



To analyze the quality of care provided during the COVID-19 pandemic, identifying what care has been prioritized and factors that have influenced such care.
BackgroundGiven the need to adapt care due to the pandemic, nurses may have been subjected to factors that have negatively affected them, however it has also been possible to find actions that have enabled nurses to maintain the quality of care provided.
MethodExploratory study with a sample of 225 nurses. Data collection was performed using a self-assessment of the care provided, the ‘Care Left Undone’ Scale, and ad hoc questionnaire for demographic variables.
ResultsThe mean rate of missed care was 5.76. Significant differences were identified according to age, professional experience, field of specialty and personal and professional strategies.
ConclusionBoth personal and professional feelings, characteristics, and strategies have an effect in the perception of quality of care provided and missed care during the pandemic.
Analizar la calidad de los cuidados brindados durante la Pandemia por Covid-19, identificando que cuidados se han priorizado y los factores que han influido. Ante la situación de adaptación de los cuidados exigidos por la Pandemia, las enfermeras han podido estar sometidas a factores que hayan afectado de manera negativa, pero también se han podido encontrar estrategias que hayan permitido mantener la calidad de los cuidados.
MétodoEstudio descriptivo con muestra de conveniencia de 225 enfermeras que atendieron a pacientes con COVID_19. Para la recogida de datos se emplea un cuestionario ad hoc de variables personales y laborales, una autovaloración de los cuidados y la escala Care Left Undone.
ResultadosLa tasa media de cuidados perdidos ha sido de 5,76 (DS 3,1). Se identifican diferencias significativas en función de la edad, experiencia profesional y del cambio de estructura y de especialidad. Las estrategias que se asocian de manera significativa con mayor valoración de la calidad de los cuidados estuvieron relacionadas con la cohesión del equipo, evitar la despersonalización, búsqueda activa de información, estrategias de control de estrés y de pensamiento positivo. Se han identificados sentimientos, características y estrategias personales y profesionales, que influyen tanto en la percepción de la calidad como en la pérdida de cuidados durante la atención a la pandemia.
In view of the care adaptation situation required by the pandemic, nurses have been subjected to personal, professional and employment factors which have impeded their care ability.
What does this paper contribute?Our study identifies personal, professional and emotional characteristics which have acted as facilitators in maintaining quality of care.
Care is the cornerstone of all health systems and there is a large body of evidence demonstrating that people's health outcomes are highly dependent on the nursing care they receive.1,2 This association is evidenced by a systematic review of 102 studies which concluded that increased levels of registered nursing care were associated with lower rates of hospital mortality and fewer adverse events.3 In addition, nursing care ensures that the person is at the centre of care, upholding the dignity of the cared-for person, through a relationship of communication, respect and collaboration.4,5 The COVID-19 pandemic has further highlighted the importance of nursing.
Several reports from official agencies have denounced the apparent shortage of nurses during the pandemic as a consequence of years of austerity and cuts in recruitment. To cope with this high demand, following the measures established by the Royal Decree of the State of Emergency,6 structural and working conditions were modified, and many nurses had to work in specialties other than their own, with mechanisms of physical and social isolation that affected the care relationship and which, in addition, often led to a prioritisation of care as a response to the high care needs that were occurring.7 This prioritisation may have resulted in the loss of essential care. Missed nursing care is defined as “any aspect of care required by the patient that is omitted or significantly delayed”,8 and is classified within the error of omission and was conceptualised as “missed nursing care” (MNC)9–11 and as “care left undone”.12 Factors that according to the literature can lead to loss of nursing care are related to lack of available labour resources; lack of accessible material resources and various relationship and communication factors that impact on the nurses' ability to provide care, such as teamwork and communication between team members or the user/family.1,2,13,14
The pandemic situation contains all the risk factors for a situation of loss of nursing care and adds a new factor derived from the situation, which is the personal psychological stress of the professional, arising from response to such an extraordinary global event.7,15,16 But we also find in the literature that there may be factors that act to maintain the quality of care, as they describe the personal and professional characteristics of nurses, the organisational climate and job support received, which are identified as significant predictors of quality of care.17–19 Therefore, in the face of the situation of adapting the care demanded by the pandemic, nurses may have been subjected to factors that have negatively affected the care provided, but it has also been possible to develop behaviours of positive adaptation to the adversity of the situation and to find actions that have allowed them to maintain the quality of nursing care within this difficult context.
