




Osteoporosis is a multifactorial disease that increases in prevalence with age, and may be associated with fragility fractures. In Colombia there are few studies conducted on male osteoporosis.
ObjectiveTo describe the characteristics of men with osteoporosis who received care at the endocrinology outpatient clinic in two institutions in Manizales.
Materials and methodsDescriptive, cross-sectional study. The medical records of over 18-year old men that submitted a bone densitometry report to the endocrinology clinic from January 2009 to October 2018 were reviewed.
The results of the bone densitometry studies, the frequency of the types of osteoporosis, their etiology, risk factors, and the characteristics of fragility fractures were described.
ResultsA total of 417 medical records were reviewed, of which 303 met the eligibility criteria. The mean age was 66 years; 90 % of were over 50 old. Osteoporosis was diagnosed in 82.2 % of the men, with a higher frequency among those between 50 and 89 years old. 61 % had secondary osteoporosis, and the main causes were chronic use of glucocorticoids (42.1 %), hypogonadism (23.7 %), and hyperparathyroidism (16.4 %). 42.2 % presented with fragility fractures and the most common location was the spine (80 %).
ConclusionsThe diagnosis of osteoporosis was frequent among the male population in this trial; the most frequent type was secondary osteoporosis, and a significant percentage of men had fragility fractures.
La osteoporosis es una enfermedad multifactorial que aumenta su prevalencia con la edad y se puede asociar a fracturas por fragilidad. En Colombia son pocos los estudios realizados sobre osteoporosis en los hombres.
ObjetivoDescribir las características de los hombres con osteoporosis que asistieron a la consulta de endocrinología en 2 instituciones de la ciudad de Manizales.
Materiales y métodosEstudio descriptivo de corte transversal. Se revisaron las historias clínicas de hombres mayores de 18 años que asistieron con reporte de densitometría ósea a la consulta de endocrinología durante el período de enero de 2009 a octubre de 2018. Se describieron los resultados de las densitometrías, la frecuencia de los tipos de osteoporosis, su etiología, factores de riesgo y las características de las fracturas por fragilidad.
Resultados417 historias clínicas fueron revisadas, 303 cumplieron los criterios de elegibilidad. La edad media de los hombres fue de 66 años, el 90 % estaba por encima de los 50 años. Se diagnosticó osteoporosis en el 82.2 % de los hombres; más frecuente entre los 50 a 89 años. El 61 % tenía osteoporosis secundaria y sus principales causas fueron el uso crónico de glucocorticoides (42.1 %), el hipogonadismo (23.7 %) y el hiperparatiroidismo (16.4 %). El 42.2 % presentó fracturas por fragilidad y la localización más común fue la columna vertebral (80 %).
ConclusionesEl diagnóstico de osteoporosis fue frecuente en la población de hombres del presente estudio, el tipo más común fue la secundaria y se encontró un porcentaje significativo de hombres con fracturas por fragilidad.
Osteoporosis is defined as a deterioration of the bone mass and the bone microarchitecture, in addition to increased fragility that predisposes to the development of fractures.1 Osteoporosis is multifactorial and its prevalence increases with age. Furthermore, the presence of fragility fractures involves a higher morbidity and mortality.2
The actual number of men with osteoporosis is unknown, mainly as a result of the lower use of screening methods and to the controversies about the bone scan (DXA) standards in men.3 The epidemiology of male osteoporosis derives from a smaller number of studies as compared to women trials and the data vary according to the population studied. It has been said that the prevalence among white men is 7 %, 5 % among black men, and 3 % among Hispanics.4 It has been estimated that by 50 years of age, males have a risk of between 13 and 25% of experiencing an osteoporotic fracture over their lifetime, and this risk increases with age.5 Hip fracture is the most severe consequence of impaired bone strength; 50 % of males with a hip fracture fail to recover their functionality and independence and over 25 % die during the first year. Similarly, the survival rate associated with vertebral fractures is higher in women, with 84 % as compared to 72 % in males.4
Osteoporosis in males is associated with genetic considerations which are modulated via various hormonal, environmental, and nutritional factors.6 The disease is classified into 2 categories: primary and secondary. The primary category presents in men with no pathological condition or risk factor for low bone mass, and includes senile osteoporosis and idiopathic osteoporosis. Senile osteoporosis develops with aging; usually in subjects over 70 years old. Idiopathic osteoporosis is defined as one or more fractures and a low bone mineral density before 65–70 years of age. Secondary osteoporosis develops in males that present with a disease or receive treatment that causes low BMD.3 It is important to rule out any secondary causes, since the treatment in these patients may differ and the response may be limited if the underlying disorder is not identified or treated.7
Improved knowledge about male osteoporosis has further encourage our interest in research. There are few studies published in Colombia providing information about the characteristics of the disease in males in our population. The main purpose of this study was to describe the characteristics of men with osteoporosis who came for endocrinology consultation in Manizales. The results are expected to contribute to a better understanding of the pattern of development of the disease in our setting, in order to guide the development of healthcare strategies that positively impact on the prevention, the evolution, and the prognosis of osteoporosis in men.
