







To determine the diagnostic performance of ultrasound-guided core-needle biopsy in thyroid nodules after two inconclusive fine-needle aspiration biopsies. To assess the complications of core-needle biopsy. To analyze the reliability of diagnoses obtained with core-needle biopsy. To measure the economic impact of avoiding lobectomies in patients with benign core-needle biopsy findings.
Material and methodsThis retrospective study reviewed 195 core-needle biopsies in 178 patients. To determine the reliability of the core-needle biopsy findings, we compared the diagnosis from the core-needle specimen versus the histologic findings in the surgical specimens when core-needle biopsy findings indicated malignancy or follicular proliferation and versus the stability of the nodule on ultrasound follow-up for one year when core-biopsy findings indicated benignity.
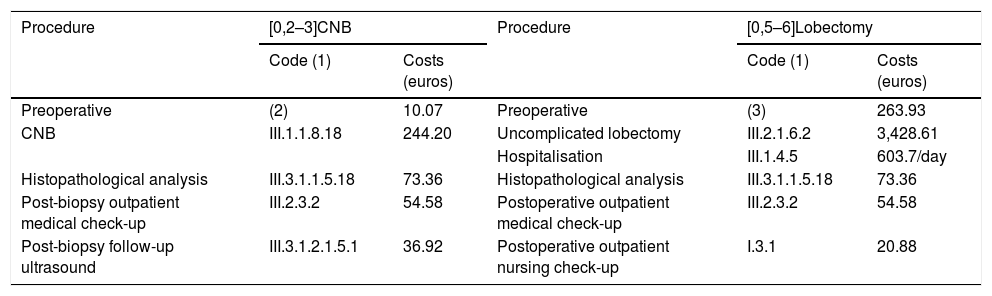
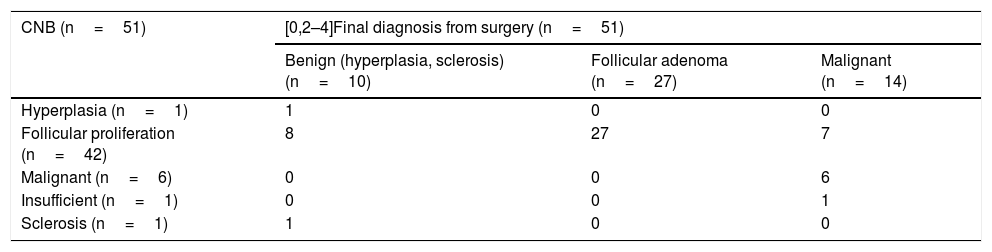
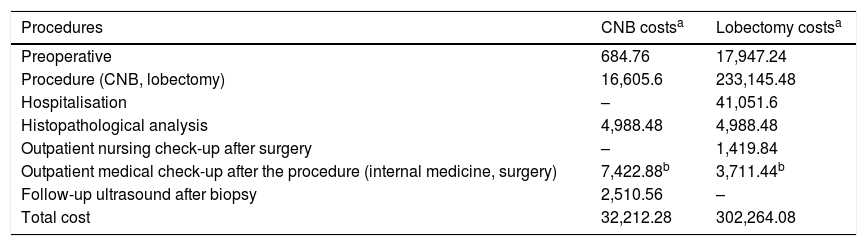
ResultsCore-needle biopsy yielded a diagnosis for 179 (91.7%) nodules, of which 122 (62.5%) were classified as benign, 50 (25.6%) as follicular proliferation, and 7 (3.6%) as malignant. The findings were inconclusive for 16 (8.3%) nodules. Minor complications were observed in 4 (2%) patients; no major complications were observed. The sensitivity of core-needle biopsy for the diagnosis of thyroid cancer was low (42.8%) because the technique was unable to detect capsular or vascular invasion, although the specificity and positive predictive value (PPV) were 100%. However, when we considered histologic findings of malignancy and follicular proliferation positive because both require surgical resection, the sensitivity increased to 97.5% and the PPV decreased to 83.3%. There were 79 nodules with ultrasound follow-up for at least one year; 76 (96.2%) had negative core-needle biopsy findings, and 74 (97.3%) of these remained stable. The negative predictive value (NPV) for malignancy of the benign nodules was 98.6%, although no malignant transformation was observed. Nevertheless, the results of the statistical analysis do not allow us to recommend forgoing ultrasound follow-up in patients with benign core-biopsy findings. The cost savings of avoiding lobectomy in patients with benign nodules and stability of the nodule on ultrasound follow-up for at least one year was about 90%.