The aim of the study was to analyse the quality of care provided during the COVID-19 pandemic, identifying care that was prioritised and exploring personal, professional, emotional or work environment factors and characteristics that may have influenced care.
MethodStudy designRetrospective descriptive and cross-sectional study, which evaluated the self-perceived quality of care provided by the nurses and analysed the care they have stopped providing.
Population and scope of studyThe reference population was the nurses of the Hospital Universitario Parc Tauli of Sabadell (809 nurses). It is a level III hospital, with 780 beds, which at the peak of the pandemic on 31/03 and 1/04 had 632 patients admitted with a diagnosis of COVID-19. A convenience sample of 225 nurses was determined with the inclusion criterion of having worked directly in the care of COVID-19 patients. To avoid losses, the survey was sent to 240 nurses, of whom 225 completed the questionnaire.
VariablesA survey containing 58 questions was designed, which measured the study variables and were grouped into the following sections:
Self-perceived assessment of the care provided and their degree of autonomy, using a visual analogue scale ranging from 0 to 10.
Care Left Undone Scale: This is a consensus-based instrument for prioritising care from which two measures of "care left undone" are derived. First, the prevalence of any care left undone (binary measure). Second, a score indicating the amount of care left undone, by summing the number of activities ticked per person.2,8,12
Ad hoc questionnaire which collected data on sociodemographics, employment, skills and personal preoccupation from COVID-19.
List identifying feelings that nurses have had while caring during the pandemic, assessing their prevalence by the degree of agreement with the statements on a Likert scale from 1 to 10. List based on the study by Bao et al.15
List of personal and professional strategies adopted to promote care. List based on the studies by Bao et al.;15 Petzold et al.16 and Wu et al.19
Data collectionData collection was carried out in May 2020 and nurses were asked to assess the care provided during the period of peak incidence, which in our setting was between 27th March and 8th April. The survey was sent via an email hyperlink. The link included information about the study, informed consent and the questionnaire. Participants then signed the consent form and sent the completed questionnaire via the platform.
Data analysisDescription, professional profile of nurses, assessment of care, emotions and strategies developed were performed using summary statistics (mean, SD, median, interquartile range [IQR], frequencies and percentages). Descriptive statistics were used to describe the prevalence and nature of the care that was missed. Groups with high valuation of care provided (≥ 7) were compared to the low valuation group (< 7), in relation to loss of care, emotions felt, barriers identified, and professional and personal strategies used. Significance analyses were performed using Spearman's correlation test and the Mann–Whitney U test, due to the non-normal distribution of scores, and comparisons of medians between more than two groups were performed using the non-parametric Kruskal–Wallis test. Comparison of percentages of missed care was performed with the Chi-square test. All the above analyses were performed with SPSS V.20 (IBM Corp., Armonk, NY).
Ethical considerationsThe study was approved by the Clinical Research Ethics Committee of the Hospital Universitari Parc Taulí of Sabadell in April 2020. Ref.2020623. Participants received information on all aspects related to the study, the voluntary nature of the study and date privacy and confidentiality.