Materials and methodsA descriptive, cross-sectional study was designed in males who came for an endocrinology consult at 2 institutions in Manizales. The medical records that met the eligibility criteria were included in the study. The inclusion criteria were: male, over 18 years old, having the results of a DXA study, and coming for an endocrinology consultation at the E.S.E Hospital Departamental Universitario Santa Sofía de Caldas or the Endocrinology office at the Centro de Especialistas, between January 1st, 2009 and October 15, 2018. The exclusion criteria were: A DXA result based on an inadequate technique or a poor report for interpretation, and incomplete medical records.
Convenience sampling was used based on the consults of men during the established period of time. The information of patients derives from their electronic medical record. An instrument was designed to collect the relevant variables and a database was developed using Microsoft® Excel® 2013.
The following variables were collected from all the medical records: age, reason for consultation, history of osteoporosis and DXA results. In addition of the medical records of men with a diagnosis of osteoporosis, disease-associated variables were also collected: age at the time of diagnosis, type of osteoporosis, etiology, presence of risk factors such as diseases and drugs described in the literature, family history of osteoporosis, presence of fragility fractures and characteristics (how many, location, ad complications). Lifestyle variables: smoking, frequent alcohol use, frequent exercise. Physical examination variables: weight, size, body mass index. Treatment variables: anti-osteoporosis agents and supplements. Laboratory variables: serum calcium, serum phosphorus, urine calcium in 24 h, PTH, 25-hydroxyvitamin D, creatinine, testosterone and alkaline phosphatase.
The DXA was classified in accordance with the WHO criteria and the International Society for Clinical Densitometry. For subjects over 50 years old, the T-score used considered normal a result ≥ −1.0 standard deviations (SD); osteopenia between −1.0 and −2.5 (SD), osteoporosis ≤ −2.5 (SD), and severe osteoporosis in the presence of a fragility fracture. In men less than 50 years old, the Z score was used, establishing osteoporosis with a score of −2 (SD) and a fragility fracture.8,9
Considering the type of trial and its methodology, the information about the variables with respect to the DXA result, the type of osteoporosis, the etiology, risk factors, inter alia, corresponds to the clinical judgement of the specialists who completed the medical records. The BMI was classified according to the WHO classification: low weight, <18.5; normal, 18.5–24.9; overweigh, 25–29.9; obesity grade I, 30–34.9; obesity grade II, 35–39.9; and obesity grade III, ≥ 40.10 Moreover, the results of the tests are from different laboratories and not from a single standardized laboratory. Vitamin D insufficiency was defined as levels of 25-hydroxyvitamin D below 30 ng/ml, and deficiency, as levels below 20 ng/ml.
A descriptive analysis of the study variables was conducted using central tendency measures, dispersion measures, frequencies and proportions in accordance with the nature of the data. Frequency tables or charts were developed based on the presence or absence of each risk factor. Contingency tables were drawn for the analysis of the variables, and the Chi square test was used. The data processing and analysis was conducted using IBM® SPSS® Statistics version 25.
The study was approved by the bioethics committee of the School of Health Sciences of the Caldas University, and by the committee of medical records of each institution where the information was collected.
Results417 medical records of men with DXA, seen between January 1st, 2009 and October 15, 2018 seen by three endocrinology specialists from 2 institutions in Manizales were reviewed; 303 medical records met the eligibility criteria.
