




Drug-induced liver injury by antituberculous drugs (anti-TBC) is an idiosyncratic drug reaction, more often associated with isoniazid. Clinical manifestations may appear between 1 and 12 weeks after the onset of treatment, although they usually do between 2nd and 4th week.1,2
A severe form of drug toxicity is DRESS syndrome (Drug Reaction with Eosinophilia and Systemic Symtoms). It is characterized by fever, rash, eosinophilia and in many cases hepatotoxicity. This is a serious and potentially fatal reaction, with a mortality rate of around 20% if the responsible drug is not discontinuated, so early diagnosis is of utmost importance. Often it is not the skin involvement, but the presence of hepatotoxicity is a crucial factor in prognosis.2,3
A 69-year-old male presented to Emergency Room due to fever and rash. The physical examination showed jaundice and a cutaneous maculopapular rash with facial edema. Laboratory tests identified hyperbilirubinemia (total bilirubin 10.32mg/dl, conjugated bilirubin 9.72mg/dl), elevated transaminases (ALT 2095U/L, AST 1208U/L, GGT 364U/L and alkaline phosphatase 566U/L), leukocytosis with eosinophilia (WBC of 13,800/μL with 17.6% eosinophils) and coagulopathy (INR 2.31. Abdominal ultrasound showed no relevant findings.
The patient had recently been diagnosed with tuberculosis so he had started first-line anti-TBC treatment with rifampicin, isoniazid, ethambutol and pyrazinamide five weeks before the onset of the clinical picture. The search for the following alternative causes was negative: viral infections (HAV, HBV, HCV, HEV, EBV, CMV), alcohol-related liver disease, autoantibody titers, serum IgG, ceruloplasmin levels and 24 urine cooper. Liver biopsy was considered, but finally it was not done because the condition presented with typical manifestations, alternative causes were ruled out and the patient evolved favorably.
Due to the temporal relationship between drug therapy and the appearance of the clinical picture and the exclusion of other causes of liver disease, the diagnosis of DRESS syndrome with acute drug-induced liver injury (DILI) with hepatocellular pattern was established. It was decided to stop treatment and prednisolone was prescribed in descending pattern.
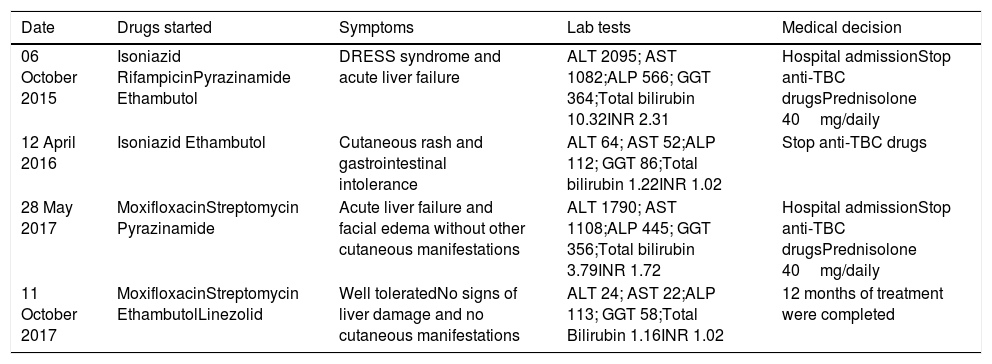
The outcome was favorable with 8 weeks of treatment normalizing liver function and transaminases levels. However, upon restarting a 2nd and 3rd line of anti-TBC treatment, our patient presented two successive episodes the second episode presented cutaneous manifestations with mild asymptomatic liver enzyme elevation and in the third episode he suffered facial edema and acute DILI with hepatocellular pattern requiring new hospital admission and systemic steroids treatment (Table 1).
Timeline of anti-TB treatments and events.
| Date | Drugs started | Symptoms | Lab tests | Medical decision |
|---|---|---|---|---|
| 06 October 2015 | Isoniazid RifampicinPyrazinamide Ethambutol | DRESS syndrome and acute liver failure | ALT 2095; AST 1082;ALP 566; GGT 364;Total bilirubin 10.32INR 2.31 | Hospital admissionStop anti-TBC drugsPrednisolone 40mg/daily |
| 12 April 2016 | Isoniazid Ethambutol | Cutaneous rash and gastrointestinal intolerance | ALT 64; AST 52;ALP 112; GGT 86;Total bilirubin 1.22INR 1.02 | Stop anti-TBC drugs |
| 28 May 2017 | MoxifloxacinStreptomycin Pyrazinamide | Acute liver failure and facial edema without other cutaneous manifestations | ALT 1790; AST 1108;ALP 445; GGT 356;Total bilirubin 3.79INR 1.72 | Hospital admissionStop anti-TBC drugsPrednisolone 40mg/daily |
| 11 October 2017 | MoxifloxacinStreptomycin EthambutolLinezolid | Well toleratedNo signs of liver damage and no cutaneous manifestations | ALT 24; AST 22;ALP 113; GGT 58;Total Bilirubin 1.16INR 1.02 | 12 months of treatment were completed |
During the follow-up period, the tuberculous disease worsened; with pulmonary, pleural, lymph node and peritoneal progression and the appearance of a chest wall abscess. Therefore, it was decided to immediately restart a new 4th-line anti-TB therapy, avoiding the potentially hepatotoxic drugs. Such therapy was based on streptomycin, moxifloxacin, ethambutol and linezolid. Surgical drainage of the chest wall abscess was also performed. The patient completed 12 months of anti-TB treatment, achieving complete clinical and bacteriological cure of tuberculosis disease, without signs of liver damage during this period.
Several cases of Drug-induced liver injury and DRESS syndrome induced by anti-TBC drugs have been reported in the literature. The main associated drugs are the first-line anti-TBC drugs; isoniazid, rifampin and pyrazinamide, especially when used in association as in the case we present.1,2,4 For the diagnosis of drug-induced liver injury and/or DRESS syndrome, clinical suspicion is very important, together with a comprehensive anamnesis of drug use, which will allow us to consider the temporal relations between drug intake and the development of the clinical picture The exclusion of alternative causes of liver damage is of utmost importance.1,4
In the case we report, due to the successive changes of anti-TBC treatment, it is not possible to define with certainty which drugs are responsible for the liver damage episodes. Rechallenge tests were not performed due to safety and ethical reasons. Based on the timeline of the events and on a revision of the scientific literature,2,4 we consider isoniazid, rifampicin and pyrazinamide as the responsible drugs. We did not consider the other used drugs directly responsible (ethambutol, moxifloxacin, streptomycin, linezolid), although we cannot rule out certain hepatotoxic role of these when used in combination with any of the three previously mentioned.
Early recognition and withdrawal of the medication must be done immediately once the etiology is suspected. Deliberate rechallenge with the causative drug is not advocated, unless the clinical scenario demands such an exposure. Controlled rechallenge after an episode of liver injury is, however, considered justified in relation to oncology and anti-TBC therapy. Therefore, the restart of treatment will usually be done once symptoms are resolved and liver function and transaminases levels have normalized.1,4
In the context of tuberculosis failure to receive specific treatment entails a high risk of disease progression, as well as a risk of transmission.5 For this reason, in patients with toxic reactions to anti-TBC treatment the choice of a line of alternative treatment that avoids delay of therapy is very complex but of vital importance to prevent the progression of the disease, with a possible fatal outcome.
This work has not had specific financing mechanisms. Finally, Irabien M. wants to thank, the invaluable support received from Blanco S.

