







The aim of this study is to investigate the nature of the link associating the risk propensity of smoking and overweight. For example, a person who is a smoker and obese does not have to be more prone to risk than another person who is obese and a non-smoker.
Material and methodsThe data were taken from the German Questionnaire on Personality and Daily (Cross section for the period 2005). This questionnaire was selected because it collects individual data on the sociodemographic characteristic, behaviours, risk attitudes, lottery games, and health status. Our main contribution is to analyze the role of risk propensity taking into account smoking and overweight.
ResultsRisk propensity encourages smoking, and smoking and overweight are positively associated. The greater the role of the unobserved characteristics, the lower the correlation between smoking and overweight is. Although the risk propensity is an important determining factor of individual behaviour (smoking and overweight), its inclusion does not decrease the influence of personal circumstances and conditions. The need to define other measurements to be able to analyze the risk propensity of risk specific to risk behaviour is also highlighted.
DiscussionTo reduce the number of smokers it would require interventions in life styles. Given that overweight is an important determining factor in the decision to smoke, encouraging healthy behaviours, such as physical exercise or balanced diets, could improve the health status of the population in reducing obesity rates, and consequently the number of smokers.
El objetivo de este trabajo es estudiar la naturaleza del nexo de unión entre la propensión al riesgo, fumar y el sobrepeso. Por ejemplo, una persona que sea fumadora y obesa no tiene porque ser más propensa al riesgo que otra persona que sea obesa pero no fumadora.
Material y métodosLos datos proceden de la Encuesta Alemana sobre Personalidad y Vida Cotidiana (corte transversal para el periodo 2005). Hemos seleccionado esta encuesta porque recoge datos individuales sobre características socio-demográficas, comportamientos, actitudes de riesgo, juegos de loterías y estados de salud. Nuestra principal contribución es analizar el rol de la propensión al riesgo considerando el consumo de tabaco y sobrepeso.
ResultadosLa propensión al riesgo fomenta fumar, y fumar y el sobrepeso están correlacionados positivamente. Cuanto mayor es el papel de las características inobservadas, menor es la correlación entre fumar y el sobrepeso. Aunque la propensión al riesgo es un determinante relevante del comportamiento individual (fumar y sobrepeso), su inclusión no menoscaba la influencia de las circunstancias y condiciones personales. También destacamos la necesidad de definir medidas de propensión al riesgo específicas al comportamiento de riesgo a analizar.
DiscusiónPara reducir los ratios de fumadores sería necesario actuaciones sobre los estilos de vida. Dado que el sobrepeso es un determinante importante de la decisión de fumar, promover comportamientos saludables (ejercicio físico o dietas equilibradas, entre otras) podría mejorar el estado de salud de los ciudadanos al reducir los ratios de obesidad, y consecuentemente los ratios de fumadores.
Preventive campaigns remind recurrently citizens about the dangers of smoking and being overweight. Their messages usually make reference to scientific research that quantifies the effects of life styles on health. For example, an anti-tobacco campaign of the World Health Organization1 states that smokers have a 12-times higher probability of suffering from laryngeal cancer than non-smokers. Although the message of tobacco campaigns is simple (“smoking kills”), many smokers are reticent to quit the habit. The reasons for not quitting smoking are wide ranging such as tobacco addiction (past consumption reinforces their current demand)2,3 or the generalized belief that people who quit smoking put on weight.4–6
The reasons for not quitting smoking and/or not controlling the body weight depend on individual priorities. There might be people who smoke, eat in a compulsive way or not practice any physical sport because their future discount rate is high, so they enjoy the present moment without worrying about the potential negative consequences of present behaviours.7–9 However the relationship among risk seeking, risky behaviours and health outcomes is more complex. For example, there might be also people who smoke because they assign a higher value to their social and body images than to their state of health. In this last case, smokers are not only behaving rationally, but also as risk averse.
This argumentation line has important implications for the theory and practice of welfare. The consumers’ freedom to choose is the key concept to make people responsible for their own actions. The transfer of responsibility to the individual exonerates the policy makers from implementing any kind of public action. For example, if smokers have health problems derived from consuming tobacco products, they should cover the expenses of their medical treatments and not the state.
