




The aim of this study was to evaluate the characteristics of fever of unknown origin (FUO) according to the definition with qualitative study criterion and of patients without diagnosis.
Materials and methodsProspective observational study performed from 2009 to 2017 of all patients who were diagnosed with FUO according to the extended definition with qualitative study criterion. Demographic, clinical, diagnostic and evolving variables were evaluated.
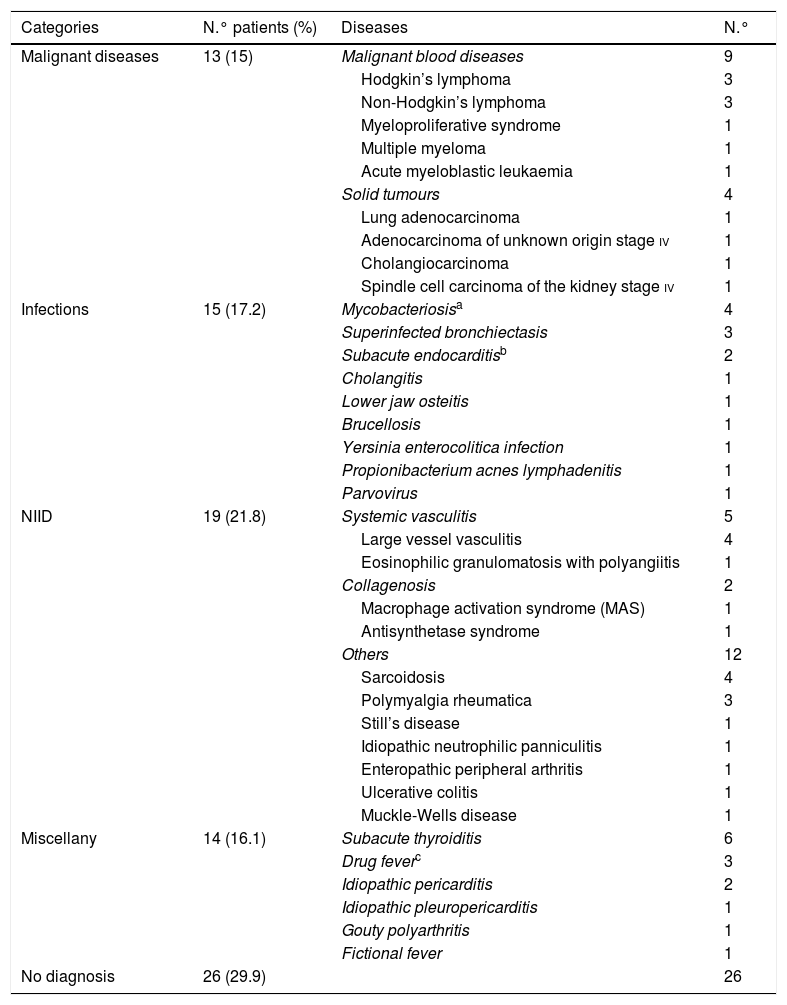
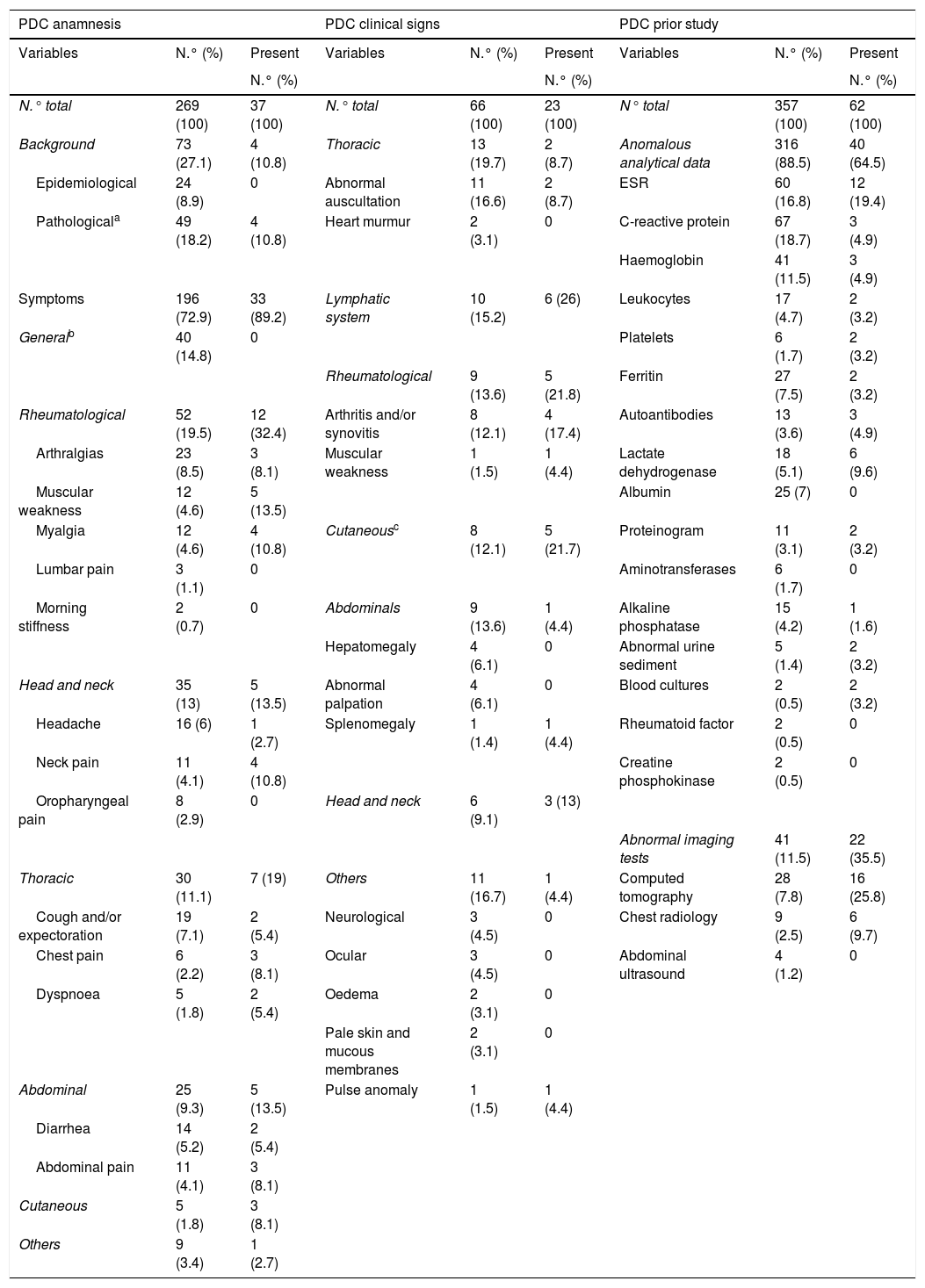
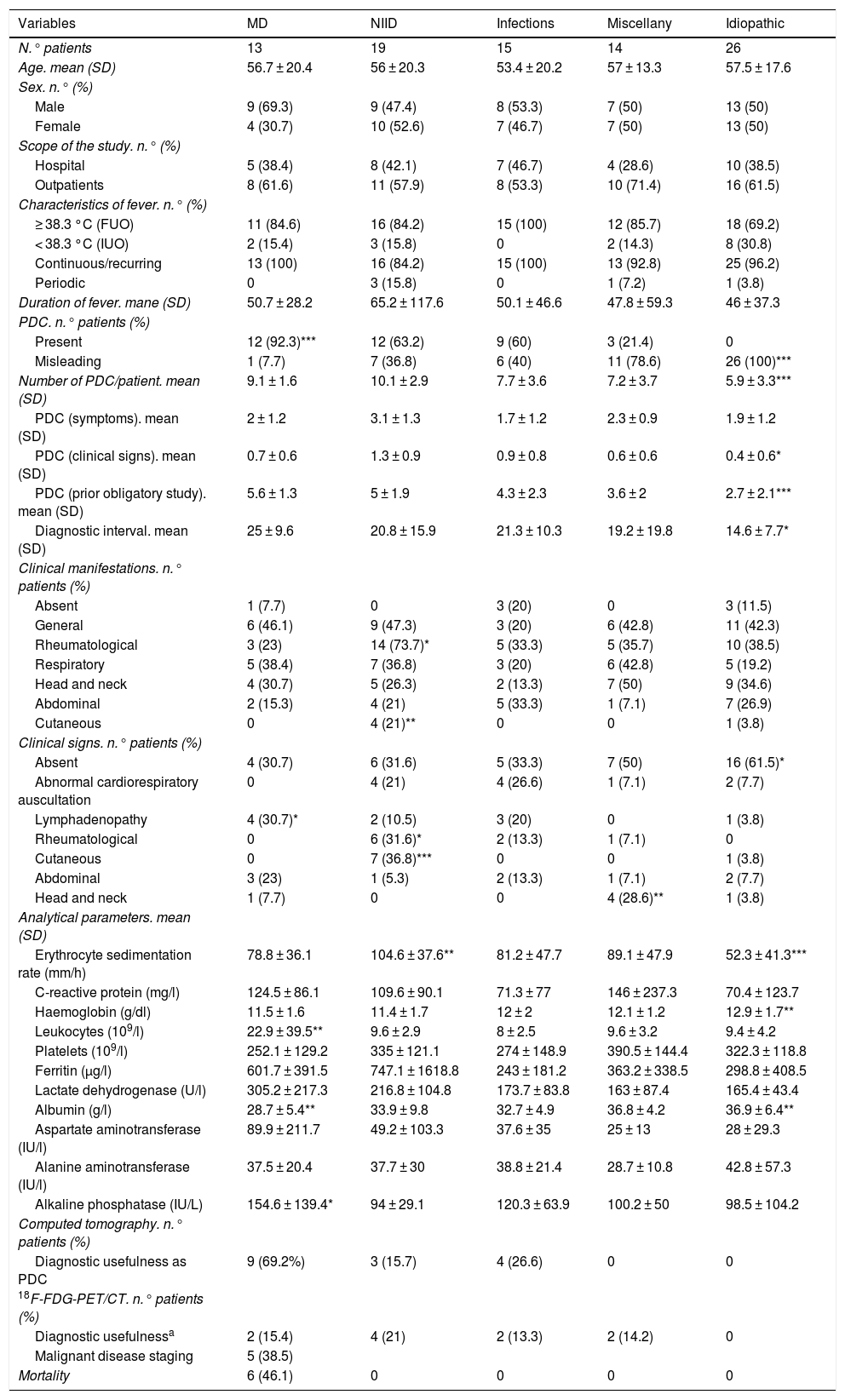
ResultsOf the 87 patients registered, 17.3% presented criteria of inflammation of unknown origin (IUO). The diagnoses were: non-infectious inflammatory diseases (NIID) in 19 patients (21.8%), infections in 15 (17.2%), miscellaneous in 14 (16.1%), malignant diseases in 13 (15%) and without diagnosis in 26 (29.9%). In 17.6% of the cases, a potentially diagnostic clue (PDC) was identified. The patients without diagnosis were characterized by a lower number of total PDC (5.9 ± 3.3 vs. 8.7 ± 3.4; P = .000), fewer clinical signs (.4 ± .6 vs. .9 ± .8; P = .001), a smaller number of tests in the previous study (2.7 ± 2.1 