








Celiac plexus neurolysis (CPN) has been used to control pancreatic cancer (PC) pain, up to our knowledge, there is no study compared intraoperative CPN and computed tomography (CT)-guided techniques.
ObjectivesTo compare the effects of intraoperative and CT-guided CPN in unresectable PC on pain intensity and analgesic requirements.
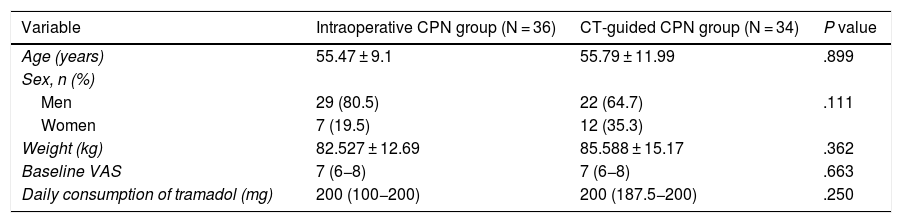
MethodsA total of 90 patients were enrolled in this prospective, randomized, open label, controlled, non-inferiority study, 20 patients were excluded or lost to follow up. The patients were randomly allocated to either intraoperative or CT-guided CPN group. A mixture of 20 mL ethanol 90%, 100 mg lignocaine and 5 mg dexamethasone was infused on each side of the aorta in both groups. Visual analogue score (VAS) and oral daily tramadol consumption were recorded at day 7, 14, 30, 60, 120 and 180 days after intervention. Occurrence of any intervention related complications were reported.
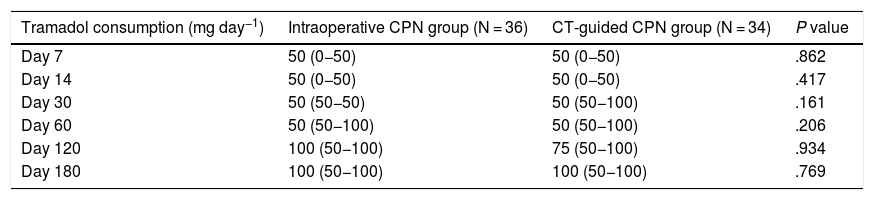
ResultsMedian VAS was similar in both intraoperative and CT-guided CPN groups from day 7 up to 180 days after intervention. The median daily analgesic consumption of oral tramadol (mg) was comparable in both intraoperative and CT-guided CPN groups after intervention at day 7 (50 versus 50), day14 (50 versus 50), day 30 (50 versus 50), day 60 (50 versus 50), day 120 (100 versus 75) and day 180 (100 versus 100). The incidence of diarrhea, vomiting, hypotension and back pain was similar in both groups.
ConclusionIntraoperative CPN is non-inferior to CT-guided CPN as both techniques were similarly associated with reduced pain severity and analgesics requirements.
Se ha utilizado la neurólisis del plexo celiaco (NCP) para controlar el dolor producido por el cáncer de páncreas (CP) y, a nuestro entender, no existe ningún estudio que compare las técnicas de NCP intraoperatoria y NCP guiada por tomografía computarizada (TC).
ObjetivosComparar los efectos de NCP intraoperatoria y NCP guiada por TC en el CP no operable en cuanto a intensidad del dolor y necesidad de analgésicos.
MétodosSe incluyó a un total de 90 pacientes en este estudio prospectivo, aleatorizado, abierto, controlado y de no inferioridad, en el que se excluyeron o perdieron 20 pacientes durante el seguimiento. Se asignó aleatoriamente a los pacientes en el grupo de NCP intraoperatoria o el grupo de NCP guiada por TC. En ambos grupos se inyectó una mezcla de 20 mL de etanol al 90%, 100 mg de lignocaína y 5 mg de dexametasona en cada lado de la aorta. Se registraron la escala analógica visual (EVA) y el consumo oral diario de tramadol los días 7º, 14º, 30º, 60º, 120º y 180º tras la intervención. Se reportó la presencia de cualquier complicación relacionada con la intervención.
ResultadosLa puntuación EVA media fue similar en ambos grupos de NCP intraoperatoria y NCP guiada por TC desde el 7º al 180º posteriores la intervención. El consumo medio diario de analgésico (mg de tramadol oral) fue comparable en ambos grupos tras la intervención en los días 7º(50 frente a 50), 14º(50 frente a 50), 30º(50 frente a 50), 60º(50 frente a 50), 120º(100 frente a 75) y 180º(100 frente a 100). La incidencia de diarrea, vómitos, hipotensión y dolor de espalda fue similar en ambos grupos.
ConclusiónLa NCP intraoperatoria no es inferior a la NCP guiada por TC, ya que la asociación de ambas técnicas a la reducción de la gravedad del dolor y a las necesidades de analgésicos fue similar.