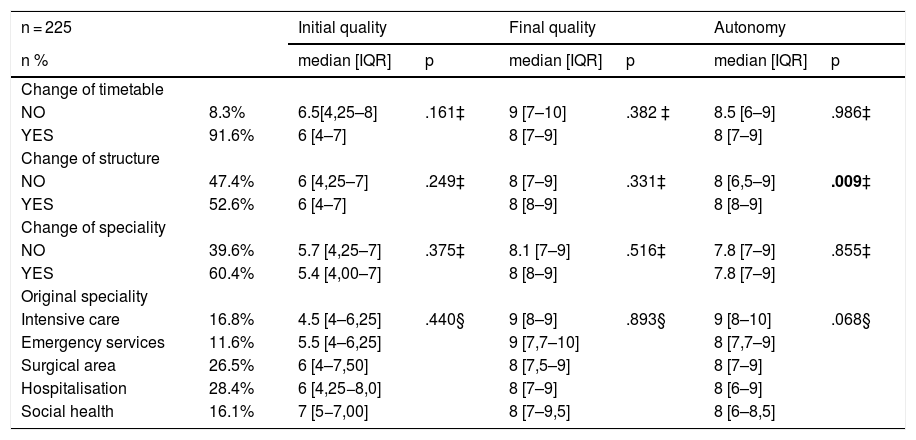
ResultsDescription of the sample and evaluation of care providedTwo hundred and twenty five nurses participated in the study, with a median age of 43.0 years (IQR: 15) and a median professional experience of 17.0 years (IQR: 12). The quality rating increased from an initial median score of 6 (IQR = 4−7) to a quality of care rating of 8.1 (IQR = 7–9) at the end of April. The increase in quality rating over the weeks was a statistically significant increase (p < .05). The perceived degree of autonomy of the nurses in carrying out this care scored 8 (IQR = 7–9) out of 10. And the mean rate of missed care was 5.7 (SD = 3.1).
Analysis of the contrast between the assessment of care and the secondary variables showed a significant association between the assessment of the quality of the initial care provided, both for age (p = .021) and for years of professional experience (p = .047). We also found that professionals who had changed physical environment had a higher degree of perceived autonomy than professionals who had not changed (p = .009). The change of timetable, the area of origin and even having to provide care other than one's own did not produce significant changes either in the assessment of the care provided or in the degree of autonomy of the care (Table 1).
Evaluation of perceived care quality and professional variables (n = 225).
| n = 225 | Initial quality | Final quality | Autonomy | ||||
|---|---|---|---|---|---|---|---|
| n % | median [IQR] | p | median [IQR] | p | median [IQR] | p | |
| Change of timetable | |||||||
| NO | 8.3% | 6.5[4,25–8] | .161‡ | 9 [7–10] | .382 ‡ | 8.5 [6–9] | .986‡ |
| YES | 91.6% | 6 [4–7] | 8 [7–9] | 8 [7–9] | |||
| Change of structure | |||||||
| NO | 47.4% | 6 [4,25–7] | .249‡ | 8 [7–9] | .331‡ | 8 [6,5–9] | .009‡ |
| YES | 52.6% | 6 [4–7] | 8 [8–9] | 8 [8–9] | |||
| Change of speciality | |||||||
| NO | 39.6% | 5.7 [4,25–7] | .375‡ | 8.1 [7–9] | .516‡ | 7.8 [7–9] | .855‡ |
| YES | 60.4% | 5.4 [4,00–7] | 8 [8–9] | 7.8 [7–9] | |||
| Original speciality | |||||||
| Intensive care | 16.8% | 4.5 [4–6,25] | .440§ | 9 [8–9] | .893§ | 9 [8–10] | .068§ |
| Emergency services | 11.6% | 5.5 [4–6,25] | 9 [7,7–10] | 8 [7,7–9] | |||
| Surgical area | 26.5% | 6 [4–7,50] | 8 [7,5–9] | 8 [7–9] | |||
| Hospitalisation | 28.4% | 6 [4,25−8,0] | 8 [7–9] | 8 [6–9] | |||
| Social health | 16.1% | 7 [5−7,00] | 8 [7–9,5] | 8 [6–8,5] | |||
†Pearson ‡ Mann Whitney § Kruskal Wallis. IQR: interquartile range.
Note: statistical significance indicated in bold.
