




Children with pneumonia need a correct position to increase their oxygen saturation and comfort level. Postural changes affect the function of the human body and disease conditions. This study aimed to identify the effect of prone and semirecumbent positions on the oxygen saturation and comfort level of children under five with pneumonia.
MethodThe study design was a quasi-experimental with a pre-posttest control group design. Thirty-six children with pneumonia aged 0-59 months were selected using consecutive sampling and divided into three groups: prone (n = 12), semirecumbent (n = 12), and control (n = 12). Statistical analysis was conducted using the Wilcoxon test, paired t test, and Kruskal-Wallis test.
ResultsA significant difference in the oxygen saturation level was found among the three groups, particularly in the semirecumbent group. No significant difference was observed on the comfort level in all groups.
ConclusionsThe semirecumbent position can be applied to improve the oxygenation status of children under five with pneumonia. Therefore, nurses should teach the family how to position the children with pneumonia during their hospitalization.
Pneumonia is the cause of 15% of deaths of children under five around the world, with 2% of these children being infants. In 2013, about 935,000 children under five were estimated to have died of pneumonia; that is, more than 2,500 children died from the disease every day1. Indonesia is one of the top 15 countries with the highest number of toddler mortality rate caused by pneumonia at 22,000 deaths in 20132,3.
Children with pneumonia undergo oxygenation problems and need oxygen therapy if the oxygen saturation level (SpO2) is less than 90%4. One of the nursing interventions for children with oxygenation problems is positioning. Positioning is considered to affect the human body and various disease conditions in terms of the expansion of the lungs and the effects of gravity affecting the human body5.
The types of positioning that can be administered to patients with oxygenation problems are prone and semi-up-right. The prone position is considered to have a rapid effect in increasing the oxygenation level in the blood of patients with acute respiratory distress syndrome (ARDS) and reduces the mortality rate of patients with ARDS6. Conversely, the 45° semi-upright position, which is generally known as the semirecumbent position, is considered to have a rapid effect in increasing oxygenation in blood7. Moreover, the semirecumbent position adjustment can increase oxygenation and gas exchange in patients with mechanical ventilation8.
As children with pneumonia have oxygenation problems, an appropriate position to increase oxygenation and comfort is necessary9. The semirecumbent position may reduce coughing and the use of sedative medicines, and increase the patient's comfort unlike the supination position during the administration of bronchoscopy procedures10. As positioning of children with pneumonia has yet to become a focus of nursing, research needs to be conducted on the effect of prone and semirecumbent positioning on the oxygen saturation and comfort level of children under five with pneumonia.
MethodThis research used a quasi-experimental design with a pre-posttest with a control group design. The intervention group was divided into two groups, namely, prone and semirecumbent. The control group conducted positioning according to the routine hospital procedure.
Sampling was conducted through consecutive sampling with the criterion of children under five, that is, aged 0-59 months, who were treated at the hospital where positioning was administered to children with pneumonia without any contraindication. Each group consisted of 12 children; thus, 36 children participated in the research. Oxygen saturation measurement was conducted using pulse oximetry, and comfort level was measured using the FLACC observation sheet. Oxygen saturation measurement and comfort level observation were performed twice: before treatment (pretest) and 60 min after treatment (posttest). The prone group was placed on the prone position, with the head facing one side; the semirecumbent group was placed on a half sitting position at a 45° angle; and the control group was positioned in accordance with the hospital routine. Ethical approval was issued by the Research Ethics Committee of the Faculty of Nursing, Universitas Indonesia. The analysis was conducted using the Wilcoxon test and the paired t test. The Kruskal-Wallis test was used to compare the groups.
ResultsThe characteristic features of the respondents are as follows: less than 12 months old (age range of 1-31 months), male, mother's education level is primary school level, good nutritional status, breastfed, fully immunized according to their age, and living environment is under the unhealthy category.
