









The purpose of this study was to identify homogenous subgroups of adolescents with emotional and behavioural difficulties using latent profile analysis. The relationship between the latent profile classes and socio-emotional and school adjustment was also analysed.
Materials and methodsA total of 1506 students, 667 men (44.3%) were selected by random cluster sampling. The mean age was 16.15 years (SD=1.36). The instruments used were the Strengths and Difficulties Questionnaire, the Personal Wellbeing Index-School Version, The 10-item Positive and Negative Affect Schedule for Children, the Prodromal Questionnaire-Brief, the Paykel Suicide Scale, the Cyberbullying-Brief Questionnaire, the Penn Matrix Reasoning Test, and the school performance assessment.
ResultsA total of 7.7% of adolescents obtained risk scores for mental health difficulties. We identified 3 mental health subgroups named: Low risk, Externalizing, and Internalizing. These 3 latent classes demonstrated a differential pattern in terms of socio-emotional adjustment and academic performance.
ConclusionsTo identify and validate risk groups of youths for emotional and behavioural problems allows implementing measures to promote emotional well-being and prevent mental health problems. Future studies should continue to analyse young people with emotional and behavioural problems longitudinally and to incorporate new forms of assessment and intervention.
El propósito de este estudio fue identificar subgrupos de adolescentes con dificultades emocionales y conductuales mediante análisis de perfiles latentes. También se analizó el patrón diferencial de ajuste personal, socioafectivo y escolar entre los perfiles latentes identificados.
Materiales y métodosMediante muestreo aleatorio estratificado por conglomerados se seleccionaron un total de 1.506 estudiantes, 667 varones (44,3%). La media de edad fue de 16,15 años (DT=1,36). Se utilizaron el Cuestionario de Capacidades y Dificultades, el Índice de Bienestar Personal-versión escolar, la Escala breve de Afecto Positivo y Negativo, el Cuestionario de Pródromos de Psicosis Breve, la Escala Paykel de Suicidio, la Test Matrices de Razonamiento, el Cuestionario de Ciberbullying Breve y un test ad hoc para la evaluación del rendimiento académico.
ResultadosEl 7,7% de los adolescentes obtuvo puntuaciones de riesgo en dificultades de salud mental. Se identificaron 3 conglomerados de participantes denominados: bajo riesgo, externalizante e internalizante. Estos 3 perfiles demostraron un patrón diferencial en cuanto a ajuste socioemocional y rendimiento académico.
ConclusionesIdentificar y validar grupos de jóvenes de riesgo para problemas emocionales y comportamentales permite poner en marcha medidas de promoción del bienestar emocional y la prevención de problemas mentales. Futuros estudios deberían seguir analizando longitudinalmente a los jóvenes identificados con problemas emocionales y conductuales e incorporar nuevas formas de evaluación e intervención.
Mental disorders are one of the major problems of worldwide-associated disability, morbimortality and financial burden.1–3 In fact, they are one of the first causes of associated disability and disease burden in the 10–24 year age group.4,5 It has been estimated that approximately one in every 5 children and teenagers have psychological problems,1 persisting into adulthood in some cases.6 At the same time, referring psychological problems in childhood and adolescence is a risk factor for the development of mental disorders in adulthood.7,8 The roots of the majority of mental health problems are to be found in these initial stages of development. Also, the presence of emotional and/or behavioural symptoms at subclinical level raise the risk of subsequent development of mental disorder.9–11
The impact of mental health problems on a personal, family, educational and social health level is clear. Early detection strategies therefore need to be implemented, within an emotional wellbeing promotion model and mental health disorder prevention model. An optimal strategy for prevention would be the reliable identification and detection of young people with psychological problem risks, prior to their transition to mental health disorder status.12 The purpose of all of this would be to establish empirically validated prophylactic treatments, when pertinent. The inclusion of detection and identification of risk subgroups may also help in the understanding of underlying causal mechanisms, to optimize treatments and establish psychotherapeutic targets.