Accepting that people smoke on the basis of biased subjective probabilities implies reconsidering the doctrine of consumer sovereignty. In practice, many public policies are aimed at protecting citizens. Special indirect taxes, regulation of cigarette ingredients, restrictions on selling conditions or anti-tobacco informative campaigns are some examples of public interventions.7,10–12
Although there is no doubt that people are subject to manipulation by television commercials that play with the craving of perfect body images and social awkwardness, conventional economic theory has not considered these ideas in the economic principles.10,13–15 In this paper, we address the issue of tobacco consumption and overweight under the paradigm of risk uncertainty. To that end, we have drawn a sample of 1012 observations from the German Personality and Daily Life Survey (Pre-test, 2005). Although most national health surveys, such as the Spanish National Survey on Health (1987–2006), include standardised questions about risky behaviours and health outcomes (ever smoked; daily smokers; number of daily cigarettes; height; weight…), this German survey has the particularity of including a rich set of variables related to risk seeking (lottery games, risk perceptions and risk attitudes). All these variables allow us to control individual heterogeneity to a greater extent than data sets with only basic questions about socio-demographic characteristics, lifestyles and health outcomes.16
Although the expected utility framework has been implemented to analyze risk attitudes and behaviours with data drawn from lottery experiments,17–20 the contribution of this paper to the economic empirical literature is two-fold. First, we estimate simultaneously two kinds of independent but correlated risky behaviours (tobacco consumption and overweight) under the paradigm of risk uncertainty. Both risks are very common in modern societies, and many people are concerned about their weight when they think about quitting smoking and vice versa. The results of this research have important policy implications because if, for instance, overweight reinforces tobacco consumption, then health campaigns aimed at promoting physical exercise or the consumption of fresh fruits and vegetables might be also useful to control tobacco demand.21 Second, this paper highlights the importance of defining neutral measures of risk seeking. Risk seeking indexes based on lottery games might generate biased estimated parameters when analyzing the influence of risk seeking over a risky behaviour. For example, according to the literature review, income and smoking are negatively correlated, therefore smokers might be more likely to choose a fixed amount of money rather than a lottery ticket, because they might have low budgets and they might require money to buy tobacco products.22–24
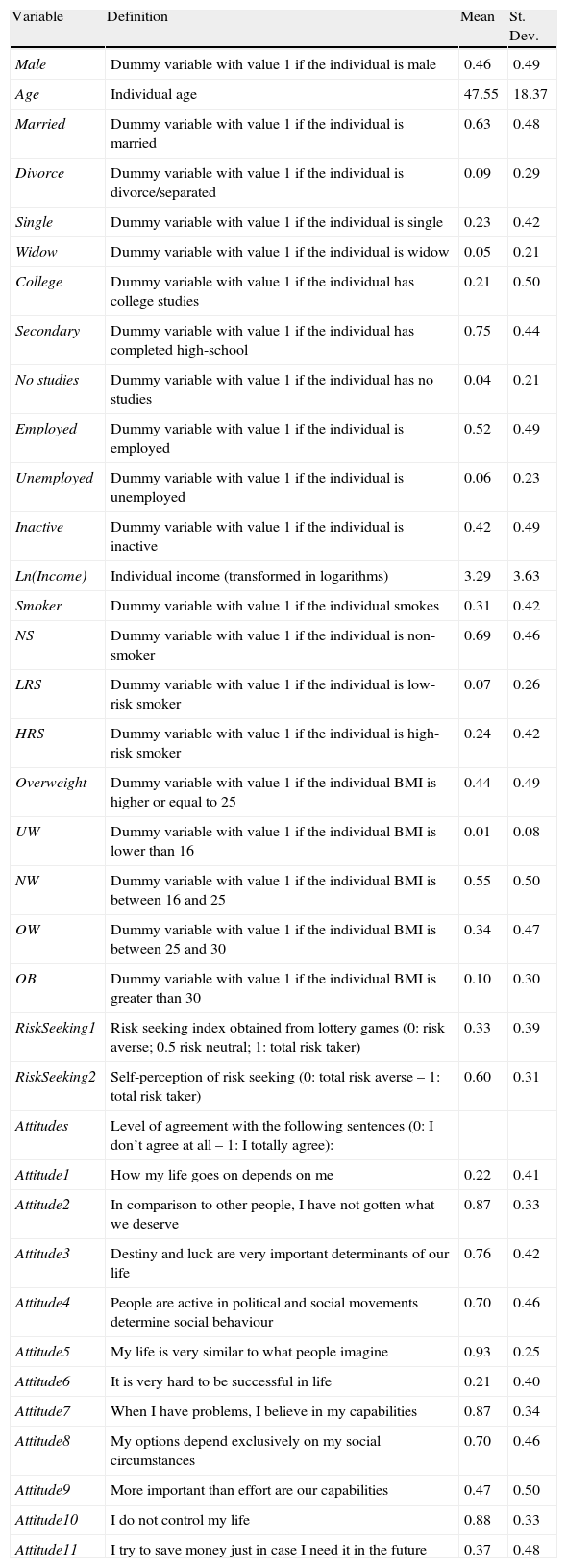
Data and methodologyThe German Personality and Daily Life Survey (Persönlichkeit und Alltag) provides us with exceptional variables to carry out this research. The structure of the survey is cross-sectional. The sample considers individuals all around Germany and it fulfils representative criteria: 1012 individuals from 14 to 90years old (543 females and 469 males) all over Germany. The main reason why we have selected this survey is because it compels standard socio-demographic variables with records of risky and healthy behaviours, risk attitudes, lottery questions and health outcomes. Given the reduced number of observations, we consider it necessary to check the representativeness of the data with other national surveys. In particular, we compare national rates of smokers and obese people over 50years old with data drawn from The Survey of Health, Aging and Retirement in Europe (SHARE) (see Table 1).