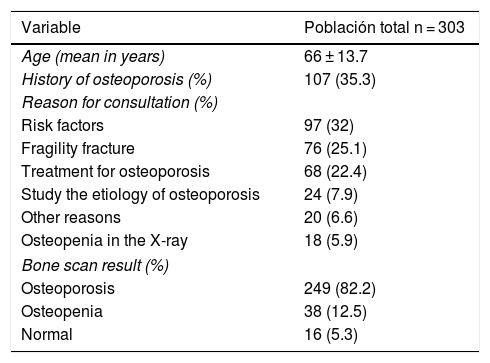
The mean age of these men was 66 years, with a minimum age of 20 years and a maximum of 96 years. 90 % (273 of 303 men) were older than 50 years. During the first endocrinology visit, 35.3 % (107 of 303 men) had a previous diagnosis of osteoporosis and the main reasons for consultation were the identification of risk factors associated with a low BMD (32 %), fragility fracture (25.1 %), and the request for osteoporosis treatment (22.4 %). 82.2 % (249 of 303 men) had a DXA result compatible with osteoporosis, 12.5 % (38 men) with osteopenia, and 5.3 % (16 men) were normal (Table 1).
Characteristics of the men who consulted for endocrinology assessment.
| Variable | Población total n = 303 |
|---|---|
| Age (mean in years) | 66 ± 13.7 |
| History of osteoporosis (%) | 107 (35.3) |
| Reason for consultation (%) | |
| Risk factors | 97 (32) |
| Fragility fracture | 76 (25.1) |
| Treatment for osteoporosis | 68 (22.4) |
| Study the etiology of osteoporosis | 24 (7.9) |
| Other reasons | 20 (6.6) |
| Osteopenia in the X-ray | 18 (5.9) |
| Bone scan result (%) | |
| Osteoporosis | 249 (82.2) |
| Osteopenia | 38 (12.5) |
| Normal | 16 (5.3) |
The diagnosis of osteoporosis was made in all age groups, with a higher frequency in subjects between 50 and 89 years old (92.8 %), with a peak between 70 and 79 years (29.3 %). Osteopenia was more common between 40 and 89 years old (89.6 %), and normal results between 30 and 69 years old (93.9 %) (Fig. 1).

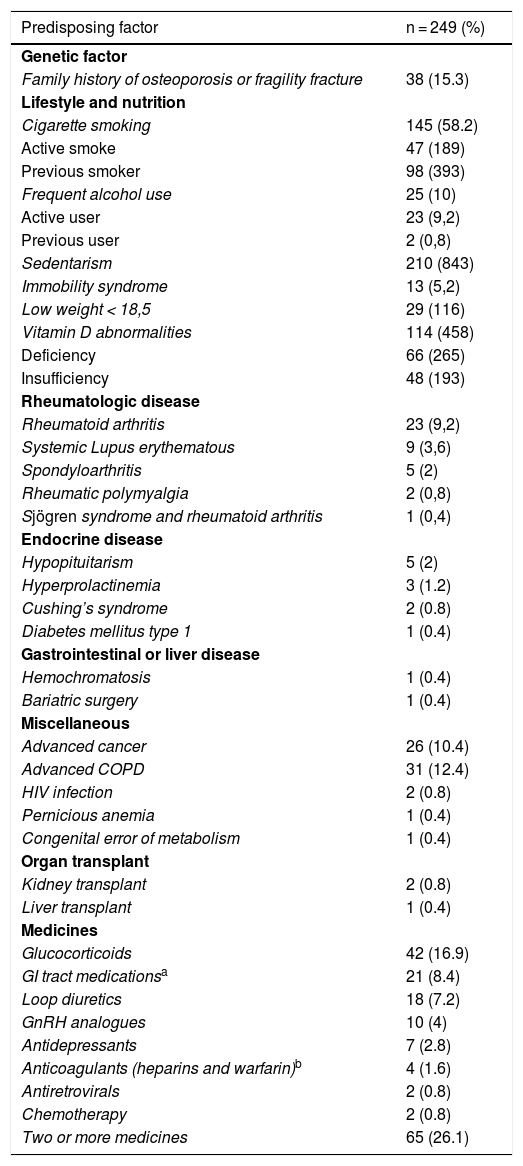
The most frequent type of osteoporosis among all the various age groups was secondary osteoporosis, with 61 % (152 of 249 men), while 39 % (97 males) were classified as primary osteoporosis and it was found that of these, 94.8 % (92 males) had at least one risk factor for low BMD. With regards to risk factors, 64.3 % (160 of 249 men) had at least one predisposing disease and 68.7 % (171 of 249 men) had at least one medication prescribed associated with low BMD. The most frequent medications were glucocorticoids (16.9 %), GI medicines including proton pump inhibitors and anti-acids, (8.4 %) and loop diuretics (7.2 %). 26.1 % had 2 or more drugs prescribed.
