


To ascertain the prevalence of obesity and overweight recording in primary care (PC) clinical records.
DesignA descriptive, cross-sectional study.
SettingThe study was conducted in three urban, primary care centers in Gipuzkoa.
Participants620 computerized clinical records were randomly selected from a population of 63,820. Patient age older than 14 years was the only inclusion criterion.
Main measurementsRecording of the clinical episode referring to obesity and/or overweight. Other variables included age, sex, body mass index (BMI), waist circumference, comorbidity (diabetes, hypertension, heart failure, among others), and variability of the record made by healthcare professionals at each center. Statistical analysis included a Chi-square test or a Fisher's test for low frequencies. A value of p<0.05 was considered significant. Analysis was performed using SPSS® v.21 software.
ResultsPrevalence of recorded obesity was 6%, and 78.4% of those with recorded obesity were women. Overweight was recorded in 3% of subjects, of which 33.2% were women. BMI was recorded in 170 cases (27%). At least one comorbidity was found in 241 subjects (39%). Association of BMI with presence of comorbidity was statistically significant (p=0.0001). Recording of obesity was associated to presence of comorbidity (p=0.0002).
ConclusionsThis study confirmed that prevalence of obesity is underestimated, mainly because it is inadequately recorded in clinical histories; that prevalence increases in the presence of other risk factors; and that there is a significant variability in data collection between healthcare professionals.
Conocer la prevalencia del registro de obesidad y sobrepeso en las historias clínicas de atención primaria (AP).
DiseñoEstudio transversal descriptivo.
EmplazamientoEstudio realizado en 3 centros urbanos de atención primaria de Gipuzkoa.
ParticipantesSeiscientas veinte historias clínicas informatizadas extraídas de manera aleatoria de una población de 63.820 pacientes. El único criterio de inclusión fue la edad de los pacientes: mayor de 14 años.
Mediciones principalesRegistro del episodio clínico obesidad y/o sobrepeso. Otras variables: edad, sexo, índice de masa corporal (IMC), perímetro de cintura, comorbilidad (diabetes, hipertensión, insuficiencia cardiaca, entre otras), y variabilidad del registro realizado por los profesionales en cada centro. Para el análisis estadístico se utilizó la prueba Chi-cuadrado o la prueba de Fisher con frecuencias bajas. Se consideró estadísticamente significativo un valor de p<0,05. Los análisis se realizaron con el software SPSS® v.21.
ResultadosLa prevalencia de la obesidad registrada fue del 6%, de los cuales, el 78,4% fueron mujeres. La prevalencia del sobrepeso fue del 3%, siendo mujeres el 33,2%. El IMC se registró en 170 casos (27%). Se encontró al menos una comorbilidad en 241 casos (39%). La asociación del IMC con la presencia de comorbilidad fue estadísticamente significativa, p=0,0001. El registro de obesidad se asoció a la presencia de comorbilidad, p=0,0002.
ConclusionesEste trabajo confirmó que la prevalencia de la obesidad está subestimada, fundamentalmente por la deficiencia de su registro en las historias clínicas; que la prevalencia aumenta si hay otros factores de riesgo presentes, y que existe importante variabilidad en la recogida de datos entre los profesionales.
Obesity is considered as a multifactorial chronic condition with a gradually increasing prevalence, which reaches epidemic proportions in some countries. The impact of this increased prevalence is reflected in the increased risk of cardiovascular diseases and in highly prevalent diseases such as dyslipidemia, metabolic syndrome, or coronary artery disease,1–3 in all of which obesity is an essential etiological factor.
According to the health survey conducted in the Basque Country in 2007,4 44.8% of males and 29.8% of females were overweight, and 13.3% of males and 11.8% of females were obese. This proportion had increased in the prior five years. In females, a socioeconomic gradient was seen in the prevalence of obesity, which was more common as socioeconomic level decreased.5
This study was intended to ascertain the prevalence of obesity detected and recorded in the clinical histories of our patients in order to compare it with the known prevalence in the general population of our region to undertake prevention and treatment strategies. We start from the principle that an inadequately detected or recorded disease will also be inadequately addressed. At the clinics, weight is measured and body mass index (BMI) is calculated in accordance to the Preventive Activity Program (PAP) for the general population, but we hypothesize that recording of these data and consideration of obesity as an independent pathological condition is more frequent if there are other comorbid conditions such as diabetes mellitus (DM) or high blood pressure (HBP). According to some studies,6 variability exists between primary care team members in recording of cardiovascular factors due to factors depending on both patients and professionals, and it has been seen that recording of preventive activities in the clinical history increases with the number of risk factors and/or diseases diagnosed.
Our project is part of a research line started to address a very specific aspect, recording the clinical history of a chronic condition of multifactorial etiology and increasing magnitude.7,8 This study is intended to ascertain the recorded prevalence of obesity and/or overweight in primary care, to consider the presence of other comorbid conditions and their impact on obesity recording, and to know the variability in recording by healthcare professionals.