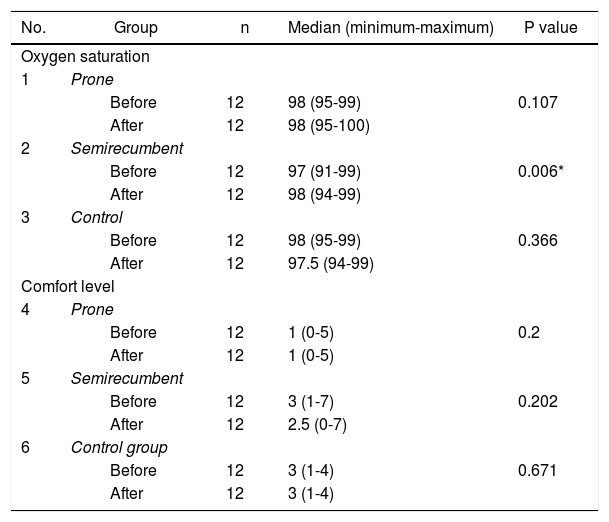
Table 1 shows that the median value of oxygen saturation increases 60 min after semirecumbent positioning is administered and that of comfort level decreases 60 min after semirecumbent positioning is administered. The median values of the prone group and the control group remain unchanged. The lower the score is, the higher the comfort level of children under five. The result of the statistical test using the Wilcoxon test indicates no significant difference in the prone position adjustment in the comfort level of children under five with pneumonia in the prone, semirecumbent, and control groups.
Analysis of the differences in oxygen saturation and level of comfort of the prone, semirecumbent, and control group adjustment positions (n=36).
| No. | Group | n | Median (minimum-maximum) | P value |
|---|---|---|---|---|
| Oxygen saturation | ||||
| 1 | Prone | |||
| Before | 12 | 98 (95-99) | 0.107 | |
| After | 12 | 98 (95-100) | ||
| 2 | Semirecumbent | |||
| Before | 12 | 97 (91-99) | 0.006* | |
| After | 12 | 98 (94-99) | ||
| 3 | Control | |||
| Before | 12 | 98 (95-99) | 0.366 | |
| After | 12 | 97.5 (94-99) | ||
| Comfort level | ||||
| 4 | Prone | |||
| Before | 12 | 1 (0-5) | 0.2 | |
| After | 12 | 1 (0-5) | ||
| 5 | Semirecumbent | |||
| Before | 12 | 3 (1-7) | 0.202 | |
| After | 12 | 2.5 (0-7) | ||
| 6 | Control group | |||
| Before | 12 | 3 (1-4) | 0.671 | |
| After | 12 | 3 (1-4) | ||
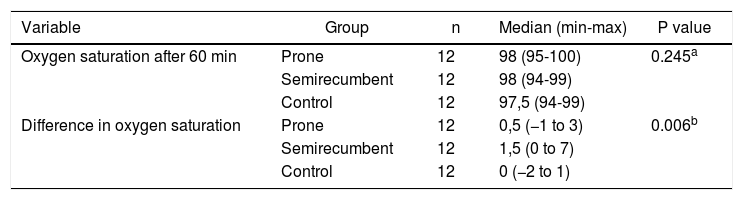
As presented in Table 2, the result of the statistical test using the Kruskal-Wallis test indicates no significant difference in oxygen saturation after 60 min in the prone, semirecumbent, and control groups (p = 0.245). The result of the post-hoc in the difference in oxygen saturation among the three groups shows the least significant difference in oxygen saturation between two groups. To determine these groups, the Mann-Whitney test was used. The result of the Mann-Whitney test shows a difference in oxygen saturation between the semirecumbent group and the control group (p = 0.002).
Analysis of the differences in oxygen saturation and comfort level after 60 min (n = 36).
Tests on the other free variables show no significant relationship between the respondents’ characteristic features (i.e., age, sex, mother's education level, nutritional status, immunization status, breastfeeding history, and living environment) and oxygen saturation. A significant relationship is found between mother's education level and comfort level of children under five with pneumonia.
DiscussionPosition adjustment is considered to affect human body functions and various disease conditions. It is associated with the expansion of lungs and the effect of gravity on the functions of the human body5. The results of this study show that the average oxygen saturation increases 60 min after semirecumbent positioning is administered. The semirecumbent position is also known as the 45° semi-upright position.
In a previous study, oxygen saturation was compared with the respiratory muscle strength of infants aged 2-11 months among the supination position, supination with a 45° elevation, and prone position11. The result shows that oxygen saturation undergoes a significant increase in the prone and supination with a 45° elevation positions. Maximum inspiratory pressure increases in the supination position and the supination position with a 45° elevation but not in the prone position. A significant oxygenation increase in the supination position with a 45° elevation is associated with the reduction in the frequency of hypoxia periods in infants11.