Methodological advances and new psychometric models may enhance this aim. For example, the mixture models are a type of statistical method that try to identify homogeneous types of subgroups according to a certain set of variables (e.g. scores in a test). When the analysed variables are continuous they are known as latent profile models, whilst if they are dichotomic in nature they are known as latent class (LC) models.13 This methodology has been extensively used in mental health to empirically identify risk or protection groups in the general population or in clinical samples. Specifically, using the Strengths and Difficulties Questionnaire, SDQ14 (a tool used for the assessment of emotional and behavioural problems) and cluster analysis, 2 studies found differentiated patterns of emotional and behavioural problems in the child and youth population.15,16 However, to date, there are no known studies which have analysed the LC of emotional and behavioural difficulties and pro-social abilities, using the SDQ,14 in Spanish teenagers. At the same time, few studies at international level have analysed the latent profiles underlying socio-emotional adjustment during adolescence.17
Within this research context, the general aim of this study was two-fold. On the one hand, to empirically identify subgroups or profiles of emotional and behavioural problems and prosocial behaviour in a representative teenage sample using latent profile analysis and on the other, to validate the subgroups identified analysing the differential impact of personal, socio-emotional and academic adjustment with different psychometric indicators of emotional wellbeing, positive and negative affect, risk of psychosis, bullying and academic performance. In keeping with previous literature, it would be possible to determine different teenage subgroups according to the scores in the SDQ (emotional and behavioural problems and prosocial behaviour). Once the groups had been identified, we would expect to find teenagers who referred to a pattern of higher emotional and/or behavioural difficulties, who presented with poorer socio-emotional adjustment and with higher school violence and poorer academic performance, compared with the teenagers who had no emotional and behavioural problems.
Material and methodParticipantsIn order to guarantee the representativeness of the sample, stratified random sampling was made by conglomerates at the classroom level in a population of approximately 15,000 students belonging to the autonomous community of La Rioja. The strata were created according to school centre (state/private or grant-maintained) and the academic stage (statutory secondary, baccalaureate and vocational training), where the probability of extraction from the class in the school centred was determined by the number of students.
The initial sample comprised 1881 students, with elimination of those participants who presented with a high score on the scale of response infrequency (over 3 points) (n=104), and aged over 19 years (n=95) or questionnaire with lost values (n=176). Thus, a total of 1506 students, 667 male (44.3%) and 839 (55.7%) female, belonging to 34 school centres and 98 classes participated in the study. Mean age was 16.15 years (standard deviation=1.36), oscillating between ages ranging from 14 to 19 years. Due to the small number of participants in the 19 year old age group, it was decided to combine it with those aged 18, and the 18–19 year old group therefore was made up of a total of 247 participants (16.2%).
Distribution of participant nationality was as follows: 89.9% Spanish, 3.7% Latin American (Bolivia, Argentina, Colombia and Ecuador), .7% Portuguese, 2.4% Romanian, 1% Moroccan, .7% Pakistani and 2% other nationalities.
Tools of measurementStrengths and Difficulties Questionnaire in its self-completion format14The SDQ is a widely used tool of measurement for the assessment of behavioural and emotional difficulties, and for assessment of prosocial abilities. The SDQ comprises 25 items with a Likert response format of 3 options (0=no, never; 1=sometimes; 2=yes, always). The items are grouped into 5 subscales (with 5 items each): emotional problems, behavioural problems, hyperactivity, problems with classmates and prosocial behaviour. The first 4 subscales for a total score of difficulties, the higher the score, the higher the level of emotional and behavioural difficulties, except for the prosocial behaviour subscale were the lowest score corresponds to poorer adjustment in behaviour. The metric properties of the SDQ were analysed in Spanish teenagers.18
Personal Well-being Index-School Children19,20The Personal Well-being Index-School Children, PWI-SC was developed to assess subjective well-being in school age children and teenagers.19,20 The PWI-SC contains a total of 8 items where the response options range from se 0=highly discontent to 10=highly content. The PWI-SC items are assessed in a relatively generic and abstract manner, with subjective satisfaction with a specific area of life. The first item of the scale analyses “life as a whole”. The other 7 items include satisfaction with: health, standard of living, life achievement, personal safety, personal relationships, future security, community connectedness. The global scale is the result of adding up the 7 items (except item 1). The metric properties of the PWI-SC were analysed in previous studies.19–21