Variables.
| Variable | Definition | Mean | St. Dev. |
| Male | Dummy variable with value 1 if the individual is male | 0.46 | 0.49 |
| Age | Individual age | 47.55 | 18.37 |
| Married | Dummy variable with value 1 if the individual is married | 0.63 | 0.48 |
| Divorce | Dummy variable with value 1 if the individual is divorce/separated | 0.09 | 0.29 |
| Single | Dummy variable with value 1 if the individual is single | 0.23 | 0.42 |
| Widow | Dummy variable with value 1 if the individual is widow | 0.05 | 0.21 |
| College | Dummy variable with value 1 if the individual has college studies | 0.21 | 0.50 |
| Secondary | Dummy variable with value 1 if the individual has completed high-school | 0.75 | 0.44 |
| No studies | Dummy variable with value 1 if the individual has no studies | 0.04 | 0.21 |
| Employed | Dummy variable with value 1 if the individual is employed | 0.52 | 0.49 |
| Unemployed | Dummy variable with value 1 if the individual is unemployed | 0.06 | 0.23 |
| Inactive | Dummy variable with value 1 if the individual is inactive | 0.42 | 0.49 |
| Ln(Income) | Individual income (transformed in logarithms) | 3.29 | 3.63 |
| Smoker | Dummy variable with value 1 if the individual smokes | 0.31 | 0.42 |
| NS | Dummy variable with value 1 if the individual is non-smoker | 0.69 | 0.46 |
| LRS | Dummy variable with value 1 if the individual is low-risk smoker | 0.07 | 0.26 |
| HRS | Dummy variable with value 1 if the individual is high-risk smoker | 0.24 | 0.42 |
| Overweight | Dummy variable with value 1 if the individual BMI is higher or equal to 25 | 0.44 | 0.49 |
| UW | Dummy variable with value 1 if the individual BMI is lower than 16 | 0.01 | 0.08 |
| NW | Dummy variable with value 1 if the individual BMI is between 16 and 25 | 0.55 | 0.50 |
| OW | Dummy variable with value 1 if the individual BMI is between 25 and 30 | 0.34 | 0.47 |
| OB | Dummy variable with value 1 if the individual BMI is greater than 30 | 0.10 | 0.30 |
| RiskSeeking1 | Risk seeking index obtained from lottery games (0: risk averse; 0.5 risk neutral; 1: total risk taker) | 0.33 | 0.39 |
| RiskSeeking2 | Self-perception of risk seeking (0: total risk averse – 1: total risk taker) | 0.60 | 0.31 |
| Attitudes | Level of agreement with the following sentences (0: I don’t agree at all – 1: I totally agree): | ||
| Attitude1 | How my life goes on depends on me | 0.22 | 0.41 |
| Attitude2 | In comparison to other people, I have not gotten what we deserve | 0.87 | 0.33 |
| Attitude3 | Destiny and luck are very important determinants of our life | 0.76 | 0.42 |
| Attitude4 | People are active in political and social movements determine social behaviour | 0.70 | 0.46 |
| Attitude5 | My life is very similar to what people imagine | 0.93 | 0.25 |
| Attitude6 | It is very hard to be successful in life | 0.21 | 0.40 |
| Attitude7 | When I have problems, I believe in my capabilities | 0.87 | 0.34 |
| Attitude8 | My options depend exclusively on my social circumstances | 0.70 | 0.46 |
| Attitude9 | More important than effort are our capabilities | 0.47 | 0.50 |
| Attitude10 | I do not control my life | 0.88 | 0.33 |
| Attitude11 | I try to save money just in case I need it in the future | 0.37 | 0.48 |
The patterns of tobacco consumption are characterized by two important dimensions: frequency and quantity. Although the only way to prevent 100% the negative externalities of cigarettes is not smoking at all, smoking one pack of cigarettes per day does not have the same consequences than smoking a cigarette once in while. In fact, people who smoke more than 10 cigarettes per day are under risk of becoming nicotine addicts.25 Under this background, we discriminate high-risk smokers from low-risk smokers, being high-risk smokers those individuals who smoke more than 10 cigarettes per day. Means reveal that 31% of the interviewed smoke and 24% smoke daily more than 10 cigarettes, that is, 75% of the smokers are under risk of becoming nicotine addicts.
Regarding the body weight, we consider the Body Mass Index (BMI) because the survey includes self-reported questions about weight and height.26 According to the sample population, 1% of the interviewed are underweight, 55% keep a healthy weight, 34% are overweight and 10% are obese.
Given that most smokers are high-risk smokers and only a minority of them suffer from underweight (BMI<16) or chronic obesity (BMI≥40), we consider two categories for both risks (Smokers&NoSmokers and Overweight&NoOverweight) in the regression analysis in order to simplify results. Combining both risky dimensions in one variable (Smoker&Overweight, NoSmoker&Overweight, Smoker&NoOverweight and NoSmoker&NoOverweight) shows important gender and age differences. The Chi2 test of independence provides us with expected frequencies of how often persons with a common characteristic are smokers and/or overweight (we repeat the Chi2 test twice: by sex and by age among men and women). The Chi2 analyses are large, which means that variables sex and age are related to the before-mentioned dimensions of smoking and overweight (see Figs. 1 and 2).

.")