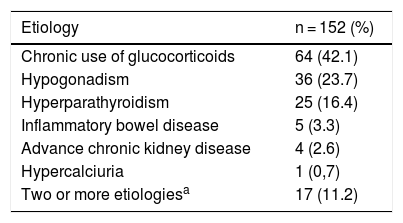
The main causes of secondary osteoporosis were the chronic use of glucocorticoids (42.1 %), hypogonadism (23.7 %), and hyperparathyroidism (16.4 %). 11.2 % of the men had 2 or more etiologies (Table 2). In the case of glucocorticoid-induced osteoporosis, the reasons for prescribing these medications were: rheumatoid arthritis (43.8 %), non-specified arthritis (29.7 %), systemic autoimmune diseases (15.6 %), adrenal failure (6.2 %) and transplants (4.7 %).
Etiology of secondary osteoporosis in men.
| Etiology | n = 152 (%) |
|---|---|
| Chronic use of glucocorticoids | 64 (42.1) |
| Hypogonadism | 36 (23.7) |
| Hyperparathyroidism | 25 (16.4) |
| Inflammatory bowel disease | 5 (3.3) |
| Advance chronic kidney disease | 4 (2.6) |
| Hypercalciuria | 1 (0,7) |
| Two or more etiologiesa | 17 (11.2) |
The mechanisms of hypogonadism-induced osteoporosis were identified as secondary hypogonadism (47.2 %), pharmacologic castration (22.2 %), primary hypogonadism (22.2 %), and surgical castration (8.3 %). With the exception of one case associated with trauma, all cases of pharmacologic and surgical castration were due to prostate cancer. In the cases of osteoporosis secondary to hyperparathyroidism, the most frequent type was the one secondary to Vitamin D deficit (88 %), followed by the primary (12 %).
In terms of lifestyle, 58.2 % (145 of 249 men) had a history of smoking; 18.9 % were active smokers, and 39.3 % had quit smoking. 10 % (25 of 249 men) reported frequent alcohol use; 9.2 % active alcohol use and 0.8 % previous use. 10.5 % (26 of 249 men) reported frequent physical activity, while 84.3 % reported sedentarism and 5.2 % had immobility syndrome. On the other hand, 11.6 % (29 of 249 men) had low body weight. A family history of osteoporosis or fragility fracture represented 15.3 %. Table 3 summarizes the risk factors for low BMD found in men with osteoporosis.
Risk factors for low mineral bone density in men with osteoporosis.