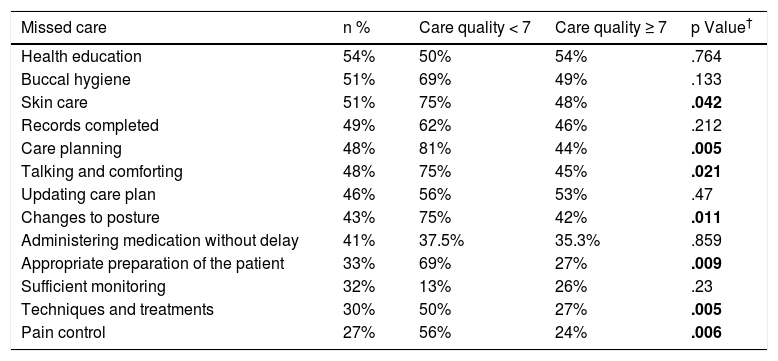
The activities most frequently identified as missed are presented in Table 2. The comparison of missed care in terms of self-assessed quality of care is also presented in Table 2.
Prevalence of missed care and relationship with self-assessment of care quality provided (n = 225).
| Missed care | n % | Care quality < 7 | Care quality ≥ 7 | p Value† |
|---|---|---|---|---|
| Health education | 54% | 50% | 54% | .764 |
| Buccal hygiene | 51% | 69% | 49% | .133 |
| Skin care | 51% | 75% | 48% | .042 |
| Records completed | 49% | 62% | 46% | .212 |
| Care planning | 48% | 81% | 44% | .005 |
| Talking and comforting | 48% | 75% | 45% | .021 |
| Updating care plan | 46% | 56% | 53% | .47 |
| Changes to posture | 43% | 75% | 42% | .011 |
| Administering medication without delay | 41% | 37.5% | 35.3% | .859 |
| Appropriate preparation of the patient | 33% | 69% | 27% | .009 |
| Sufficient monitoring | 32% | 13% | 26% | .23 |
| Techniques and treatments | 30% | 50% | 27% | .005 |
| Pain control | 27% | 56% | 24% | .006 |
†Chi square.
Note: statistical significance indicated in bold.
The volume of unperformed care is obtained from the sum of the number of marked activities per person. This calculation gives a mean volume for our study population of 5.4 (SD = 3.5). In inferential analysis, significant differences are identified as a function of change of structure (p = .002), change of care activities (p = .005), age (p = .002) and work experience (p = .003). There is also a significant relationship between the assessment of final care and the degree of autonomy with the rate of lost care (p = .010)/(p = .021).
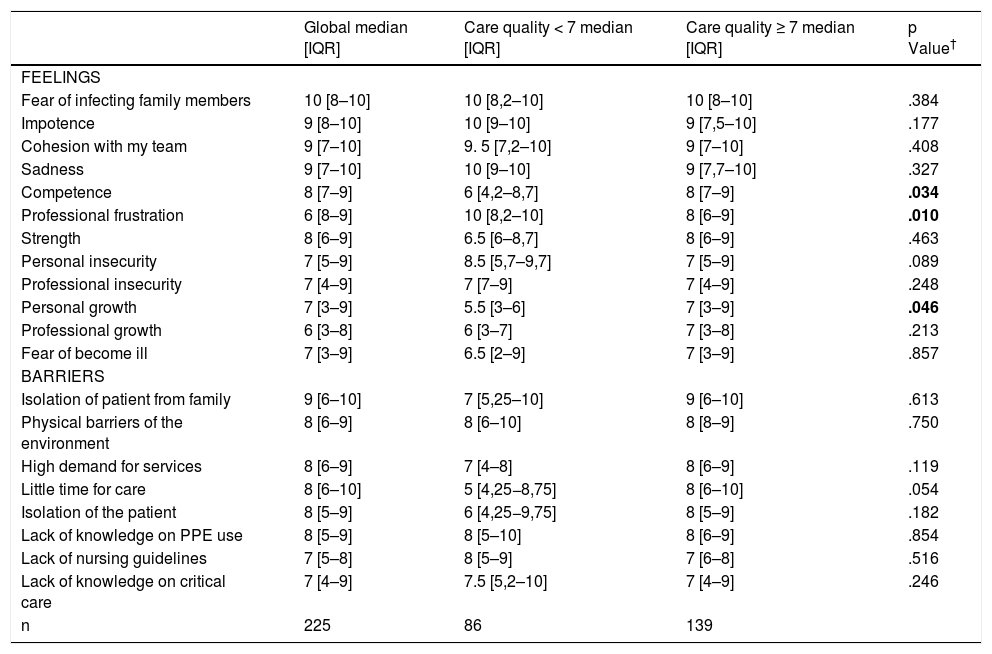
Feelings and barriers identified during the provision of careThe analysis of the emotions experienced by the nurses while performing this care and the barriers identified is presented in Table 3. The comparative analysis, according to the degree of quality of care, shows significant differences in the feelings of competence and personal growth. These are more prevalent in the nurses with a high evaluation of the care, whilst in the group with a lower evaluation, feeling of frustration is more prevalent (Table 4).