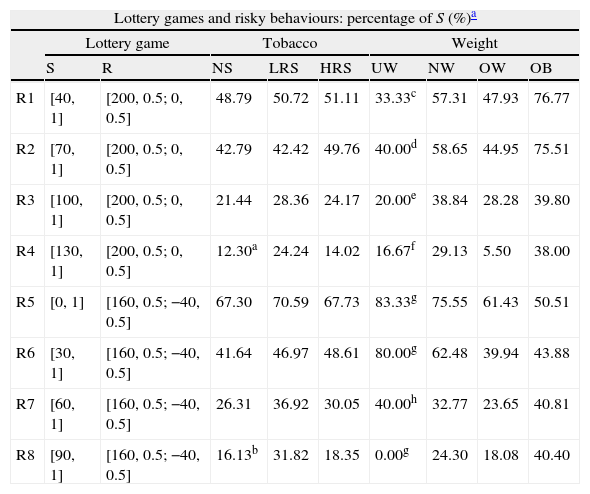
To determine individual levels of risk seeking, we focus on two kinds of indexes based on different information. First, we look at lottery games and then, at self-reported levels of risk seeking. Lottery questions inform us about the kind of prizes people prefer: a fixed amount of money or a lottery ticket with assigned winning probabilities. To understand the correlation between risky attitudes and risky behaviours, we define different kinds of risk seeking indexes.17,20 In the German Personality and Daily Life Survey, there are 8 game lotteries (R1–R8) in which the interviewed person has to choose among a lottery ticket or a fixed amount of money (see Table 2).
Risk seeking and risky behaviours.
| Lottery games and risky behaviours: percentage of S (%)a | |||||||||
| Lottery game | Tobacco | Weight | |||||||
| S | R | NS | LRS | HRS | UW | NW | OW | OB | |
| R1 | [40, 1] | [200, 0.5; 0, 0.5] | 48.79 | 50.72 | 51.11 | 33.33c | 57.31 | 47.93 | 76.77 |
| R2 | [70, 1] | [200, 0.5; 0, 0.5] | 42.79 | 42.42 | 49.76 | 40.00d | 58.65 | 44.95 | 75.51 |
| R3 | [100, 1] | [200, 0.5; 0, 0.5] | 21.44 | 28.36 | 24.17 | 20.00e | 38.84 | 28.28 | 39.80 |
| R4 | [130, 1] | [200, 0.5; 0, 0.5] | 12.30a | 24.24 | 14.02 | 16.67f | 29.13 | 5.50 | 38.00 |
| R5 | [0, 1] | [160, 0.5; −40, 0.5] | 67.30 | 70.59 | 67.73 | 83.33g | 75.55 | 61.43 | 50.51 |
| R6 | [30, 1] | [160, 0.5; −40, 0.5] | 41.64 | 46.97 | 48.61 | 80.00g | 62.48 | 39.94 | 43.88 |
| R7 | [60, 1] | [160, 0.5; −40, 0.5] | 26.31 | 36.92 | 30.05 | 40.00h | 32.77 | 23.65 | 40.81 |
| R8 | [90, 1] | [160, 0.5; −40, 0.5] | 16.13b | 31.82 | 18.35 | 0.00g | 24.30 | 18.08 | 40.40 |
| Self-perception of risk seeking and risky behaviours | |||||||
| NS | LRS | HRS | UW | NW | OW | OB | |
| Self perception of risk seeking(Scale from 0 to 1 increasing in risk seeking) | 0.52 | 0.53 | 0.51 | 0.5g | 0.47 | 0.55 | 0.64 |
[yH, pH; yL, pL] represents a probability of pH of obtaining yH Euros and a probability of pL of obtaining yL Euros.
ANOVA: Bonferroni pairwise comparison: a denotes that Mean(NS)<Mean(LRS) with a significance level of 5%; b denotes that Mean(NS)<Mean(LRS) with a significance level of 1% and Mean(LRS)>Mean(HRS) with a significance level of 5%; c denotes that Mean(NW)>Mean(OW) with a significance level of 5% and that Mean(OB)>Mean(OW) and Mean(OB)>Mean(NW) with a significance level of 1%; d denotes that Mean(NW)>Mean(OW) and Mean(OB)>Mean(NW) with a significance level of 1% and that Mean(NW)<Mean(OB) with a significance level of 5%; e denotes that Mean(OB)>Mean(NW) with a significance level of 1%; f denotes that denotes that Mean(NW)>Mean(OW) and Mean(OB)>Mean(OW) with a significance level of 1%; g denotes that Mean(NW)>Mean(OW) and Mean(NW)>Mean(OB) with a significance level of 1%; h denotes that Mean(NW)>Mean(OW) with a significance level of 5% and that Mean(OB)>Mean(OW) with a significance level of 1%.
Games in which the expected value of safe and risky options are the same offer an unbiased environment to observe who is risk averse or risk taker. If for example, the expected value of the risky option was higher, then there would be an additional incentive to choose the lottery ticket versus the fixed amount of money. There are two games (R3 and R7) in which the expected value of the lottery game is equal to the fixed amount of money, so our first index of risk seeking is the number of times the individual chose the lottery ticket divided by two. We will refer to this risk seeking measure as RiskSeeking1.
On an average people behave as risk averse or risk neutral when facing lottery games, but they consider themselves as risk neutral or slightly risk taker when they are questioned about their self-perceived level of risk seeking. Risk seeking and risk affinity vary substantially by individual heritage, and are only partially explained by socio-economic positions.27 According to this argumentation line, definitions of risk aversion indexes based on monetary decisions might be strongly correlated to the socio-economic status. We also build up a risk seeking index based on the individual self-perception, thus we will refer to this risk seeking measure as RiskSeeking2.