ConclusionsCore-needle biopsy of thyroid nodules is effective because it diagnoses more than 90% of nodules with inconclusive findings after fine-needle aspiration biopsy. It is safe if done by experienced professionals. It is reliable because it yields 100% specificity and 100% PPV for malignant nodule, 97.5% sensitivity for the detection of nodules that require surgery, and 98.6% NPV for benign nodules. It is efficient because it reduces the costs of diagnosis compared to lobectomy in benign nodules.
Conocer el rendimiento diagnóstico de la biopsia con aguja gruesa (BAG) ecoguiada en nódulos tiroideos con dos punciones aspirativas con aguja fina (PAAF) previas no diagnósticas. Evaluar complicaciones de la BAG. Analizar la fiabilidad de los diagnósticos obtenidos mediante BAG. Medir el impacto económico de evitar lobectomía tras BAG con resultado benigno.
Material y métodosRevisión retrospectiva de 195 BAG realizadas en 178 pacientes. Las referencias utilizadas para medir la fiabilidad de los resultados de la BAG fueron el análisis de la pieza quirúrgica tras una biopsia con malignidad o proliferación folicular (PF) y la estabilidad ecográfica superior a 1 año tras una BAG benigna. Se compararon costes directos de BAG más seguimiento ecográfico frente al que hubiera tenido realizar lobectomía sin complicaciones en los pacientes con estabilidad ecográfica superior a 1 año tras BAG benigna.
ResultadosDe los 195 nódulos sometidos a BAG, el resultado fue diagnóstico en 179 (91,7%), incluyendo 122 benignos (62,5%), 50 PF (25,6%) y 7 malignos (3,6%). No fue diagnóstico en 16 nódulos (8,3%). Hubo complicaciones menores en 4 pacientes (2%) y mayores en ninguno. La sensibilidad de la BAG para el diagnóstico de cáncer de tiroides fue baja (42,8%) por su incapacidad para detectar invasión capsular o vascular, aunque con especificidad y valor predictivo positivo (VPP) del 100%. Al considerar los diagnósticos de malignidad y PF como positivos, pues ambos obligan a resección quirúrgica, la sensibilidad ascendió al 97,5%, con descenso al 83,3% del VPP. Hubo 79 nódulos con seguimiento ecográfico superior a 1 año, 76 con BAG benigna (96,2%), de los cuales mostraron estabilidad 74 (97,3%). El valor predictivo negativo (VPN) para malignidad de los nódulos benignos fue del 98,6%, aunque no se detectó ninguna transformación maligna. Sin embargo, el análisis estadístico no permite recomendar la supresión del seguimiento ecográfico tras BAG benigna. La reducción del coste diagnóstico respecto a lobectomía en pacientes con nódulos benignos y estabilidad ecográfica superior a 1 año fue próxima al 90%.
ConclusionesLa BAG de tiroides es efectiva porque diagnostica más del 90% de los nódulos con PAAF no diagnósticas; segura si es realizada por personal experimentado; fiable porque presenta especificidad y VPP del 100% en nódulos malignos, sensibilidad del 97,5% para detectar que nódulos necesitan cirugía y VPN del 98,6% en nódulos benignos; y eficiente porque reduce los costes diagnósticos respecto a lobectomía en nódulos benignos.