Comparison between feelings and barriers detected in care according to the self-assessment of care provided.
| Global median [IQR] | Care quality < 7 median [IQR] | Care quality ≥ 7 median [IQR] | p Value† | |
|---|---|---|---|---|
| FEELINGS | ||||
| Fear of infecting family members | 10 [8–10] | 10 [8,2–10] | 10 [8–10] | .384 |
| Impotence | 9 [8–10] | 10 [9–10] | 9 [7,5–10] | .177 |
| Cohesion with my team | 9 [7–10] | 9. 5 [7,2–10] | 9 [7–10] | .408 |
| Sadness | 9 [7–10] | 10 [9–10] | 9 [7,7–10] | .327 |
| Competence | 8 [7–9] | 6 [4,2–8,7] | 8 [7–9] | .034 |
| Professional frustration | 6 [8–9] | 10 [8,2–10] | 8 [6–9] | .010 |
| Strength | 8 [6–9] | 6.5 [6–8,7] | 8 [6–9] | .463 |
| Personal insecurity | 7 [5–9] | 8.5 [5,7–9,7] | 7 [5–9] | .089 |
| Professional insecurity | 7 [4–9] | 7 [7–9] | 7 [4–9] | .248 |
| Personal growth | 7 [3–9] | 5.5 [3–6] | 7 [3–9] | .046 |
| Professional growth | 6 [3–8] | 6 [3–7] | 7 [3–8] | .213 |
| Fear of become ill | 7 [3–9] | 6.5 [2–9] | 7 [3–9] | .857 |
| BARRIERS | ||||
| Isolation of patient from family | 9 [6–10] | 7 [5,25–10] | 9 [6–10] | .613 |
| Physical barriers of the environment | 8 [6–9] | 8 [6–10] | 8 [8–9] | .750 |
| High demand for services | 8 [6–9] | 7 [4–8] | 8 [6–9] | .119 |
| Little time for care | 8 [6–10] | 5 [4,25−8,75] | 8 [6–10] | .054 |
| Isolation of the patient | 8 [5–9] | 6 [4,25−9,75] | 8 [5–9] | .182 |
| Lack of knowledge on PPE use | 8 [5–9] | 8 [5–10] | 8 [6–9] | .854 |
| Lack of nursing guidelines | 7 [5–8] | 8 [5–9] | 7 [6–8] | .516 |
| Lack of knowledge on critical care | 7 [4–9] | 7.5 [5,2–10] | 7 [4–9] | .246 |
| n | 225 | 86 | 139 | |
†Mann Whitney. IQR: interquartile range.
Note: statistical significance indicated in bold.
