




In contrast to cancer or dementia, chronic obstructive pulmonary disease (COPD) progresses in a much more complex way. Some authors suggest that the extent of the needs of patients with advanced chronic diseases reaches beyond the purely clinical and disease management aspects and must include multidimensional questions in their evaluation (functional, social, psychological, and ethical points).1 Advanced disease, invalidating dyspnoea, and functional deficits limit the patients’ access to the outside world, like going out into the street and meet people, as they are not able to overcome the barriers of their homes (i.e. stairs, flats without a lift, etc.). The forced seclusion and social isolation inevitably form a handicap difficult to overcome. They restrict access to instrumental, leisure, and social life activities, which in turn lead to the occurrence of depressive states, anxiety or both.2
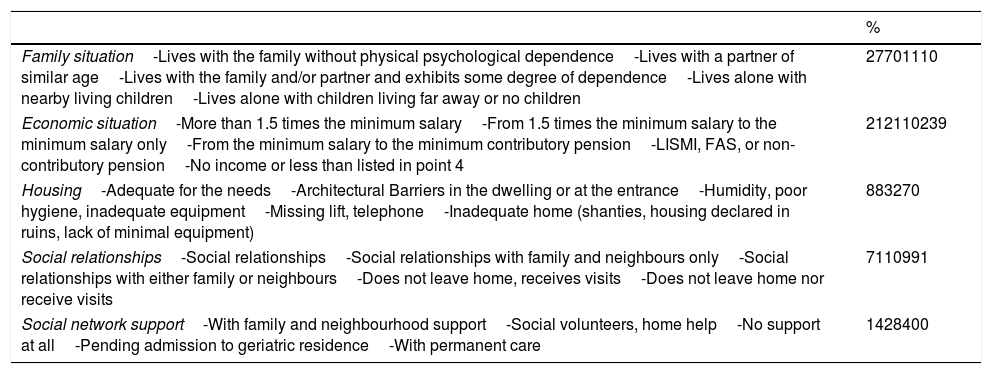
To evaluate the psychosocial situation in a cohort of patients with COPD, followed up at the Outpatient Clinics of Pneumology of the University Hospital Nuestra Señora de Candelaria (HUNSC), Santa Cruz de Tenerife, a descriptive observational study was conducted from January 2011 to December 2013. The Gijón as well as the Goldberg scale were applied. Out of a database of 308 COPD patients, 100 agreed to participate in the study. The patients’ mean age was 68±8.5. The majority (84%) were males; 18% were active smokers with a forced expiratory volume in the first second (FEV1) mean of the predicted 46%±18 and a mean BODE index of 4. A total of 84% of the patients stated not to have any support from their social network (Table 1), 42% had incomes below the inter-professional minimum salary, and 56% had some signs of depression.
Data obtained through the Gijón scale.
| % | |
|---|---|
| Family situation-Lives with the family without physical psychological dependence-Lives with a partner of similar age-Lives with the family and/or partner and exhibits some degree of dependence-Lives alone with nearby living children-Lives alone with children living far away or no children | 27701110 |
| Economic situation-More than 1.5 times the minimum salary-From 1.5 times the minimum salary to the minimum salary only-From the minimum salary to the minimum contributory pension-LISMI, FAS, or non-contributory pension-No income or less than listed in point 4 | 212110239 |
| Housing-Adequate for the needs-Architectural Barriers in the dwelling or at the entrance-Humidity, poor hygiene, inadequate equipment-Missing lift, telephone-Inadequate home (shanties, housing declared in ruins, lack of minimal equipment) | 883270 |
| Social relationships-Social relationships-Social relationships with family and neighbours only-Social relationships with either family or neighbours-Does not leave home, receives visits-Does not leave home nor receive visits | 7110991 |
| Social network support-With family and neighbourhood support-Social volunteers, home help-No support at all-Pending admission to geriatric residence-With permanent care | 1428400 |
LISMI: Law on the Social Integration of the Disabled; FAS: health assistance for illness/old age.
The perception of lack of social support has harmful effects on health and leads to an increase in depressive symptoms, a decrease in physical activity and quality of sleep, an increase in tobacco consumption, and also to reduced social interactions when spending a long time in solitude. These conditions augment morbidity and mortality to a similar extent as other known factors, such as smoking, obesity, or hypertension.3–5
COPD goes beyond a purely pulmonary dysfunction,6 and the lack of social support reported by our COPD patients must be taken into account, as it can significantly affect patient management. Improving the follow up and handling during the care process for this group includes an adequate health education on the disease itself as well as putting emphasis on a correct treatment adherence and self care and should also consider the need for a family approach.7
Informal caregivers (IC) provide technical and emotional support. We can find that patients supported by IC are less likely to smoke, seek emergency services less frequently, and adhere better to pharmacological treatment.8 Therefore, the role of IC is fundamental to a comprehensive framework of patient care and provides benefits to both the patient and the health system. However, we must take into account how the caregiver perceives the disease, as this could lead to a higher degree of dependence of the patient on their environment, so that health professionals should evaluate the role of the IC.8,9
In a situation of poverty, the possibilities of receiving support are limited, given that the members of this support network are in a similar situation of precariousness and vulnerability. Thus, help would need to be sought outside said setting, e.g., in the health sector. However, it must be taken into account that the services provided throughout the territory are heterogeneous.9 Professional awareness of this “other reality” and its approach from a perspective that comprehends the patients’ daily life situation are essential to meet sometimes hidden and not sufficiently expressed needs. Adapting to this reality is key to alleviate symptomatology and its functional and psychological repercussion, which would allow persons with COPD to better cope and manage their situation more effectively.

