained by Roy et al.11 (18.26 and 18.55 for each of the 2 examiners) and Tenneij et al.18 (12.27 and 13.19 for nursing and psychology/psychiatry professionals, respectively). We should bear in mind that the sample in this research study comprised more people with extensive and pervasive support needs compared to the study by Roy et al. (44.2% vs 26.5%, respectively). With respect to the paper by Tenneij et al., the authors excluded the group with the most support needs and only considered a sample with a limited-intermittent support level. If only the median scores of the participants of this sample with limited and intermittent support levels are considered (13.00 and 16.00 respectively), the medians/means of the studies are similar.
With regard to the internal structure analysis, we must bear in mind that the HoNOS-LD was conceived as a scale to assess functioning in people with IDD and mental health problems/behavioural disorders, and this is determined by variables of various types that attempt to measure with each of the items. Therefore, conceptually, each item would be a partial but “necessary” measure of the general functioning construct. In this sense, various issues need to be highlighted. Firstly, we chose to undertake a factor analysis because, unlike a principal component analysis, it distinguishes between common variance between the items (which is explained by the factors) and error variance. This type of analysis is considered more appropriate in the area of psychometry, where the variables analysed often have a degree of measure error. In addition, despite being based on a clear hypothesis about the number of factors underlying the scores of the scale (in this case one), we took into account that each of the items did not constitute a factorially pure measure. Therefore we chose an exploratory factor analysis rather than a confirmatory analysis.41 Secondly, in light of the importance of evaluating the internal structure of the scores of a psychometric instrument in the process evidencing its validity, it is important to highlight that in the study to create the original HoNOS-LD scale no analysis was undertaken to determine the factor validity, since selection of the items was based on clinical criteria alone.11 In this sense, despite the fact that the model fit was not satisfactory according to the residual root mean square and the GFI index, we considered that it was important to take into account the same aspects of the functioning of people with IDD that were covered in the original version. For this reason, we chose to keep certain items that showed low factor weights, but that are relevant from a clinical perspective. Furthermore, it is noteworthy that the semiotics of the items with lower factor weights related to clinical problems. This might be associated with the fact that all the participants in this study received care in a specialist mental health centre for people with IDD and that, therefore, it was presupposed that the clinical symptoms of these people were well controlled. The importance of these aspects would be reflected in people with IDD not receiving appropriate care for their mental health problems/behavioural disorders.
The internal consistency of the scale was good, with an omega coefficient of .87. This value is comparable with the Cronbach's alphas indicated by Tenneij et al.,18 at .89 and .74, depending on whether the examiners were nursing or psychology/psychiatry professionals, respectively. The interexaminer reliability was excellent with an ICC of .95. This value is higher than those of Roy et al.11 (Pearson correlations of .93 and .76 for evaluation times 1 and 2, respectively) and of Tenneij et al. (ICC of .72). These differences might be due to the fact that in this research study only 2 psychologists (both trained in the area of IDD) took part in the interexaminer reliability study, whereas the other investigators were higher in number and had varied training. This study is the first to provide data on the test–retest reliability of the HoNOS-LD scale which, with an ICC of .98, was excellent.
Each of the sections of HoNOS-LD scale correlated in the expected direction and in a highly significant way (p<.001) with the other instruments. This indicates that, despite its brevity, the HoNOS-LD scale is an appropriate measure of different aspects of the functioning of people with IDD and mental health problems/behavioural disorders. These aspects include challenging behaviours, cognition, clinical problems, adaptive skills and social relationships.42 The results show a correlation of .55 between the scores of section A to I of the HoNOS-LD scale (items 1.3) and the ABC scale. Roy et al.11 also used the ABC, but in this case its score correlated with the total score of the HoNOS-LD scale, obtaining correlations between .66 and .76 (depending on the examiners and the time of the assessment). Moreover, it can be observed how the HoNOS-LD score increases with the level of support required by the participants. This provides additional information about the validity of the relationship of the HoNOS-LD score with other variables, given that the higher the severity of the IDD, the poorer the functioning. Along the same lines, Tenneij et al.18 showed that individuals with IDD institutionalised in large closed residential complexes (those with a higher number of behavioural disorders) had poorer functioning that those living in open residential units, or those living in standard environments.