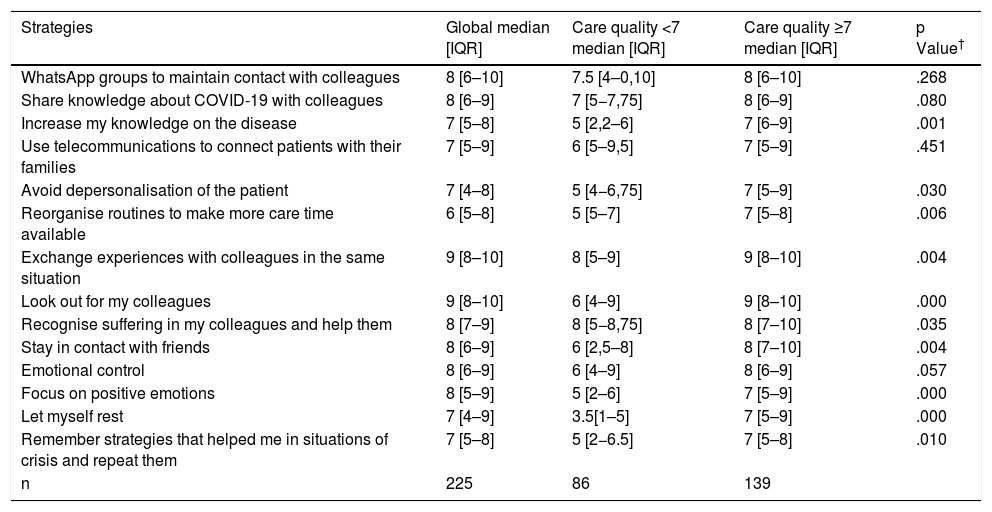
Analysis of strategies developed and self-assessment of care quality provided.
| Strategies | Global median [IQR] | Care quality <7 median [IQR] | Care quality ≥7 median [IQR] | p Value† |
|---|---|---|---|---|
| WhatsApp groups to maintain contact with colleagues | 8 [6–10] | 7.5 [4–0,10] | 8 [6–10] | .268 |
| Share knowledge about COVID-19 with colleagues | 8 [6–9] | 7 [5−7,75] | 8 [6–9] | .080 |
| Increase my knowledge on the disease | 7 [5–8] | 5 [2,2–6] | 7 [6–9] | .001 |
| Use telecommunications to connect patients with their families | 7 [5–9] | 6 [5–9,5] | 7 [5–9] | .451 |
| Avoid depersonalisation of the patient | 7 [4–8] | 5 [4−6,75] | 7 [5–9] | .030 |
| Reorganise routines to make more care time available | 6 [5–8] | 5 [5–7] | 7 [5–8] | .006 |
| Exchange experiences with colleagues in the same situation | 9 [8–10] | 8 [5–9] | 9 [8–10] | .004 |
| Look out for my colleagues | 9 [8–10] | 6 [4–9] | 9 [8–10] | .000 |
| Recognise suffering in my colleagues and help them | 8 [7–9] | 8 [5−8,75] | 8 [7–10] | .035 |
| Stay in contact with friends | 8 [6–9] | 6 [2,5–8] | 8 [7–10] | .004 |
| Emotional control | 8 [6–9] | 6 [4–9] | 8 [6–9] | .057 |
| Focus on positive emotions | 8 [5–9] | 5 [2–6] | 7 [5–9] | .000 |
| Let myself rest | 7 [4–9] | 3.5[1–5] | 7 [5–9] | .000 |
| Remember strategies that helped me in situations of crisis and repeat them | 7 [5–8] | 5 [2−6.5] | 7 [5–8] | .010 |
| n | 225 | 86 | 139 |
The highest scoring personal and professional strategies are listed in Table 4. We found there were significant differences in the strategies developed, depending on the evaluation of care quality, also contained in Table 4.