Brief Cyberbullying questionnaire22The Cyberbullying (CB) questionnaire is a tool which assess bullying and cyberbullying behaviours. The CB is structured around a series of dimensions which consider: (1) Traditional bullying; (2) ICT accessibility (to internet and mobile phone); (3) Cyberbullying through internet; and (4) Cyberbullying by mobile phone. They psychometric properties of this tool of measurement were analysed in previous studies. Eight questions were selected from the CB (items 1–6, 16 and 17) which drew information on behaviour of bullying and cyberbullying. The CB has been extensively used in previous studies with Spanish teenagers.23,24
Prodromal Questionnaire-Brief25The Prodromal Questionnaire-Brief (PQ-B) is a self-completion report comprising 21 items which assess prodromal symptoms of positive type psychosis. The items are formulated in dichotomous format of True/False. If the participant says yes to the item, they have to mark their degree of resulting concern or malaise on a Likert type scale with 5 options from 1=totally disagree to 5=totally agree). In the general population, this tool may also be used as a screening tool for risk of psychosis26 or as a measure of assessment of mitigated psychotic symptoms. The PQ-B has proven to be of use for the assessment of attenuated psychotic symptoms in young people.27 The PQ-B presents with appropriate psychometric properties in terms of score reliability (internal consistency a=.93), and essentially one-directional structure in samples of Spanish teenagers.28
Paykel Suicide Scale, PSS29The Paykel Suicide Scale, PSS is a tool designed for the assessment of different manifestations of suicidal behaviour (desire to die, ideation, planning, previous attempt). It consists of a total of 5 items with a dichotomous Yes/No response. Scores range between 0 and 5. The higher the scores, the greater the severity of suicidal ideation. The Paykel scale has been used previously on Spanish teenagers, showing evidence of appropriate psychometric quality.30–32
The 10-items Positive and Negative Affect Schedule for Children33The short 10-items Positive and Negative Affect Schedule for Children contains 10 items designed to measure positive and negative affect. The items have a Likert type format with answers ranging from 1=very little or nothing, to 5=extremely or a lot. Five items assess the positive affect using adjectives such as: cheerful, animated, happy, energetic, and proud; and another 5 negative affects; depressed, angry, fearful, scared and sad. The short PANAS for children is complemented by the teenage one, taking into account the way they have felt and/or behaved during the last few weeks. The short PANAS for children was used in previous studies with Spanish samples.34
Assessment of academic performanceTo measure the academic level of students they were asked the flowing question “what was your average mark in the previous year” which was to be answered in Likert form by one of 5 options: fail, pass, good, very good and excellent. The following question was added “did you fail any subjects in the previous year review? To which the response was Yes/No. If they did, they had to specify the number of failed subjects. Only the previous year's mark was used as an indirect marker of academic performance in this test.
Penn Matrix Reasoning Test35,36The Penn Matrix Reasoning Test, PMRT is a task within the Penn-Neurocognitive battery computerised child version. This task was developed to measure non-verbal reasoning (using problems of matrixial reasonings used in the Raven Progressive Matrix Test). PMRT comprises 20 elements and may be considered as a calculation of IQ. The PENN battery includes different neuro-behaviour indicator (e.g. memory, social cognition) with different tasks adapted to young people to ensure appropriate psychometric properties.
Family Affluence Scale-II37The Family Affluence Scale-II (FAS-II) rates the socioeconomic level using a measurement of family wealth of 4 items which are child appropriate. Scores range between 0 and 9, with higher score being indicative of a higher socioeconomic level. Previous studies have shown their appropriate psychometric properites.37
Oviedo response infrequency scale38The Oviedo response infrequency scale (INF-OV) was developed to detect those patients who had responded randomly, pseudo-randomly or dishonestly. The INF-OV is a self-completion type tool of measurement comprising 12 Likert type format items of 5 categories according to level of adherence (1=completely disagree; 5=completely agree). Once the items have been dichotomized, the student who gave an incorrect score to more than 2 items were eliminated from the study. This scale was used in previous studies and is valid for detecting participants who present with a random, pseudo-random or dishonest responses.39
ProcedureThe research was approved by the Directorate-general for education of the regional government of La Rioja and the Clinical Research Ethics Committee of La Rioja (CEICLAR for its initials in Spanish). Administration of the tools was collectively undertaken in groups of between 10 and 30 participants and in school centre classrooms. The whole procedure was done by computers, in school hours and for an approximate duration of 50min. To standardise the administration process, researchers who had been previously trained supervised the test administration. They were informed at all times of the confidentiality of the responses, and of the voluntary nature of participation, with no incentives being awarded for study participation. Informed consent was requested from fathers/mothers for participation of minors in the research. This study forms part of a study on emotional well-being during teenage years.