RiskSeeking1 and RiskSeeking2 are positively correlated in a 23% (correlation coefficient statistically significant at 5%), which implies that the more conservative the people behave in lottery games, the more likely they are to perceive themselves as risk averse. However the magnitude of the correlation leaves enough space for different scenarios: there are individuals who consider themselves as risk seeking but they might prefer a fixed amount of money rather than a lottery ticket because they might just need the money. In fact, the differences between both indexes are palpable when analyzing risky behaviours. According to RiskSeeking1, people who are overweight are the most risk averse. However, according to RiskSeeking2, obese people are the most risk seeking followed by overweight and people with healthy BMI.
Lastly, risk attitudes provide us with an important outlook of the individual personality. For example, 22% of the interviewed think that their lives just depend on them; 76% believe that destiny and luck are important determinants of what happens to them; 87% think they have not gotten in life what they deserve in comparison to people who surround them; 87% rely on their capabilities to overcome problems.
Any person who faces decisions related to tobacco consumption or weight control in a framework of uncertainty will consider the consequences of every choice with the corresponding probabilities of occurrence. The selection criteria imply to choose that option that is associated with a higher expected utility. One important problem of traditional literature on freedom is not taking into account social interactions.28 Indeed, the usual framework assumes that individuals face opportunity sets from which they can choose any option without interactive constraints, but this is not necessarily true. For example, there might be people who smoke even accepting that smoking is bad for their health, because people who belong to their social environment smoke.
In addition there is a strong correlation among behaviours. Regarding smoking and body weight, it is generally accepted that people who stop smoking put on weight. The scientific literature review offers two main points of view. For some authors, smoking helps to control weight,4,29 for others there is no empirical evidence about this causality after controlling for endogenity between smoking and BMI.5,6
Experiments offer a new field for health researchers to identify the causation of different behaviours on health. If tobacco consumption is negatively correlated with the body weight, and at the same time, risk seeking promotes smoking, then it might be also extrapolated that risk seeking is correlated with the individual's body weight. Under this argumentation line, Dave and Saffer30 introduce in the alcohol demand function a proxy of risk seeking. The authors conclude that risk seeking has a significant negative effect on alcohol consumption. Following this argumentation line, we consider that the tobacco demand function is characterized by:
where the tobacco consumption for the individual ith (Ti) depends on socio-economic factors (Xi), the individual body weight (Wi), the individual risk seeking (Ri) and a set of unobserved variables summarized in a zero-mean error term (εi). The parameters to estimate are β0, β1, β2 and β3. The intercept (β0) is the value of Ti when all explanatory variables are equal zero, which is rather unlikely. It actually explains nothing about the relationship between the explanatory variables and the dependent variable, but we need to introduce it in the model to obtain good estimations of β1, β2 and β3. In fact, the key parameter for our research is β3 because it informs us about the causal effect of risk seeking on smoking decisions, controlling for differences in the observed and unobserved determinants of risky behaviours. The fundamental challenge in using observational data to estimate β3 is the possibility that even after controlling for observed characteristics, the unobserved determinants may vary with the risky behaviour. For example, weight is an endogenous explanatory variable:Our first approach to this challenge is the simplest: we include a rich set of observed characteristics (Xi) to model the impact of socio-demographic characteristics on the probabilities of being NoSmoker&NoOverweight (TWi=1), NoSmoker&Overweight (TWi=2), Smoker&NoOverweight (TWi=3) and Smoker&Overweight (TWi=4). Given the categorical nature of dependent variable we use Multinomial Logit Regressions:The main advantage of Eq. (3) is that it offers a reliable picture about the influence of socio-economic variables (Xi) on risky behaviours. All explanatory variables are exogenous, so there is no doubt of bias derived from endogeneity. The main disadvantage is that the role of risk seeking is compelled under the unobserved term, so this equation does not help us to understand how risk seeking determines risky behaviours. To overcome this difficulty, we repeat the estimation introducing a measure of risk seeking (Ri):Eq. (4) is estimated twice for RiskSeeking1 and RiskSeeking2 independently. The exogeneity test of Schmith–Bundell confirms that both RiskSeeking1 and RiskSeeking2 are endogenous explanatory variables at the level 1% (the estimated parameters of the residual of RiskSeeking1 and RiskSeeking2 in the estimation of TWi are equal to 10.87 and 39.49 with a z-statistics of 6.02 and 4.54 respectively). To understand how endogeneity misleads empirical results, we repeat estimations once again introducing this time risky attitudes variables (Ai):In the conceptual framework of economics, individual attitudes or preferences are important determinants of both smoking decisions and weight control. For example, individuals who think that destiny or luck are important determinants of their lives might be more likely to engage in risky behaviours than those individuals who think that their lives just depend on them. Controlling for a range of attitudes reduces unobserved heterogeneity and improves our estimated results.