DiscussionIn our study we noted good self-perception of care quality provided during the pandemic as evidenced by the results of the care left undone scale with a score of 5.4. When comparing this result with the study by Ball et al.,12 we found there was concordance, since care scores classed as good correlated with a range of care left undone of between 4.02 and 5.44. Physical and organisational conditions of work were identified in the references as causal factors of care left undone. 12–14,20,21
In our study we also identified this relationship within the context of pandemic care, since we found that the care left undone was greater in cases where nurses had to change their physical structure and working area.
With regard to essential care that was left undone, similarly to that shown in the studies by Ball et al.,14 Griffiths et al.21 and Juvé-Udina et al.,22 care relating to the most acute physical needs (pain, surveillance and medication) were prioritised, whilst psychosocial activities which were considered bureaucratic and which required a large amount of time, received lower priority. When comparing the percentage of the most prevalent care left undone with the study by Ball et al.,12 we observed similar percentages in our sample of the most left undone care: health education 54% vs. Ball et al., 52%, recording and planning care 48% vs. Ball et al., 47%, and talking and comforting 48% vs. Ball et al., 66%. In contrast, in the least left undone care, in our sample rates were higher: pain control 27% vs. Ball et al., 7%, and applying care and techniques 30% vs. Ball et al., 11%. This discrepancy may be due to the high prevalence of factors identified as barriers and which also coincide with factors identified in the references as the most common causes of care omission: inappropriate ratios; work overload, and time required for nursing intervention.23,24
In the context of the COVID-19 pandemic, all three factors are identified in our study as barriers to care: the overburden of having to work in isolation, high demand for care, the physical barriers of rehabilitated environments that make it difficult to work.
Regarding personal characteristics, missed care and reduction of care quality, as with other studies,20,24–26 we observed a significant impact relating to age, experience and speciality. Coinciding with Subirana et al.27 we found that the clinical experience was related to high quality of care and better levels of monitoring. Finally, we found, as in the study by Du et al.,20 that there was an association between better outcomes in care and psychosocial factories such as social support, positive attitudes and group cohesion.
In the analysis of professional strategies developed, the most highly appraised were group cohesion and the exchange of and search for knowledge. Of note was the significant association between high scores on care with professional strategies which seek to prevent depersonalisation and to maintain communication with the families, since they are presented as the solution to one of the main barriers identified – physical and family user isolation. This active search for solutions coincides with the concept of personal responsibility which Drach-Zahavy et al.17 identified in their study as a protective factor against missed care.
Finally, with regard to the personal strategies used by nurses, our study coincided with that of Salvarani et al.,28 who found an association between nurses with a higher ability to control their emotions and greater empathy and the fact they suffered from less distress. In our study we found that the nurse who gave high scores to care provided stated they had more frequently used personal emotional control strategies, positive thinking, and concern for the well-being of their colleagues.
We may conclude that the nurses of our study reflected that, despite the difficulties identified in the study as barriers and the high prevalence of feelings such as fear of infecting their families or impotence, they were able to maintain care quality by developing personal and professional strategies which helped them not just to maintain but also to increase care quality. Being aware of the factors which had an impact on care during the COVID-19 pandemic may help managers and planners of nursing services, when faced with higher care demands, to organise the teams in such a way as to ease missed care, by designing support strategies, preventing stated barriers and promoting professional and personal strategies that have been identified as protective for maintaining care quality.
FinancingAll persons listed as authors participated sufficiently in this study to accept public responsibility for the manuscript content. This article did not receive any funding from public or private entities.
Conflict of interestsThe authors have no conflict of interests to declare.
Our very special thanks to the nurses who participated in the study. We highly appreciate their commitment and professionalism, and the great work they did taking care of patients in the difficult context of the COVID-19 pandemic.
Please cite this article as: Obregón-Gutiérrez N, Puig-Calsina S, Bonfill-Abella A, Forrellat-González L, Subirana-Casacuberta M. «Cuidados perdidos» y calidad de los cuidados durante la pandemia por COVID-19: factores y estrategias influyentes. Enferm Clín. 2022;32:4–11.