Data analysisFirstly, to examine the prevalence of emotional and behavioural difficulties, the descriptive statistics were analysed (mean, standard deviation, asymmetry, and kurtosis) of the SDQ scores in the total sample. The participant percentages were also calculated in each of the 3 score slots of the SDQ (No case, Limit and Possible risk) for the total sample and according to gender. In the self-completion version of the SDQ, a total score of difficulties between 0 and 15 was considered as “no case”; a score between 16 and 19 was considered the “limit”; and a score between 20 and 40 was considered as “probable case” or “possible risk of poor mental health”.
Secondly, to identify different subgroups of participants according to their scores on the SDQ latent profile analysis was performed. To examine and determine the number of possible subgroups the following indicator were considered. The Akaike Information Criterion (AIC),40 the Bayesian Information Criterion (BIC),41 and the sample-size adjusted BIC (ssaBIC).42 When values between models are compared, the lowest indicate better fit. Also, the different probability tests were taken into consideration where the K classes model was compared with the k-1 class model. This test tests out the nil hypothesis that there are no statistically significant differences. As such, a p<.05 value indicates that the k class model is better than the k-1 class model. Whilst a p>.05 value suggests that the k-1 class model is preferable in terms of data precision. The Lo-Mendell-Rubin's adjusted likelihood (LRT)43 test was also considered and its associated p value, as was the standardised entropy measurement (values close to 1 indicate better fit). This measurement assesses the relative precision when classifying participants in their respective groups; a high score indicates there is appropriate separation between the participants belonging to the different groups.44
Thirdly, once LC were identified, a MANCOVA was firstly performed to determine whether a differential pattern existed between the subgroups and the socioemotional fit, measured in scores through the SDQ, the PWI-SC, the brief PANAS for children, the PSS and the PQ-B. The total participant sample was used as a reference for calculating standard scores. Transforming test scores into Z scores enables comparison of scores to be made of all the instruments as the same scale of measurement is used. Gender, age, IQ and socioeconomic level effects were controlled. In the case of the MANCOVA, the Wilks Lamda value was used to confirm if any there were any statistically significant differences. Furthermore, for calculation of the effect size the partial η2 was used. Values of partial η2 of .01 indicate a small effect size, values of .06 a medium size and values above .14 a large effect size. However, to determine whether a differential pattern exist between the LC found and the academic performance and random behaviour, different contingency tables were performed, using the chi square test.
Data analysis was performed with the statistical programme SPSS v2245 and the Mplus 7.4.13
ResultsPrevalence of emotional and behavioural difficultiesResults showed that 7.3% of teenagers obtained scores relating to risk of emotional and behavioural problems (total score of difficulties of the SDQ). 13.7% was located in the limit score section and 79% of the sample was found to be in the no risk group. Considering the SDQ subscale scores, it was observed that 13.5% presented with high scores in the possible risk of emotional problems section, 8.5% in the behavioural problems section, 6.1% in problems with classmates, 16.5% in hyperactivity and 1.7% in prosocial behaviour.
With regard to gender, statistically significant differences were found in the emotional problems, behaviour problems subscales and in the total score of difficulties (p<.01) when the proportion of participants was compared in the different sections of the SDQ subscales. In emotional problems, there was a higher percentage of women than men, whilst the men reported higher behavioural problems compared with the women. Regarding total score of difficulties results showed that 9.4% of women were at a possible risk of poor mental health, whilst 5.8% of the men would be within this band, with the differences being statistically significant (χ2(2)=11.93; p<.01).
Identification and determination of latent profiles of emotional and behavioural difficultiesTo identify and determine participant subgroups according to their SDQ scores, different latent profile analyses were performed.
Table 1 contains the goodness of fit indices for the different models estimated. As may be observed, the model which best fit the data was that formed by 3 participant subgroups. Comparatively speaking, this model showed the highest entropy index, the p value of the LMR-A was statistically significant, and AIC and BIC values were lower.
Adjustment indices for latent class models of emotional and behavioural problems and prosocial behaviour.
| Models | Log-likelihood | AIC | BIC | ssaBIC | Entropy | LMR-A | LMR-A p |
|---|---|---|---|---|---|---|---|
| 1 class | −15199.62 | 30419.20 | 30472.42 | 30440.65 | – | – | – |
| 2 classes | −14876.51 | 29785.02 | 29870.19 | 29819.27 | .85 | 631.83 | .001 |
| 3 classes | −14725.83 | 29495.67 | 29612.65 | 29542.78 | .85 | 294.63 | .001 |
| 4 classes | −14649.18 | 29354.30 | 29503.24 | 29414.29 | .72 | 149.89 | .189 |
AIC: Akaike information criterion; BIC: Bayesian information criterion; LMR-A: Lo-Mendell-Rubin-adjusted likelihood ratio test; ssaBIC: Sample-size adjusted BIC.