The brevity of the HoNOS-LD scale enables it to be applied routinely and for a longitudinal register to be created. Moreover, the scale evaluates separately the aspects that combine to define the general functioning of an individual, so that it indicates the specific areas where impairment appears and can provide an indication of the aetiology of the mental health problems. This is an advantage compared to other scales used for the same purpose, such as the Global Assessment of Functioning Scale,43 which does not make this distinction. If a psychiatric disorder is suspected, it will be necessary to complement the information obtained using the HoNOS-LD with that provided by other instruments adapted for the IDD population, such as the complete interview of the Psychiatric Assessment Schedule for Adults with Developmental Disabilities, based on ICD-1014 criteria. In addition, it is important to take into account previous levels of cognitive functioning using different neuropsychological evaluation scales (Barcelona Test for people with Intellectual Disabilities44 or CAMDEX-DS45), as well as adaptive skills, with scales such as the Adaptive Behaviour Scale-Residential and Community, second edition33 or the System for the Evaluation of Adaptive Behaviour.46
The HoNOS-LD scale enables the benefits of an intervention to be evaluated beyond its effect on the specific symptoms of a disorder. This is important in assessing whether there has also been improvement in the different areas of the individual's functioning. In this regard, the English version of the scale has already been used in various studies that evaluated the efficacy of an intervention, including positive behavioural support,20 behavioural activation for depressive symptoms21 and bereavement support.19 Obviously, instruments should be used together with the HoNOS-LD scale that specifically assess changes in symptoms, such as the ABC for behavioural problems.16 In addition, the HoNOS-LD scale has been used to evaluate the quality of IDD specialist services in a considerable number of research studies.22–24
This study has some limitations that should be taken into account. Firstly, a larger sample size would have been advisable for the internal structure analysis of the scores.4 Moreover, the participation of native translators who were specialists in IDD psychopathology would have made the translation more sensitive. Nevertheless, the translators of the scale had suitably competent levels in the original language to ensure the translation and back-translation. Finally a social desirablity scale could have been included, such as the Marlowe–Crowne Social Desirability Scale adapted to Spanish by Ferrando et al.,47 because it provides some advantages when assessing certain personality items. Nevertheless, it is worth mentioning that these types of scales (with questions such as “before I vote I get detailed information on the ability of the candidates” or “sometimes I look for revenge rather than forgiving or forgetting something that someone has done to me”) are not manageable with the IDD population, not only because of the complexity of their semantic structures, but because of the cognitive deployment required for the responses. Equally, self-report scales could have been included; however, for the abovementioned reasons, their use in patients with IDD is advised against.
In sum, the results obtained indicate that the Spanish version of the HoNOS-LD scale is a brief, valid and reliable instrument to evaluate changes in general functioning in people with IDD and mental health problems. Its routine use could improve the quality of care for this group, helping to identify mental health problems and their causes, as well as the consequences of these problems, and contribute to the assessment of the efficacy of interventions.
Ethical responsibilitiesProtection of human and animal subjectsThe authors declare that the procedures followed comply with the ethical guidelines of the committee responsible for human experimentation, and with the World Medical Association's Helsinki Declaration.
Confidentiality of dataThe authors declare that they have followed the protocols of their centre of work with regard to the publication of patient data.
Right to privacy and informed consentThe authors obtained the informed consent of the patients and/or subjects referred to in the article. This document is held by the corresponding author.
FinancingThis paper was financed through the project “Estudi de les necessitats de tractament psiquiàtric i psicològic en usuaris que resideixen als dispositius de l’ICASS (2007–2009)” of the Departament d’Acció Social i Ciutadania (Department of Social Action and Citizenship) (Government of Catalonia).
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Esteba-Castillo S, Torrents-Rodas D, García-Alba J, Ribas-Vidal N, Novell-Alsina R. Traducción y validación de la versión española de la escala Health of the Nation Outcome Scales for People with Learning Disabilities (HoNOS-LD). Rev Psiquiatr Salud Ment (Barc). 2018;11:141–150.