| Predisposing factor | n = 249 (%) |
|---|---|
| Genetic factor | |
| Family history of osteoporosis or fragility fracture | 38 (15.3) |
| Lifestyle and nutrition | |
| Cigarette smoking | 145 (58.2) |
| Active smoke | 47 (189) |
| Previous smoker | 98 (393) |
| Frequent alcohol use | 25 (10) |
| Active user | 23 (9,2) |
| Previous user | 2 (0,8) |
| Sedentarism | 210 (843) |
| Immobility syndrome | 13 (5,2) |
| Low weight < 18,5 | 29 (116) |
| Vitamin D abnormalities | 114 (458) |
| Deficiency | 66 (265) |
| Insufficiency | 48 (193) |
| Rheumatologic disease | |
| Rheumatoid arthritis | 23 (9,2) |
| Systemic Lupus erythematous | 9 (3,6) |
| Spondyloarthritis | 5 (2) |
| Rheumatic polymyalgia | 2 (0,8) |
| Sjögren syndrome and rheumatoid arthritis | 1 (0,4) |
| Endocrine disease | |
| Hypopituitarism | 5 (2) |
| Hyperprolactinemia | 3 (1.2) |
| Cushing’s syndrome | 2 (0.8) |
| Diabetes mellitus type 1 | 1 (0.4) |
| Gastrointestinal or liver disease | |
| Hemochromatosis | 1 (0.4) |
| Bariatric surgery | 1 (0.4) |
| Miscellaneous | |
| Advanced cancer | 26 (10.4) |
| Advanced COPD | 31 (12.4) |
| HIV infection | 2 (0.8) |
| Pernicious anemia | 1 (0.4) |
| Congenital error of metabolism | 1 (0.4) |
| Organ transplant | |
| Kidney transplant | 2 (0.8) |
| Liver transplant | 1 (0.4) |
| Medicines | |
| Glucocorticoids | 42 (16.9) |
| GI tract medicationsa | 21 (8.4) |
| Loop diuretics | 18 (7.2) |
| GnRH analogues | 10 (4) |
| Antidepressants | 7 (2.8) |
| Anticoagulants (heparins and warfarin)b | 4 (1.6) |
| Antiretrovirals | 2 (0.8) |
| Chemotherapy | 2 (0.8) |
| Two or more medicines | 65 (26.1) |
COPD: Chronic obstructive pulmonary disease; GnRH: Gonadotropin releasing hormone; HIV: Human immunodeficiency virus.
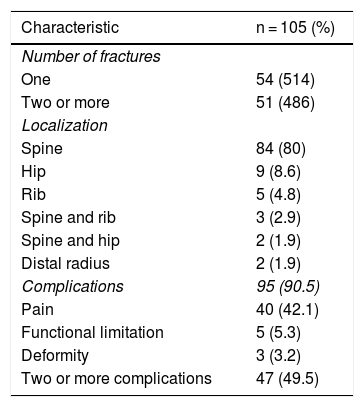
Fragility fractures were reported in 42.2 % (105 of 249 males), more frequent in men between 50 and 89 years old (93.4 %). 51.4 % had one single fracture and 48.6 % presented with 2 or more fractures. The most frequent location was the spine (80 %), followed by the hip (8.6 %). 90.5 % (95 of 105 men) presented complications associated with fractures; while pain was the most frequent complication (42.1 %), 49.5 % presented with 2 or more complications (Table 4).
Characteristics of fragility fractures in men with osteoporosis.
| Characteristic | n = 105 (%) |
|---|---|
| Number of fractures | |
| One | 54 (514) |
| Two or more | 51 (486) |
| Localization | |
| Spine | 84 (80) |
| Hip | 9 (8.6) |
| Rib | 5 (4.8) |
| Spine and rib | 3 (2.9) |
| Spine and hip | 2 (1.9) |
| Distal radius | 2 (1.9) |
| Complications | 95 (90.5) |
| Pain | 40 (42.1) |
| Functional limitation | 5 (5.3) |
| Deformity | 3 (3.2) |
| Two or more complications | 47 (49.5) |
Most of the lab results were normal; 45.8 % (114 of 249 men) presented 25-hydroxyvitamin D abnormalities: 26.5 % due to deficit, and 19.3 % due to insufficiency. PTH was high in 14.5 % of the subjects and testosterone was low in 13.7 % of the cases, corresponding to cases of hypothyroidism and hypogonadism, respectively.
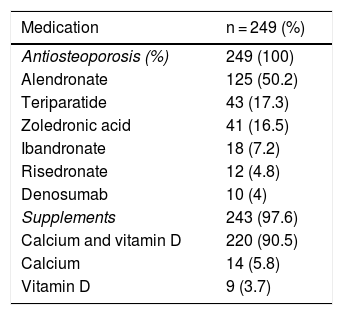
100 % of the men with osteoporosis were prescribed anti-osteoporotic medication and alendronate was the most frequently prescribed drug (50.2 %). Supplements were prescribed in 97.6 % of patients, and the most frequent was the calcium vitamin D combination (90.5 %) (Table 5).