vs. 4.6 ± 2; P = .000), a shorter diagnostic interval (14.6 ± 7.7 days vs. 21.4 ± 9.5 days; P = .029) and less alteration of erythrocyte sedimentation rate (52.3 ± 41.3 mm/h vs. 89.8 ± 42.7 mm/h; P = .000), haemoglobin (12.9 ± 1.7 g/dl vs. 11.7 ± 1.6 g/dl; P = .003) and albumin (36.9 ± 6.4 g/l vs. 33.2 ± 7.2 g/l; P = .025). 18F-fluorodeoxyglucose positron-emission tomography combined with computed tomography (18F-FDG-PET/TC) proved to be helpful in 37% of the cases. Mortality was 6.8%.
ConclusionsThe definition of FUO with qualitative study criterion incorporates a diagnostic protocol that provides clear benefits in terms of cost-effectiveness.
Evaluar las características de la fiebre de origen desconocida (FOD) según la definición con criterio de estudio cualitativo y de los pacientes sin diagnóstico.
Material y métodosEstudio prospectivo observacional realizado entre 2009-2017 de todos los pacientes diagnosticados de FOD según la definición con criterio de estudio cualitativo ampliada. Se evaluaron variables demográficas, clínicas, diagnósticas y evolutivas.
ResultadosDe los 87 pacientes registrados el 17,3% presentaron criterios de inflamación de origen desconocido. Los diagnósticos fueron: enfermedades inflamatorias no infecciosas en 19 pacientes (21,8%), infecciones en 15 (17,2%), miscelánea en 14 (16,1%), enfermedades malignas en 13 (15%) y sin diagnóstico en 26 (29,9%). Se identificó algún indicio con potencial diagnóstico (IPD) en el 17,6% de los casos. Los pacientes sin diagnóstico se caracterizaron por un menor número de IPD totales (5,9 ± 3,3 vs. 8,7 ± 3,4; p = 0,000), menos signos clínicos (0,4 ± 0,6 vs. 0,9 ± 0,8; p = 0,011), menor número de pruebas en el estudio previo (2,7 ± 2,1 vs. 4,6 ± 2; p = 0,000), un menor intervalo diagnóstico (14,6 ± 7,7 días vs. 21,4 ± 9,5 días; p = 0,029) y una menor alteración de la velocidad de sedimentación globular (52,3 ± 41,3 mm/h vs. 89,8 ± 42,7 mm/h; p = 0,000), hemoglobina (12,9 ± 1,7 g/dl vs. 11,7±1,6 g/dl; p = 0,003) y albúmina (36,9 ± 6,4 g/l vs. 33,2 ± 7,2 g/l; p = 0,025). La tomografía por emisión de positrones con 18F-fluorodesoxiglucosa combinada con tomografía computarizada resultó de utilidad en el 37% de los casos. La mortalidad fue del 6,8%.
ConclusionesLa definición de FOD con criterio de estudio cualitativo incorpora un protocolo diagnóstico que aporta evidentes beneficios en términos de coste-eficacia.