MethodsDesign and participantsThis was a descriptive, cross-sectional study conducted in three urban primary CARE centers (A, B, and C) from a healthcare area of the province of Gipuzkoa from January 2012 to January 2013. The study population consisted of the 63,820 patients assigned to the participant health centers. Actual prevalence of obesity was considered to be the one reported in the 2007 Basque Country Health Survey.4
The only inclusion criterion was age over 14 years. It was assumed that a sample of 600 clinical histories would allow for estimating obesity and overweight prevalence rates with a 95% confidence interval±5%. This calculation was performed using nQuery Advisor® v.7 software.
VariablesThe primary study variable was recording of the obesity and/or overweight episode. To collect this, the potential ICD-9 codes referring to this condition were identified. Demographic variables such as age and sex were also collected. Other independent variables studied included BMI, waist circumference (WC), presence of comorbid conditions such as DM, HBP, hyperlipidemia, coronary ischemia, congestive heart failure, stroke, sleep apnea syndrome, peripheral venous insufficiency, and hypothyroidism. Information was also collected about the professional in charge of the patient population at each center to ascertain the percentage of episodes recorded by both nursing and medical staff.
Statistical analysisCategorical variables are given as frequencies and percentages (%), and continuous variables as mean and standard deviation (SD). Association between categorical variables was analyzed using a Chi-square test or a Fisher's test in the event of low frequencies. The 95% confidence interval (95% CI) was estimated for prevalence rates of obesity and overweight. A value of p<0.05 was considered statistically significant. Analyses were performed using SPSS® v.21 software.
The Clinical Research Ethics Committee (CREC) of Euskadi approved the conduct of this study.
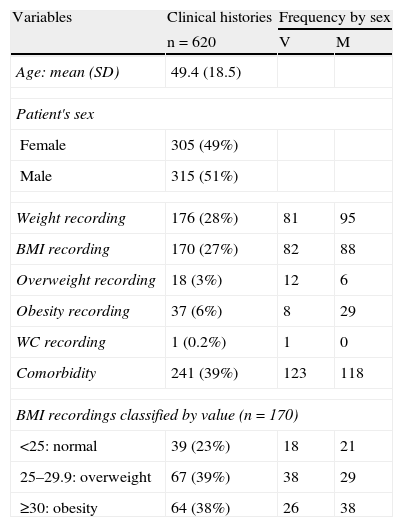
ResultsData from 620 patients were studied. Mean age was 49.4 years (SD: 18.5), and 49% of subjects were females. Weight was recorded in 28% of the clinical histories of subjects reviewed. BMI was recorded for 170 subjects (27%). Overweight was recorded as an independent clinical episode for 18 subjects (3%, 95% CI: 2–4%), six of them women. Obesity was recorded as an independent clinical episode for 37 subjects (6%, 95% CI: 4–8%), 29 of them women. Waist circumference (WC) was recorded for a single subject. At least one comorbidity was found in 241 subjects (39%). Among the 170 BMI values recorded, 64 met the criterion for obesity, but this was only recorded as an episode in 30 subjects (47%). Sixty-seven subjects were overweight, and this was recorded in 17 cases (25%) (Table 1).
Demographic data and records related to weight and obesity in clinical histories.
| Variables | Clinical histories | Frequency by sex | |
| n=620 | V | M | |
| Age: mean (SD) | 49.4 (18.5) | ||
| Patient's sex | |||
| Female | 305 (49%) | ||
| Male | 315 (51%) | ||
| Weight recording | 176 (28%) | 81 | 95 |
| BMI recording | 170 (27%) | 82 | 88 |
| Overweight recording | 18 (3%) | 12 | 6 |
| Obesity recording | 37 (6%) | 8 | 29 |
| WC recording | 1 (0.2%) | 1 | 0 |
| Comorbidity | 241 (39%) | 123 | 118 |
| BMI recordings classified by value (n=170) | |||
| <25: normal | 39 (23%) | 18 | 21 |
| 25–29.9: overweight | 67 (39%) | 38 | 29 |
| ≥30: obesity | 64 (38%) | 26 | 38 |
BMI: body mass index; F: female; WC: waist circumference; M: male.
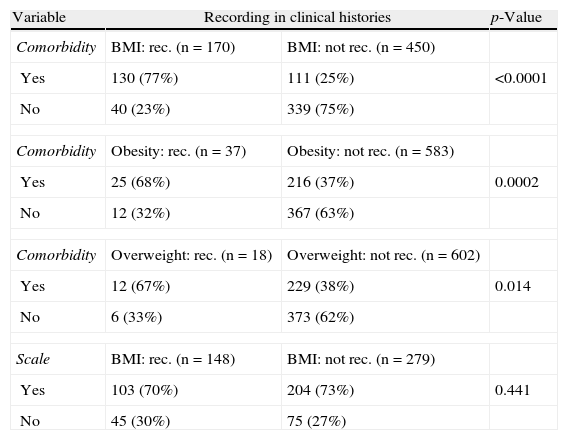
Presence of comorbid conditions related to BMI recording was analyzed, and 77% of subjects for which BMI was recorded had at least one comorbidity (p<0.0001). Recording of obesity as an independent episode in the presence of comorbidity was also found in 68% (p=0.0002). Similarly, recording of overweight in the presence of comorbidity occurred in 67% (p=0.014). BMI was not recorded in 204 subjects, despite availability of a scale at the clinic (Table 2).