Pharmacological therapy prescribed to men with osteoporosis.
| Medication | n = 249 (%) |
|---|---|
| Antiosteoporosis (%) | 249 (100) |
| Alendronate | 125 (50.2) |
| Teriparatide | 43 (17.3) |
| Zoledronic acid | 41 (16.5) |
| Ibandronate | 18 (7.2) |
| Risedronate | 12 (4.8) |
| Denosumab | 10 (4) |
| Supplements | 243 (97.6) |
| Calcium and vitamin D | 220 (90.5) |
| Calcium | 14 (5.8) |
| Vitamin D | 9 (3.7) |
The primary reason for consultation of males was the identification of risk factors (32 %), followed by pathological fractures (25.1 %), which means that one fourth of the men consulted because of severe osteoporosis; this should further encourage the search and intervention of the disease and of the risk factors in our setting.
The prevalence of male osteoporosis increases with aging, particularly among those who are ≥ 70-year old.11 In our study, the diagnosis was more frequent between 50 and 89 years, with a peak between 70 and 79 years, which is consistent with the studies including male populations in Latin America and Colombia.12–15 The most frequent type of osteoporosis was secondary osteoporosis (61 %), similar to what is described in the literature above 50 %, while primary osteoporosis is reported at 30–40 %.7,16–18 Jaller et al., in a study on male osteoporosis conducted in Barranquilla, reported secondary osteoporosis in 62.2 %.13
The main causes of osteoporosis were the chronic use of glucocorticoids, hypogonadism, and hyperparathyroidism. Although alcohol abuse has been described as a frequent cause, this was not the case in our study (10 %).4,6,11 This low frequency as a cause or predisposing factor has also been identified in other trials; probably because of the different consumption habits around the world.13,15 In the study by Jaller et al., the principal causes were cigarette smoking, chronic use of glucocorticoids and rheumatoid arthritis. We found; cigarette smoking (58.2 %), chronic use of glucocorticoids (42.1 %), as the most predisposing medication (16.9 %), and rheumatoid arthritis (9.2 %) as the most common rheumatological disease and the main reason for prescribing glucocorticoids (43.8 %). This latter finding is similar to the report of the study by Caballero et al. on glucocorticoid-induced osteoporosis conducted in Barranquilla.19 Although the study by Jaller et al. was also descriptive, they had a smaller number of men with osteoporosis and less complementary studies that may probably have increased the prevalence of secondary causes.13
In terms of glucocorticoid-induced osteoporosis, about 30–50 % of those receiving these drugs will experience a fracture.20 In 2013, a study on the prophylactic prescription for osteoporosis in patients who are chronic users of glucocorticoids in Colombia, Manizales was number two in the ranking of cities with the highest prescription of glucocorticoids, and also of those that failed to receive prophylaxis.21 Consequently, and considering also the results of this study we feel it is important to constantly assess the indications and dosing of patients receiving these drugs.
11.2 % of the men with osteoporosis had 2 or more causes recorded and in most cases, in addition to the causes, other risk factors were identified. 64.3 % had at least one disease and 68.7 % had prescribed at least one medication as a risk factor. One of the highlights is that 94.8 % of the men with primary osteoporosis had at least one risk factor for low BMD. A study in Venezuela reported that 100 % of the men with osteoporosis and osteopenia had risk factors.14 Likewise, the study by Ryan et al. reported that most of the men referred to an osteoporosis clinic has multiple risk factors and potential secondary causes.22
There is an overlap between what is considered to be a risk factor for primary osteoporosis and a cause of secondary osteoporosis; this is evidenced by the broad range of the results from the studies.5 Secondary osteoporosis maybe caused by different entities, in which bone loss may be associated with one single cause or by with a combination of multiple factors. Hence, the identification of the primary cause of osteoporosis may often prove to be challenging.23,24
Low weight was infrequent (11.6 %); probably this has to do with the presence of factors such as sedentarism, use of glucocorticoids, and hypogonadism; however, a different type of methodology is needed to establish these associations.