In the 3 LC model distribution in frequency and percentage of participants was: LC1 n=190 (12.61%), LC2 n=1.160 (77.02%), and LC3 n=156 (10.35%). The average probability of belonging to its latent class was .96; .99 and .99, respectively. This result is indicative of the existence of a clear differentiation between the 3 groups of participants, with a participant belonging to an LC having a higher probability of belonging to that class and not to another.
The results of the 3 profiles are shown in Fig. 1. Within the LC1 there are teenagers with high scores in the dimensions of behaviour and hyperactivity problems, which is why it was called “externalizing”. The LC2, composed of participants with low scores in all the measurements and high in prosocial behaviour was called “low risk”. The LC3 was comprised of teenagers with high scores in problems with classmates and emotional problems, and was therefore called “internalising”.
Validation of latent profiles: relationship with subjective well-being, positive and negative affect, suicidal behaviour and attenuated psychotic experiences identified according to emotional and behavioural problems and prosocial behaviour.")
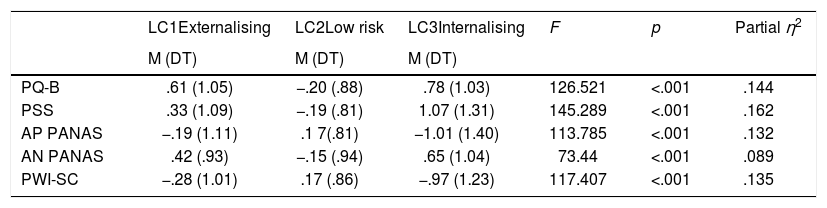
We analysed if the participants identified in the 3 latent profiles presented with a differential pattern regarding subjective well-being, positive and negative affect, suicidal behaviour and attenuated psychotic experiences. The MANCOVA indicated the existence of statistically significant experiences when all variables were considered jointly with the fixed factor of belonging to the latent class (Wilk's λ=.730, F(10,2990)=51.037; p<.001, partial η2=.146).
Table 2 contains statistical significance and effect size from the univariate variance analysis. It also contains the typified mean scores of the tools of measurement according to the latent profiles. Estimated effect sizes were high. In Fig. 2 there is a graphic representation of the mean scores in typified values.
Results from the MANCOVA for scores in socioemotional adjustment according to latent profiles.
| LC1Externalising | LC2Low risk | LC3Internalising | F | p | Partial η2 | |
|---|---|---|---|---|---|---|
| M (DT) | M (DT) | M (DT) | ||||
| PQ-B | .61 (1.05) | −.20 (.88) | .78 (1.03) | 126.521 | <.001 | .144 |
| PSS | .33 (1.09) | −.19 (.81) | 1.07 (1.31) | 145.289 | <.001 | .162 |
| AP PANAS | −.19 (1.11) | .1 7(.81) | −1.01 (1.40) | 113.785 | <.001 | .132 |
| AN PANAS | .42 (.93) | −.15 (.94) | .65 (1.04) | 73.44 | <.001 | .089 |
| PWI-SC | −.28 (1.01) | .17 (.86) | −.97 (1.23) | 117.407 | <.001 | .135 |
Typified values. AN PANAS: Negative affect; AP PANAS: Positive affect; LC: Latent class; PQ-B: Psychosis risk screening with the Prodromal questionnaire – brief version; PANAS: Positive and negative affect Schedule for children; PSS: Paykel suicide scale; PWI-SC: The Personal Well-being Index-School Children.

Comparisons in socioemotional adjustment according to latent profile groups. Typified values. AN PANAS: negative affect; AP PANAS: positive affect; LC: Latent class; PQ-B: Psychosis risk screening with the Prodromal questionnaire – brief version; PSS: Paykel suicide scale; PWI-SC: The Personal Well-being Index-School Children.