Lastly, the estimations of Eqs. (1) and (2) will complete the estimated results for TWi. We carry out the exogeneity test of Schmith–Bundell to check all explanatory variables are independent variables. If any explanatory variable is simultaneously explained by the model that defines the dependent variable, then we might have a problem of endogeneity which might generate biased results. Given that the structure of our data is cross-sectional, if there were problems of endogeneity, the estimated results might show correlation effects rather than causal effects. The tests confirms that overweight is an endogenous explanatory variable of tobacco consumption at the level 5% (the coefficient of the residual of being overweight in the estimation of being smoker is equal to −5.47 with a z-statistic of 2.82). However, there is no empirical evidence that tobacco consumption is an endogenous explanatory variable of body weight (the coefficient of the residual of being smoker in the estimation of being overweight is equal to −3.47 with a z-statistic of 2.73). To overcome this technical problem of endogeneity, we consider a system of simultaneous equations following the approach of Altonji, Taber and Alder.31 According to these authors, assume that the correlation between the unobserved determinants of the outcome and the endogenous variable is equal to the correlation between the observed determinants of the outcome and the endogenous variable (Equal Selection Rule). To complete the follow-on results, we also carry out constrained bivariate probits models in which we fix the values of rho from 0 to 0.3.
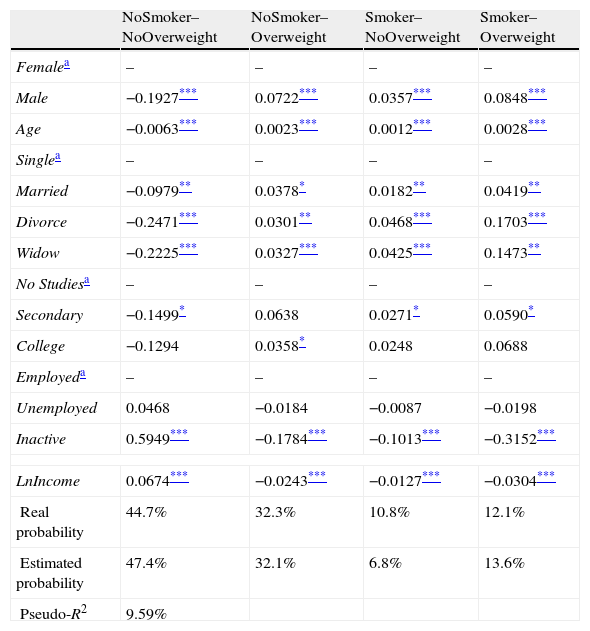
ResultsSocio-demographic characteristics are important determinants of smoking and overweight. Men are 19% less likely to be NoSmokers&NoOverweight than women, and the other way around are 8% more likely to be Smoker&Overweight, 7% to be NoSmoker&Overweight and 4% to be Smoker&NoOverweight. Taking into account the magnitude of the estimated parameters we conclude that men are worse at controlling their weight than their tobacco consumption. Similar results are obtained for the individual age; the older is the individual, the greater is the probability of being Smoker&Overweight, NoSmoker&Overweight and Smoker&NoOverweight. As a consequence, the older is the individual the worse he controls his body weight. Civil status also plays an important role on both risky behaviours. Single people are the most likely to be NoSmoker&NoOverweight. Married people are 4% more likely to be Smoker&Overweight than singles, resulting with the prevalence of overweight people being greater than the prevalence of smokers. Divorced and widows are around 15% more likely to be Smoker&Overweight than single, although for them the prevalence of smoking is slightly higher than the prevalence of overweight. Regarding differences on behaviours by educative levels, college studies are positively correlated with BMI, and secondary education with smoking decisions. Regarding working status, although there are no great differences among unemployed and employed, there are relevant differences comparing inactive and employed people. Inactive people are 60% more likely to be NoSmoker&NoOverweight. Lastly, income plays a relevant role, thus the greater is the income the lower is the probability of being Smoker&Overweight. The influence of income is greater on BMI than on smoking decisions. In both cases, the greater is the income the lower is the probability of smoking and being overweight, although the reduction of these probabilities is negatively correlated with the income. To analyze the explanatory power of the model, we focus on the Pseudo-R2 and the estimated probabilities. The explanatory variables only describe around 10% of the combined probabilities of smoking and overweight. The estimated values of these combined probabilities are acceptable compared to the real ones, especially in case of Overweight (see Table 3).
Socio-economic determinants of risky behaviours (Multinomial Probit Model: Marginal Effects).
