







Lung retransplantation (LR) is a valid choice with a significant risk of perioperative morbidity and mortality in selected patients with graft dysfunction after lung transplantation. Our goal is to analyse our experience in LR in terms of survival and lung function.
MethodsRetrospective study of patients undergoing LR (1990–2019). Variables: recipients and procedure, early mortality, survival and lung function in patients with CLAD. Quantitative variables (mean±SD); qualitative (%). Student's t test or χ2 was used. Survival was estimated using Kaplan–Meier, compared with Log Rank. A p<0.05 was established as significant.
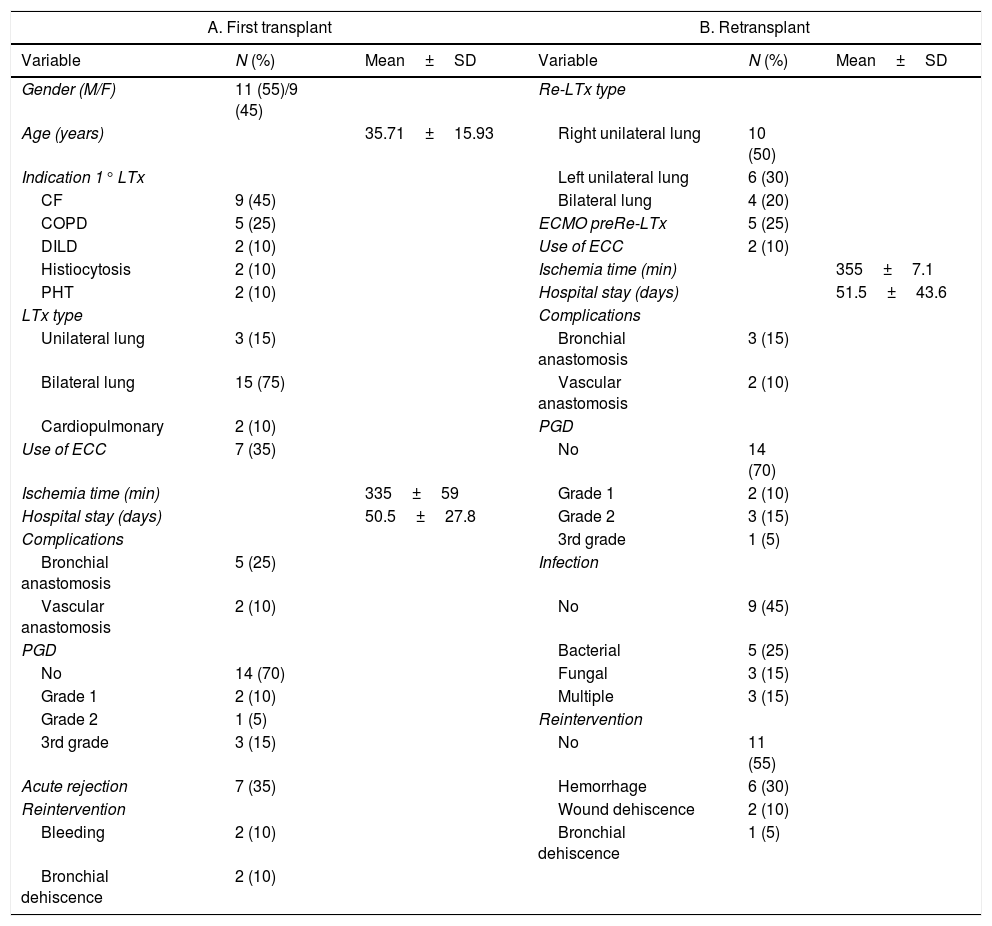
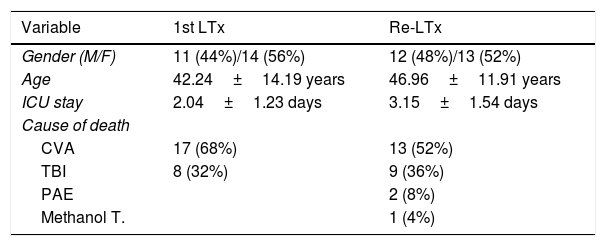
ResultsOf 784 transplanted patients, 25 patients (mean age 38.41–16.3 years, 12 men and 13 women) were LR; CLAD (n=19), pulmonary infarction (n=2), airway complications (n=2), graft dysfunction (n=1), hyperacute rejection (n=1), mean time to retransplantation: 5.41±3.87 years in CLAD and 21.2±21.4 days in non-CLAD.
The 90-day mortality was 52% and 36.8% in the second period (p=0.007), being higher in patients who required preoperative ECMO (80% vs. 20%, p=0.04).
The 1- and 5-year survival was 53.9% and 37.7%, respectively (p=0.016). Survival of the CLAD group was greater (p=0.08). Pre LR ECMO decreased survival (p=0.032).
After LR, FEV1 improved an average of 0.98±0.13L (25.6±18.8%) (p=0.001).
ConclusionsLR is a high mortality procedure that requires careful selection of patients with better results in patients with CLAD. The lung function of patients with CLAD improved significantly.
El retrasplante pulmonar (RTP) es un tratamiento válido en pacientes con disfunción pulmonar, pero con una elevada morbimortalidad. Nuestro objetivo es analizar nuestra experiencia en RTP en supervivencia y función pulmonar.
Pacientes y métodosEstudio retrospectivo de pacientes con RTP (1990-2019). Variables: receptores y procedimiento, mortalidad precoz, supervivencia y función pulmonar en pacientes CLAD. Variables cuantitativas (media±DE); cualitativas (%). Se utilizó el test t de Student o χ2. La supervivencia se estimó mediante Kaplan-Meier, comparándose con Log Rank. Se estableció como significativa p<0,05.
ResultadosDe 784 pacientes trasplantados, 25 pacientes (edad media 38,41±16,3 años, 12 hombres y 13 mujeres) fueron RTP; CLAD (n=19), infarto pulmonar (n=2), complicaciones de vía aérea (n=2), disfunción del injerto (n=1), rechazo hiperagudo (n=1). Tiempo medio hasta el retrasplante: 5,41±3,87 años en CLAD y 21,2±21,4 días en no CLAD.
La mortalidad a 90 días fue del 52% y 36,8% en el segundo periodo (p=0,007), siendo mayor en pacientes que precisaron ECMO preoperatorio (80 vs. 20%, p=0,04).
La supervivencia a 1 y 5 años fue del 53,9% y 37,7%, respectivamente (p=0,016). La supervivencia del grupo CLAD fue mayor (p=0,08). El ECMO pre RTP disminuyó la supervivencia (p=0,032). FEV1 mejoró una media de 0,98±0,13L (25,6±18,8%) (p=0,001).
ConclusionesEl RTP es un procedimiento de elevada mortalidad que obliga a una cuidadosa selección de los pacientes, con mejores resultados en aquellos con CLAD. La función pulmonar de los pacientes con CLAD mejoró significativamente.
