






Cardiac surgery (CS) is associated with a significant use of blood products. The aim of this study was to evaluate the effect of red blood cells concentrates (RBC) transfusion on regional cerebral oxygen saturation (SrO2) in patients undergoing CS with additive EuroSCORE I>6.
Material and methodsThis is a prospective descriptive study. Patients with additive EuroSCORE I>6 undergoing CS with extracorporeal circulation were included in the study. The demographic values, perioperative complications, hospital/ICU length of stay (LOS), as well as the preinduction baseline SrO2 values, the lowest SrO2 value during surgery, number of blood products transfused, hemoglobin (HB) and pre and postransfusional SrO2 values were recorded, and events of significant decrease in SrO2 below 20% of basal value or decrease below 50%. We considered responders those who had an increase post-transfusion SrO2 at least 20% of pre-transfusion value, an increase of standard deviation (7.9) or an increase up to basal SrO2.
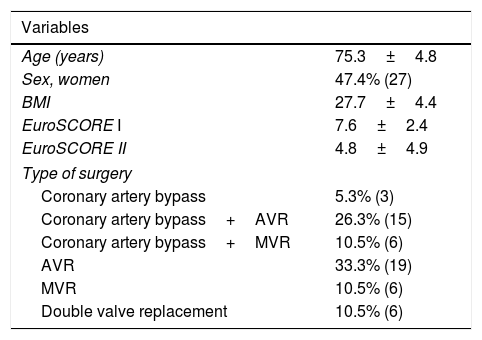
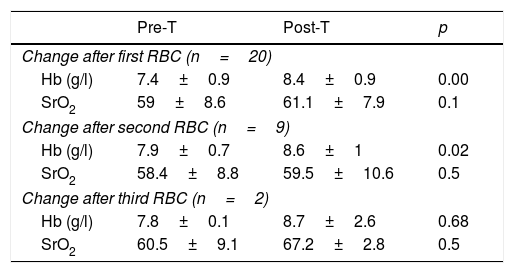
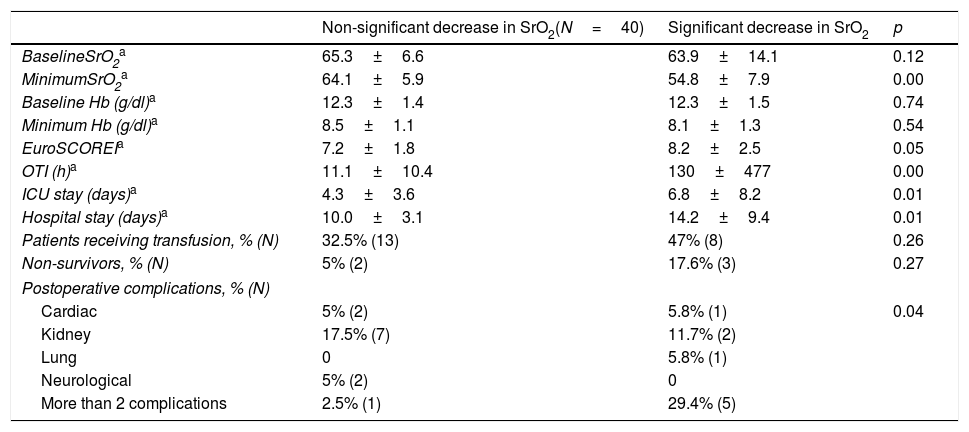
ResultsData from 57 patients were collected. The average additive EuroSCORE I was 7.4 (SD 2.6) and the EuroSCORE II was 6.1 (SD 7.4). 52% were male. 35.1% of patients received intraoperative transfusion of at least one unit of RBC. The overall mortality was 8.7% (N=5). During surgery 29.8% of the overall sample presented a decrease of more than 20% of baseline SrO2 or a value lower than 50%. Patients with a significant decrease in SrO2 presented a higher rate of perioperative complications (p=0.04) and longer ICU-LOS 4.3 (SD 3.6) vs. 6.8 (SD 8.2) days (p=0.01) and hospital LOS 10.1 (SD 3.1) vs. 14.2 (SD 9.4) days (p=0.01). Pretransfusional HB was 7.4 (SD 0.8) mg/dl and postransfusional value was 8.4 (SD 0.8) (p=0.00). Pretransfusional SrO2 was 59 (SD 8.6) and increased non- significantly after RBC transfusion to 61.1 (SD 7.9) (p=0.1). Only 6 patients out of 21 could be considered responders. There were no significant differences in morbidity, mortality or LOS between responders and non-responders.
DiscussionIn our population a non statistically significant increase in SrO2 was observed after RBC transfusion. When considering responders few patients were identified by SrO2. In conclusion SrO2 might not be reliable triger to decide transfusion.
La cirugía cardíaca se asocia a un uso significativo de hemoderivados. El objetivo de este estudio fue evaluar el efecto de la transfusión sobre la saturación regional de oxígeno cerebral (SrO2) en pacientes tratados mediante cirugía cardiaca con EuroSCORE I aditivo > 6.
Material y métodosEstudio prospectivo observacional. Se incluyó en el estudio a los pacientes con EuroSCORE I aditivo > 6 tratados mediante cirugía cardiaca con circulación extracorpórea. Se recogieron los valores demográficos, complicaciones perioperatorias, estancias hospitalarias, así como el valor de SrO2 basal preinducción, el valor más bajo de hemoglobina (Hb) registrado durante la cirugía, el valor de la Hb y la SrO2 pre y postransfusional, así como la existencia de una caída significativa de más del 20% del valor basal de la SrO2 o por debajo del 50%.
Consideramos como respondedores a la transfusión aquellos que presentaron un aumento de la SrO2 postransfusión de al menos el 20% del valor previo, un aumento de la desviación estándar (DE) (7,9) o un aumento hasta el nivel basal.
ResultadosSe recogieron los datos de 57 pacientes. El EuroSCORE I aditivo medio ± DE fue de 7,4 ± DE 2,6 y el EuroSCORE II fue de 6,1 ± DE 7,4. El 52% fueron varones. Se trasfundió al menos un concentrado de hematíes al 35,1% de la muestra (20 pacientes). La SrO2 pretransfusional fue 59 ± DE 8,6 y aumentó de forma no significativa tras la transfusión del primer CH (61,19 ± 7,9; p = 0,1). Un 29,8% de los pacientes presentaron durante la cirugía una disminución de la SrO2 del 20% con respecto a su basal o un valor inferior al 50%. Los pacientes con una disminución significativa de la SrO2 presentaron un mayor tasa de complicaciones perioperatorias (p = 0,04). La estancia en la Unidad de Cuidados Intensivos (UCI) fue mayor en los pacientes con una disminución significativa de la SrO2 respecto a los que la no presentaron (6,8 ± 8,2 días vs. 4,3 ± 3,6; p = 0,01) al igual que la estancia hospitalaria (14,2 ± 9,4 días vs. 10,1 ± 3,1; p = 0,01). En nuestra muestra, 6 de los 21 pacientes fueron respondedores. No hubo diferencias significativas en la morbilidad o la mortalidad entre los respondedores y los no respondedores.
DiscusiónEn nuestra población, se observó un aumento no significativo en la SrO2 tras la transfusión. Cuando se analizaron los respondedores a la transfusión por incrementos de SrO2, pocos pacientes fueron identificados como respondedores. En conclusión, la SrO2 podría no ser una herramienta que guíe la transfusión en pacientes tratados mediante cirugía cardiaca con EuroSCORE I aditivo > 6.