| NoSmoker–NoOverweight | NoSmoker–Overweight | Smoker–NoOverweight | Smoker–Overweight | |
| Femalea | – | – | – | – |
| Male | −0.1927*** | 0.0722*** | 0.0357*** | 0.0848*** |
| Age | −0.0063*** | 0.0023*** | 0.0012*** | 0.0028*** |
| Singlea | – | – | – | – |
| Married | −0.0979** | 0.0378* | 0.0182** | 0.0419** |
| Divorce | −0.2471*** | 0.0301** | 0.0468*** | 0.1703*** |
| Widow | −0.2225*** | 0.0327*** | 0.0425*** | 0.1473** |
| No Studiesa | – | – | – | – |
| Secondary | −0.1499* | 0.0638 | 0.0271* | 0.0590* |
| College | −0.1294 | 0.0358* | 0.0248 | 0.0688 |
| Employeda | – | – | – | – |
| Unemployed | 0.0468 | −0.0184 | −0.0087 | −0.0198 |
| Inactive | 0.5949*** | −0.1784*** | −0.1013*** | −0.3152*** |
| LnIncome | 0.0674*** | −0.0243*** | −0.0127*** | −0.0304*** |
| Real probability | 44.7% | 32.3% | 10.8% | 12.1% |
| Estimated probability | 47.4% | 32.1% | 6.8% | 13.6% |
| Pseudo-R2 | 9.59% | |||
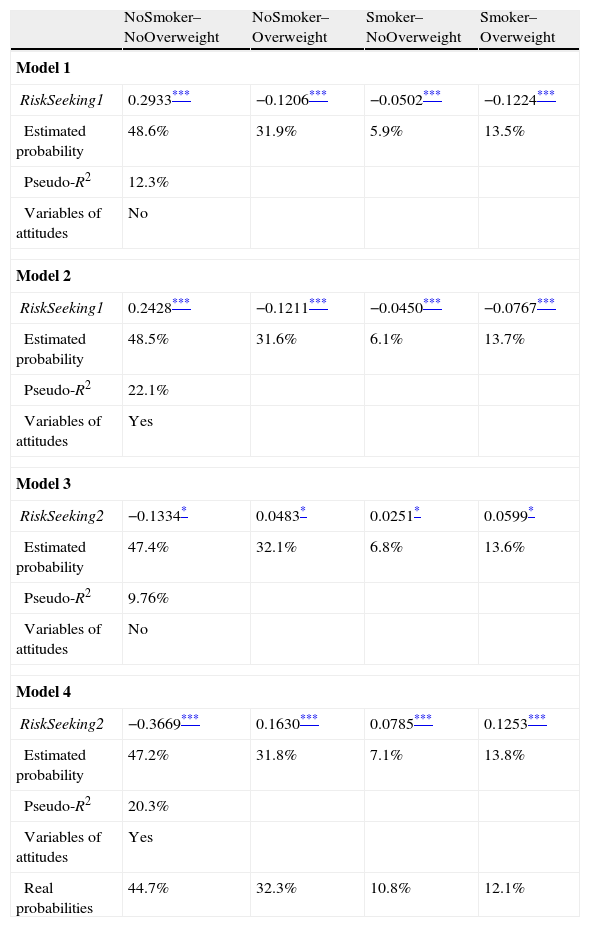
In Table 4, we complete estimations of Table 3 by introducing risk seeking measures and risk attitudes. As expected, the influences of RiskSeeking1 and RiskSeeking2 differ considerably. The more often the individual prefers the fixed amount of money versus the lottery ticket, the more likely he is to be Smoker&Overweight. However the higher is the self-perception of risk seeking, the more likely the individual is to be Smoker&Overweight. Changes in both risks affect more BMI than smoking decisions. Once we have introduced risk attitude variables, we can observe that RiskSeeking1 lose intensity which reinforces the idea that it behaves as an endogenous explanatory variable. Meanwhile RiskSeeking2 gains intensity and statistically significance. The measures of goodness of fit are contradictory. For one hand, according to the Pseudo-R2 the explanatory power of the models with attitude variables is better than for those models without them. In addition, the models with RiskSeeking1 adjust better than the models with RiskSeeking2. On the other hand, the model with RiskSeeking2 and without attitude variables seems to be the one that best predicts the dependent variable. Under this background, we continue working with RiskSeeking2 and without attitude variables because Model 3 provides good estimations of the dependent variable and the problem of endogeneity is less important than in the case of RiskSeeking1 (see Table 4).
Risk seeking as a determinant of risky behaviours (Multinomial Probit Model: Marginal Effects).
| NoSmoker–NoOverweight | NoSmoker–Overweight | Smoker–NoOverweight | Smoker–Overweight | |
| Model 1 | ||||
| RiskSeeking1 | 0.2933*** | −0.1206*** | −0.0502*** | −0.1224*** |
| Estimated probability | 48.6% | 31.9% | 5.9% | 13.5% |
| Pseudo-R2 | 12.3% | |||
| Variables of attitudes | No | |||
| Model 2 | ||||
| RiskSeeking1 | 0.2428*** | −0.1211*** | −0.0450*** | −0.0767*** |
| Estimated probability | 48.5% | 31.6% | 6.1% | 13.7% |
| Pseudo-R2 | 22.1% | |||
| Variables of attitudes | Yes | |||
| Model 3 | ||||
| RiskSeeking2 | −0.1334* | 0.0483* | 0.0251* | 0.0599* |
| Estimated probability | 47.4% | 32.1% | 6.8% | 13.6% |
| Pseudo-R2 | 9.76% | |||
| Variables of attitudes | No | |||
| Model 4 | ||||
| RiskSeeking2 | −0.3669*** | 0.1630*** | 0.0785*** | 0.1253*** |
| Estimated probability | 47.2% | 31.8% | 7.1% | 13.8% |
| Pseudo-R2 | 20.3% | |||
| Variables of attitudes | Yes | |||
| Real probabilities | 44.7% | 32.3% | 10.8% | 12.1% |
Lastly, we conclude with the estimations of Smoker and Overweight taking into account as determinants their reciprocal influence and a measure of risk seeking. To achieve identification, we impose different values of rho. According to the Equal Selection Rule that imposes the same distribution to unobserved characteristics, rho takes a value of 0.2. In addition, we consider other three values of rho: 0, 0.1 and 0.3. First, we would like to point out that smoking reinforces overweight and vice versa. Second, when we introduce a risky behaviour on the estimation of the other one, risk seeking index loses intensity and statistical significance. In fact, there is only evidence that risk seeking promotes smoking. And third, the greater is the imposed level of correlation between unobserved characteristics, the greater is the influence of risk seeking for smoking and the lower is the influence of Smoker on Overweight and vice versa. Comparing the model in which we impose the Equal Selection Rule with the ones of previous tables, the estimated probabilities of the four different combinations of smoking and overweight are the most precise (see Table 5).