Children under five with pneumonia normally experience disruption in the ventilation process caused by the decrease in lung volume and parenchymal lung disorders. To over come the ventilation disruption caused by the decreasing lung volume, the body attempts to compensate by increasing the tidal volume and respiratory rate so that clinical tachypnea and dyspnea are observed with signs of inspiratory effort. The optimum ratio in the ventilation perfusion is not reached, which is a condition called ventilation perfusion mismatch, because of the decrease in ventilation12. Prone and semirecumbent positioning can cause the diaphragm capacity to expand (i.e., increased compliance). Accordingly, the chest wall obtains a uniform movement and the ventilation is distributed well, thus resulting in the increased balance of the perfusion ventilation, which directly increases oxygenation. The prone position can also increase oxygenation through the end-expiratory volume increase mechanism and correct the occurrence venous stasis. Moreover, prone and semirecumbent positioning may reduce the occurrence of gastroesophageal reflux13.
The result of the Wilcoxon test shows no significant effect of prone positioning on oxygen saturation. Nevertheless, the average oxygen saturation increases more after than before prone positioning, but statistically the result is not significantly important.
Oxygen saturation after prone positioning is in the range of 95%-100%. This result is consistent with that of Mancebo et al. (2006)14, who found that the prone position has a positive effect by increasing and maintaining oxygen saturation within normal limits at 95%-100%.
Prone positioning is considered to increase the oxygenation status of patients undergoing respiratory problems. The method is relatively simple and easy to administer, and has no side effects15. Prone positioning may be administered for a long period. For patients with respiratory failure, an increase in the duration of prone positioning may progressively increase oxygenation from 8 h to 16 h since the beginning of the administration16. In this research, the prone position is administered for 60 min only; therefore, the oxygenation status of children under five with pneumonia may not be optimal.
Forty-five newborns were examined in terms of the effect of prone position on the strength of newborns’ respiratory muscles, oxygen saturation, and respiratory rate. The result of the research shows that the prone position increases oxygen saturation and lowers inspiratory pressure unlike in the supination position, and that no difference is found in the respiratory rate in both positions17. Prone positioning has been widely administered as additional therapy for acute respiratory distress syndrome patients18.
Semirecumbent positioning is an effective way to increase a patient's oxygenation status. This research result is in accordance with previous research, which indicated that semirecumbent (45° semi-upright) positioning has a rapid effect on increasing oxygenation in the blood and on reducing endtidal carbon dioxide. The semirecumbent position is easy, safe, and effective to administer on patients with mechanical ventilation and is capable of preventing the occurrence of ventilator-associated pneumonia19.
Oxygenation significantly increases in the semirecumbent position compared with the supination position7. The semirecumbent position is considered more effective in reducing the occurrence of gastroesophageal aspiration than the supination position5. Children with pneumonia are usually more comfortable when placed in a half-sitting position9.
No significant effect on the prone position is observed in the comfort level of children under five with pneumonia in the semirecumbent and control groups. This research result is not consistent with that of Ling, Piccolo, Mulrennan, and Phillips (2011), who found that semirecumbent position could reduce coughing and the use of sedative medicines as well as increase the patient's comfort level compared with the supination position during the administration of bronchoscopy procedures10.
According to Kolcaba, the need for comfort covers physical, psychospiritual, sociocultural, and environmental comforts20,21. Positioning is one attempt to increase a patient's physical comfort. However, the psychospiritual, sociocultural, and environmental comforts are not controlled in this research. Children under five with pneumonia seem to be traumatized by changes in their environmental condition from home to hospital.
Four factors affect a child's coping capacity during hospitalization, namely, child, family, disease condition, and experience in undergoing treatment22,23. As these factors are not controlled in this research, they may affect children's comfort. Future research should assess disease conditions, such as severity of cough, use of invasive tools, use of oxygen, environmental condition, and presence of parents in measuring a child's comfort.
A significant difference exists in oxygen saturation before and after the administration of semirecumbent positioning. No significant difference is found in the comfort level of children under five with pneumonia before and after 60 min in the prone, semirecumbent, and control groups.
Conflicts of interestThe authors declare no conflicts of interest.