Only 10.5 % of the men exercised regularly, which is a low frequency for a protective factor. However, other studies have also reported low frequencies.25
Approximately one of every 4 men over 50 years old presents at least one fragility fracture associated with higher morbidity and mortality, as compared against females.6 Our study population presented with high risk factors for fractures, including old age, the use of glucocorticoids, rheumatoid arthritis, and secondary osteoporosis. Fragility fractures were present in 42.2 % of men; almost one half of the cases had 2 or more fractures, with the spine being the most frequent site (80 %). Most men presented complications associated with fractures.
A study on fragility fractures conducted in Bogotá, which included a low percentage of males, reported a fracture prevalence of 46 %. The most frequent anatomical sites were the distal radius, the spine, and the femur.15 Another study on male osteoporosis conducted in Chile reported a higher frequency of fractures (51.4 %), mostly in the spine (55 %).26
The spine is a common site for fragility fractures; their presence predicts new fractures and is associated with higher mortality.17,27,28 The high frequency of these fractures in our study is probably related to a higher BMD loss in the spine and to the age of occurrence of the fractures; however, the type of the study and the content of the medical records limited the capture of these variables. Moreover, it must be kept in mind that the sample is derived from a selected population of a clinical subspecialty, where the most complex cases among the general population are expected to be found. It would be interesting to further research fragility fractures in men in our setting.
In the studies, low vitamin D levels have been variable (50–80 %); probably because of differences in the definition of insufficiency and deficiency, measurement techniques, and sun exposure.29–31 We found a low vitamin D level in 45.7 % of the men, and more than half of the cases were vitamin D deficit. A study on Vitamin D in patients with osteoporosis conducted in Cali reported a prevalence of insufficiency of 55.3 %.32
With regards to treatment, there are few randomized clinical trials assessing the efficacy of various drugs against osteoporosis and reduced risk of fracture in men. In a meta-analysis and systematic review conducted by Nayak and Greenspan, they found that bisphosphonates – as a class of drugs – significantly reduced the risk of vertebral fracture and probably non-vertebral as well, making it the treatment of choice for male osteoporosis, in particular alendronate and risedronate. 33 Zoledronic acid is the only intravenous bisphosphonate with proven efficacy in the prevention of fractures in men, while other agents such as ibandronate do not have the same level of evidence.34,35
Teriparatide and denosumab have shown in randomized controlled trials an increase in BMD in men with osteoporosis, and are the drugs of choice in men with a high risk of fractures.36–38 It is important to emphasize that male osteoporosis is usually secondary and in a high percentage severe; hence, evidence-supported medications must be used in this population.
In our study, all men were prescribed anti-osteoporotic therapy; oral bisphosphonates were the most widely used, and the majority received supplements, mainly calcium and vitamin D, similar to the reports of other studies.39,40
ConclusionsThis study gives information on the characteristics of a male population with osteoporosis and the data are derived from a clinical subspecialty in Manizales. Osteoporosis was a frequent occurrence in males who consulted with DXA results. The most frequent type was secondary osteoporosis and the major causes were the chronic use of glucocorticoids, hypogonadism, and hyperparathyroidism. Most of the men presented high risk factors for fractures and a high frequency of severe osteoporosis was detected, in addition to a preponderance of fragility fractures in the spine. The most frequently used drugs were oral bisphosphonates, rather than the drugs with stronger evidence of efficacy in men with a high risk of fractures, such as zoledronic acid, denosumab and teriparatide.
The strengths of the trial are the sample size and the fact that this is the first publication in our region, and one of the few existing in Colombia on osteoporosis in men. The limitations are that because of the type of study depending on the content of the medical records, no significant variables could be measured: sociodemographic, age at the time of sustaining the pathological fracture, falls risk, calcium intake, sun exposure, and further details such as the type of drugs and lifestyle.
The study was conducted in a selected male population of the endocrinology clinic and hence the results may not be extrapolated to the general population. Nevertheless, the results are considered to be of interest for healthcare professionals who take care of this type of patients.
FinancingNo financing was received. This paper was not supported by any grant or funding from the pharmaceutical industry.
Conflict of interestThe authors have no conflicts of interest to disclose.
Please cite this article as: Sánchez Lozada A, de la Portilla Maya DA. Osteoporosis en hombres de la consulta de endocrinología en la ciudad de Manizales, Colombia. Rev Colomb Reumatol. 2019;26:247–254.