Smoking and weight (Constrained Bivariate Probit Model: Marginal Effects).
| Model 1Rho=0.3 | Model 2Rho=0.1 | Model 3Rho=0 | Model 4Equal Selection Rule | |
| Smoker | ||||
| Overweight | 0.2594** | 0.6172*** | 0.7855*** | 0.4633*** |
| RiskSeeking2 | 0.4126* | 0.3931*** | 0.3812 | 0.4024* |
| Overweight | ||||
| Smoker | 0.2902** | 0.6625*** | 0.8374*** | 0.5024*** |
| RiskSeeking2 | 0.1717 | 0.1311 | 0.1125 | 0.1484 |
| Estimated rho | – | – | – | 0.19 |
| Prob(Smoker=1, Overweight=1) | ||||
| Mfx: RiskSeeking2 | 0.0706 | 0.0561 | 0.0493 | 0.0623 |
| Prob(Smoker=1, Overweight=0) | ||||
| Mfx: RiskSeeking2 | 0.0363 | 0.0437 | 0.0469 | 0.0406 |
| Prob(Smoker=0, Overweight=1) | ||||
| Mfx: RiskSeeking2 | −0.0030 | −0.0045 | −0.0050 | −0.0038 |
| Prob(Smoker=0, Overweight=0) | ||||
| Mfx: RiskSeeking2 | −0.1039 | −0.0954 | −0.0912 | −0.0991 |
| Estimated probability: | ||||
| Smoker | 20.3% | 20.5% | 20.9% | 20.4% |
| Overweight | 45.7% | 45.8% | 45.7% | 45.7% |
| Smoker–Overweight | 12.0% | 10.1% | 10.1% | 11.1% |
| Smoker–NoOverweight | 8.4% | 9.9% | 10.6% | 9.2% |
| NoSmoker–Overweight | 33.7% | 35.1% | 35.6% | 34.5% |
| NoSmoker–NoOverweight | 45.9% | 44.3% | 43.6% | 45.0% |
Mfx: Marginal effects are the estimated elasticities, that is, how much and in which sense the dependent variable varies when one independent variable changes 1%, considering the remaining independent variables constant.
In each model, we have also included the socio-demographic variables of Table 3. Complete table of results is available under request to the author.
This research paper brings to light that risk seeking characterizes risky behaviours such as smoking and overweight. However this paper also states the importance of defining risk seeking indexes including more than one dimension. Kahnemann and Tversky32 already argued that when analyzing choices under uncertainty it is not enough to carry out lottery games. Rather, we should know more about the situation at the time the individual makes his choice. For example students prefer a fixed amount of money rather than a lottery ticket. This choice does not necessary mean that students are more risk averse, but only they do not have much money, so they value small amounts of money like 50 Euros more than adults who work.22–24
Given the importance of lifestyles in the state of health, it is necessary to design strategies that go beyond fiscal policies (for example, tobacco taxation), and act over other fields such as physical exercise.10,12
The promotion of physical health care is important for all population groups (women and men, young people and elderly). Obese people who smoke are at risk of developing health and social problems. Addressing overweight prevents future health problems, but it has also important effects on ill-diagnosed people.33 For example, the excess cardiovascular mortality associated with mental problems is attributed to an increased risk of the modifiable coronary heart disease risk factors, obesity, smoking, diabetes, hypertension, and dyslipidaemia.34
In addition, health care providers should be aware of underlying other heath issues, particularly obesity, in patients seeking smoking cessation treatment. For example, smokers who seek treatment may have suffered other health problems such as obesity and hepatitis…, so their health profile may be different from those smokers who do not consider quitting.35 Causes and consequences of smoking and eating are studied from different perspectives (dieting, lifestyle, behavioural treatments, pharmacotherapy, surgery, and intensive in-patient treatment) to suggest policies aimed at improving citizen's health status. There is a generalized tendency of integrating all these strategies to benefit from positive synergies.
Given that there is a positive relation between smoking and overweight, especially among younger females,36 changing eating behaviours of overweight smokers may trigger positive change in smoking behaviours. Smokers interested in losing weight typically hold higher expectations for the benefits of weight loss than when they do for quitting smoking. As such, they are more likely to attempt weight loss than smoking cessation. Consequently, weight control programme is also an effective strategy to reduce smoking. Joint effort among food and nutrition professionals, physicians, and other health care professionals may be necessary to facilitate change in individuals.37,38
Both individual and environmental approaches should be considered.39 Integration of clinical and community resources for health prevention, such as school teachers and child health-carers, could serve as potential models for structuring future treatment approaches.40
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestThe authors have no conflict of interest to declare.
Please cite this article as: Gil-Lacruz AI, Gil-Lacruz M. El rol de la propensión al riesgo para fumadores y personas con sobrepeso. Rev Psiquiatr Salud Ment (Barc.). 2012;5:139–49.