Regarding bullying at school, statistically significant differences were found between the 3 latent profiles in their perception of what this was (χ2(2)=33.665, p<.001), suffering from bullying as a victim (χ2(2)=106.35, p<.001), perception of cyberbullying (χ2(2)=15.072, p<.002) and suffering cyberbullying as a victim (χ2(2)=56.811, p<.001). In this sense, the group of no risk showed a lower degree and perception of bullying and cyberbullying compared with the groups at risk of mental health problems. Analysis of the externalizing and internalizing groups revealed that the internalising profile group had a higher prevalence of bullying and cyberbullying and victimization than the externalising profile group. Results are contained in Fig. 3.
 and their relationship with school bullying and cyberbullying.")
With reference to the relationship between the profiles and academic performance, statistically significant differences were found between the groups (χ2(8)=32.08, p<.001). Results are contained in Fig. 4. Thus, the low risk group had a lower number of fails and a higher number of good marks for the previous academic year compared with the externalizing and internalising problem risk groups. The externalizing and internalising problem groups were similar in academic performance.
Discussion and their relationship with academic performance.")
The aim of this study was to empirically identify homogenous groups of teenagers with differentiated patterns of emotional, behavioural and prosocial behavioural patterns. The relationship between latent profiles identified and socioemotional adjustment was analysed (e.g. emotional well-being, positive and negative affect, suicidal behaviour, attenuated psychotic experiences, (cyber) bullying and academic performance). To this end, a representative sample of teenagers from the general population was used and mixture modes, specifically the analysis of latent profiles. This methodology meant that subgroups of participants would be identified and classified using different prevention measures, such as early identification and detection and/or early intervention. The ultimate purpose was to try to prevent possible impact of mental health problems in young people at multiple levels (e.g. personal, school, family, social and health).
In this study we identified 3 latent profiles according to the emotional and behavioural problems and prosocial behaviour, calculated through use of the SDQ. The differentiated behavioural pattern corresponded with the groups: low risk, externalising and internalizing problems. The students with the externalising profile presented mainly with high scores in the dimensions relating to behavioural problems and hyperactivity. The students with the internalising profile obtained more markedly higher scores in problems with classmates and emotional problems. Finally, the students with the low risk – or protection – profile – showed low scores in al dimensions of SDQ difficulties and high prosocial behaviour, compared with the externalizing and internalizing profiles. It is noteworthy that the solution of grouping teenagers together into 3 sections, in view of the analysis on the SDQ difficulties and strengths, offered greater support to the mental health models which went beyond the “deficient” traditional view. For example, the model of positive development was more focused on the skills and strengths, and not so much on the limitation or difficulties of the teenager.46
In previous literature no studies were found to have examined latent classes or possible typologies of emotional and behavioural problems and prosocial behaviour in Spanish teenagers using the SDQ. However, previous studies have analysed groups of young people to identify patterns of emotional and behavioural problems using the SDQ and cluster analysis.15,16 For example, in the Bradshaw and Tipping16 study it was possible to divide the children together into 5 groups, based on their characteristics through 5 SDQ subscales. The group with the greatest prevalence was the one where the children had no emotional difficulties. Two groups of children arose with more problematic behaviour, one had scores in hyperactivity and lack of attention which was considerably higher, whilst the other had emotional difficulties higher than the mean, together with problems relating to behaviour, peers and hyperactivity. For its part, in the Ortuño-Sierra et al.15 study, with a sample of Spanish teenagers, 5 groups were found: (a) absence of emotional and behavioural difficulties with high scores in prosocial behaviour; (b) high scores in difficulties and low in prosocial behaviour; (c) high scores in hyperactivity and in prosocial skills; (d) high scores in emotional difficulties and relationships; and (e) high scores in difficulties of hyperactivity and medium scores in the other subscales of difficulties and in prosocial skills. At the same time, the results found were convergent with factorial studies which discovered the internalising and externalizing dimension both in the SDQ18 and in the Youth Self Report.47,48 Internationally, Ling et al.17 studied the SDQ using latent class analysis in a sample of 4121 Chinese teenagers (M=15.35, SD=1.70). The results supported a model of 3 latent classes (“group with major difficulties”, “non-cooperative group” and “well-adjusted group”), with fairly similar results to those found in this study. Specifically, the teenagers in the group with major difficulties, and the non-cooperative group were older, had parents in unstable marriages and a lower academic performance, compared with the group of low scores in the SDQ.
