





Q fever (QF) is a zoonotic infection caused by Coxiella burnetii. Previous studies suggest that the incidence in the island of Majorca may be high. The objective was to know the epidemiological, clinical, diagnostic, and therapeutic characteristics of acute QF (AQF) on the island of Majorca during the years 2017–2022.
MethodsRetrospective analysis of a series of cases of AQF diagnosed in 3 out 4 hospitals of the Health Service of the island of Majorca. AQF was considered if a clinically compatible syndrome was present with one of the following serological criteria: confirmed AQF if IgG seroconversion phase II, very possible if only IgG ≥1/128 is available in addition to a positive IgM, and AQF possible if IgG≥ 1/512 with negative IgM or if IgM positive with negative IgG in a single serological determination.
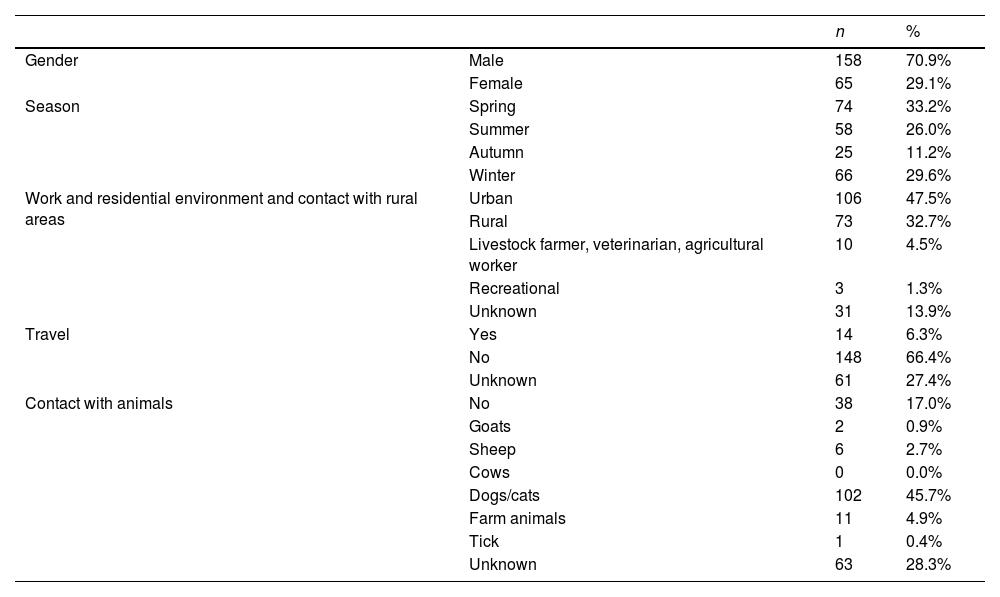
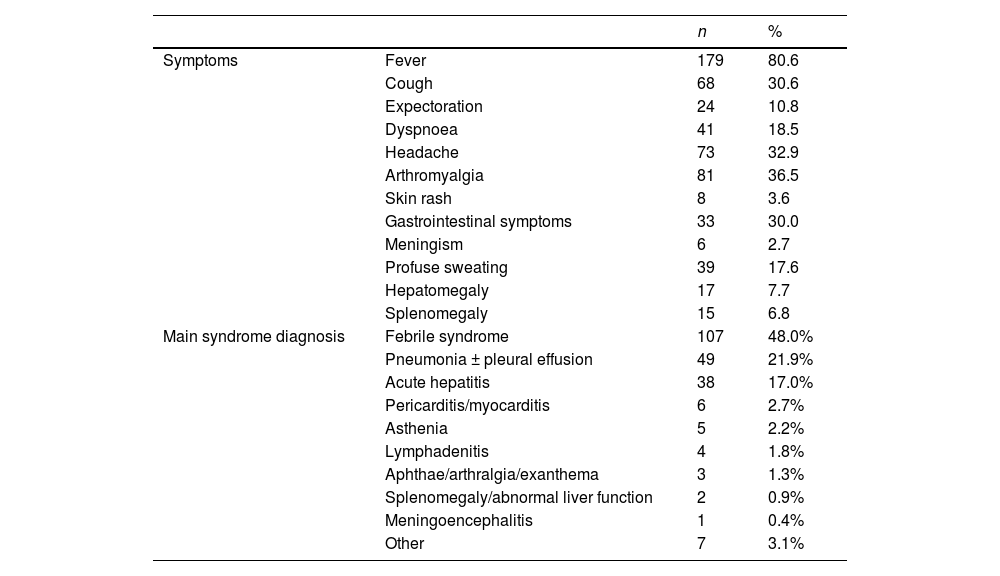
Results223 cases of AQF were diagnosed, of which 102 (45.7%) were confirmed, 84 (37.7%) very probable and 37 (16.6%) probable AQF. Prolonged febrile syndrome was the most frequent clinical diagnosis (107, 48.0%), followed by pneumonia with/without pleural effusion (49, 21.9%), acute hepatitis (38, 17.0%), pericarditis and/or myocarditis (6, 2.6%). Three patients developed endocarditis (one in the acute phase, two others during follow-up). The median number of cases per year was 34 (p25–p75: 31.7–40.25). AQF-related mortality was 1.8% (4 patients).
ConclusionAQF is a preventable and little recognized zoonosis, causing significant morbidity and mortality in Majorca.
La fiebre Q (FQ) es una zoonosis de distribución universal causada por Coxiella burnetii. Estudios previos sugieren que la incidencia en Mallorca puede ser elevada. El objetivo fue conocer las características epidemiológicas, clínicas, diagnósticas y terapéuticas de la FQ aguda (FQA) en la isla de Mallorca durante los años 2017 a 2022.
MétodosAnálisis retrospectivo de una serie de casos de FQA diagnosticados en 3 hospitales del Servicio de Salud de la isla de Mallorca. Se consideró FQA si el cuadro cínico era compatible y cumplían alguno de los siguientes criterios serológicos: FQA confirmada si seroconversión de IgG fase II, muy probable si solo se dispone de una determinación de IgG ≥1/128 además de IgM positiva y FQA probable si IgG ≥1/512 con IgM negativa o si IgM positiva con IgG negativa en una única determinación serológica.
ResultadosSe diagnosticaron en el periodo del estudio 223 casos de FQ aguda, de los cuales 102 (45,7%) FQA confirmada, 84 (37,7%) FQA muy posible y 37 (16,6%) FQA posible. El síndrome febril prolongado fue el diagnóstico clínico más frecuente (107, 48,0%), seguido de la neumonía con/sin derrame pleural (49, 21,9%), hepatitis aguda (38, 17,0%), pericarditis y/o miocarditis (6, 2,6%). Tres pacientes desarrollaron endocarditis (una en la fase aguda, otros dos durante el seguimiento). La mediana de casos por año fue de 34 (p25-p75: 31,7–40,25). Cuatro pacientes (1,4%) fallecieron en relación a la FQA.
ConclusiónLa FQ es una zoonosis prevenible y poco reconocida, causante de una significativa morbimortalidad en Mallorca.
Article
Socio de la Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica
![]()
Para acceder a la revista
Es necesario que lo haga desde la zona privada de la web de la SEIMC, clique aquí
Para realizar los cursos formativos
La actividad estará abierta para socios de la SEIMC. IMPORTANTE, recuerde que requiere registro previo gratuito. Empezar aquí