Contingency tables for comorbidity, recording of BMI, obesity, and overweight, and scale availability at the clinic.
| Variable | Recording in clinical histories | p-Value | |
| Comorbidity | BMI: rec. (n=170) | BMI: not rec. (n=450) | |
| Yes | 130 (77%) | 111 (25%) | <0.0001 |
| No | 40 (23%) | 339 (75%) | |
| Comorbidity | Obesity: rec. (n=37) | Obesity: not rec. (n=583) | |
| Yes | 25 (68%) | 216 (37%) | 0.0002 |
| No | 12 (32%) | 367 (63%) | |
| Comorbidity | Overweight: rec. (n=18) | Overweight: not rec. (n=602) | |
| Yes | 12 (67%) | 229 (38%) | 0.014 |
| No | 6 (33%) | 373 (62%) | |
| Scale | BMI: rec. (n=148) | BMI: not rec. (n=279) | |
| Yes | 103 (70%) | 204 (73%) | 0.441 |
| No | 45 (30%) | 75 (27%) | |
BMI: body mass index; p: statistical significance.
On the other hand, results showed great variability in recording of obesity and overweight in the 45 physician clinics analyzed. Eleven clinics recorded the obesity/overweight episode in more than 50% of cases, four in 50% of subjects, and 30 in less than 50% of subjects. BMI was recorded in 47% of subjects at center A, in 35.5% of subjects at center B, and in 11% of subjects at center C. Physicians recorded the BMIs of 31 subjects, obesity in 17, and overweight in 9 subjects. All other recordings were made by nursing staff.
DiscussionThe study took as a reference for the actual prevalence of obesity the data published in the 2007 Basque Country Health Survey,4 the last survey conducted before this study, which reported obesity in 13% of males and 12% of females, with a progressive increase in the previous five years. Prevalence in the three study centers in Gipuzkoa, covering 63,820 patients, was consulted in the databases of the Basque Health Service, and obesity episodes were found to be recorded in 3.13% of cases, while BMI≥30 (defining obesity) was recorded in this study in 10% of cases, showing that there were cases which were not recorded as obesity.
In the clinical histories reviewed, obesity was recorded as an independent episode in 6%, and overweight in 3%. A comparison of these data with those published in the Basque Health Survey showed a lower prevalence of obesity and overweight in our study centers.
In our study, a comprehensive data collection was performed, consulting active open episodes in both PAPs and text, which provided a greater number of data. This allowed for finding that, among the 620 clinical histories analyzed, BMI had only been recorded in 170 cases, and 38% of BMI values (10% of the total) revealed obesity. However, of the corresponding cases of obesity, only 6% were recorded as independent episodes in the clinical histories. The same occurred with overweight, present in 39% (11% of the total) according to the BMI criterion but only recorded as an independent episode in 3%. These results are closer to data from the Basque Health Survey, very probably because BMI is more frequently recorded when there are other associated conditions. This demonstrates the little attention paid to obesity as an independent cardiovascular risk factor in clinical histories, despite the fact that it is the initial or adjuvant cause of some of these diseases. When no concomitant disease existed, and despite the finding of a BMI value suggesting obesity or overweight, the affected patient was not duly identified.
Etiology of obesity is multifactorial.9 Obesity and overweight are not mutually exclusive conditions, are part of the same process, and adequate identification of the affected patients is essential to start prevention and treatment.10,11
Variability was also found in obesity and BMI recording both between centers and between professionals in a same center. There were professionals who recorded the great majority of cases of obesity when BMI so advised, and other professionals who recorded almost no episodes of obesity even in patients with associated comorbidity and high BMI values. Few references about variability in PC recording have been found in the literature reviewed,6,12 and additional research on this subject is therefore needed.
We are aware of the limitations of this study, and although data from the study population are comparable by geographical area and sex to those of the reference population, the socioeconomic status of the study population is not available. We think, however, that the differences found in actual prevalence are due to inconsistency of records and the different sensitivity among professionals as regards the recording of the obesity/overweight episode.
Healthcare has a primary role in health promotion and disease prevention.13–18 This study confirmed that prevalence of obesity is greater than observed, mainly because of its deficient recording in clinical histories, and that prevalence increases in the presence of other risk factors.
Major current problems such as obesity, the epidemic of chronic diseases, and social inequalities in health represent complex social problems requiring the joint work of various sectors.19,20 Such complexity requires healthcare professionals who are at the entry gate of the system to make the first effort of adequately collecting and recording data from their patients.
Conflicts of interestThere are no conflicts of interest.
We thank all members of the Research Unit in Primary Care-Donostia, because this study would not have been possible without their invaluable help.
To Pilar Lopetegi Uranga and Isabel Escribano, primary care nurses, for their unselfish collaboration.
Please cite this article as: Gutiérrez Angulo ML, Amenabar Azurmendi MD, Cuesta Solé ML, Prieto Esteban I, Mancebo Martínez S, Iglesias Alonso A. Prevalencia de la obesidad registrada en atención primaria. Endocrinol Nutr. 2014;61:469-473.