Also, differentiation was found between the latent profiles in the different personal adjustment, socioemotional and school indicators. Results showed the existence of a cognitive, emotional and behavioural pattern characteristic of each of the 3 established groups. In this sense, several results attest to this. First, the group with the internalising problems had higher mean scores in suicidal behaviour and poorer emotional well-being (subjective quality of life), compared with the other 2 groups. Second, the low risk group had a lower level and perception of bullying and cyberbullying compared with the externalising and internalising groups. Third, analysis of the groups with externalising and internalising problems revealed that the internalising profile group had a higher prevalence of perception of bullying and cyberbullying and of victimisation compared with the externalizing profile group. Fourth, the low risk group demonstrated higher academic performance indicators in the previous academic year, compared with groups with psychological difficulties. However, teenagers belonging to the groups of externalising and internalising problems demonstrated similar academic performance. Fifth, the groups who mostly referred to greater externalising or internalising problems, compared with the low risk group, reported higher attenuated psychotic experiences (a behavioural indicator of vulnerability to psychosis).49,50
The identification of similar subgroups in heterogeneous populations of young people who probably share a common set of emotional and behavioural difficulties is a relevant issue with clear practical implications. Establishing early detection and identification strategies, within a preventative and stratification model, in people at “high risk” of mental disorders, is an extremely interesting goal with clear practical implications. Also, and considering that research into early detection and identification is a book as yet unwritten in the field of mental health, in its initial phases, it is possible that some of the participants with a positive screening presented, de facto with higher vulnerability (at least theoretically) to develop psychopathological problems of a diverse nature. The combination of this propensity with other bio-psycho-social factors (e.g. substance abuse, traumatic experiences, urbanicity, family history of mental disorder), and the presence of malaise, concern and/or associated disability, leads to greater persistence of these experiences or symptoms, increasing the probability of leading to initial symptoms and the need for treatment.49–51 In this respect, it is interesting to highlight that internalizing problem groups and/or externalizing problem groups, as a general rule, presented with higher manifestations of suicidal behaviour (e.g. ideation, previous attempts, planning) and more attenuated psychotic experiences. This result is important, given that previous studies indicate that the combination of emotional problems (e.g. internalizing type or emotional imbalance) and the presence of subclinical psychotic experiences or symptoms increases the probability of future clinical symptoms.50–53 Thus, the combination of different mental health indicators may help to predict and prevent psychological disorders,12 whether or not they reach clinical threshold.
Several limitations should be considered when interpreting the findings obtained from this study. Firstly, conclusions are restricted by the self-reporting measurement tools used, with their corresponding limitations. Second, the sample belongs to a Spanish autonomous community (La Rioja), which partially limits generalisation to other populations and contexts, even though a random stratified sampling by conglomerates was made. Third, the cross-sectional nature of the study limits the establishment of cause and effect relationships. Fourth, the type of methodology used, an analysis of latent profiles, is based on a categorical classification, which may induce error, on the assumption that belonging to one group is stable and excludes the presence of problems related to other groups. Fifth, results could be considered affected by a broad amalgam of variables (individual, social, temporary, etc.) which did not form part of this study and which may have conditioned the results obtained. Future studies should therefore replicate the results found in this study. Sixth, the incorporation of confidence intervals from each teenage subgroup would have been of interest.
Over and above the before-mentioned limitations, this study constitutes an advance in the comprehension of child-teenage mental health. Depending on the results obtained strategies could be designed and implemented for the promotion of emotional well-being or prevention (e.g. early intervention) in this type of problem. The purpose would be to mitigates its possible impact at different levels (e.g. personal, educational, family, social or health), both present and future, and establish possible lines of action within the educational, social and healthcare policies (e.g. optimize resource management). Future studies should continue to longitudinally analyse young people identified with internalising and externalising problems and incorporate new forms of measurement and treatment, in keeping with assessment and out-patient intervention.54 Furthermore, the introduction of new aetiological models such as, for example the network model,55,56 may lead to a more complete comprehension of human behaviour.
FinancingThis research study was financed by the Instituto Carlos III, Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), by the 2015 call for BBVA Foundation Assistance to Researchers and Cultural Creators, by the BBVA Foundation 2017 Assistance to scientific research teams and co-financed by FEDER funds in the PO FEDER of La Rioja 2014-2020 (SRS 6FRSABC026).
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Fonseca-Pedrero E, Ortuño-Sierra J, Pérez-Albéniz A. Dificultades emocionales y conductuales y comportamiento prosocial en adolescentes: un análisis de perfiles latentes. Rev Psiquiatr Salud Ment (Barc.). 2020;13:202–212.