




The consortium for the study of thyroid cancer (CECaT), including 20 hospitals and one research institute, was recently created in Catalonia (Spain). One of the first initiatives of the group was to perform a descriptive analysis of the characteristics of patients with differentiated thyroid carcinoma (DTC).
Patients and methodsThe cohort included 1855 patients from 11 hospitals treated over a period of 15 years (1998–2012).
ResultsIn this series, 1470 (79.2%) patients were women. Mean age was 47.7 (15.7) years. Age was significantly higher in male than in female patients, 49.3 (15) versus 47.3 (15.8); p=0.02. Papillary thyroid carcinoma accounted for 88.9% of cases. Mean tumor size was 21.5 (16)mm, and was significantly lower in females than in males, 20.1 (14.5)mm and 26.6 (20.3)mm respectively (p<0.001). After a follow-up period of 5.5 (3.7) years, information was available for 1355 patient, of whom 1065 (78.6%) were free of disease, 239 (17.6%) had no tumor persistence, and 51 (3.8) % had died. The risk of persistent or recurrent disease was significantly associated to older age at diagnosis, male gender, larger tumor size, lymph node metastases at surgery, no signs of thyroiditis in the remaining thyroid tissue, and presence of vascular and/or extraglandular invasion.
ConclusionsPatient characteristics analyzed are similar to those reported in other parts of the world.
Recientemente, se ha constituido en Cataluña el Consorcio para el Estudio de Cáncer de Tiroides (CECaT). Se trata de una plataforma que reúne 20 hospitales y un instituto de investigación de la comunidad. Una de sus iniciativas ha sido la realización de un estudio retrospectivo de las características de pacientes tratados de cáncer diferenciado de tiroides (CDT).
Material y métodosSe incluyeron 1.855 pacientes de 11 hospitales tratados en el periodo (1998–2012).
ResultadosDel total, 1.470 (79,2%) eran mujeres. La edad media al diagnóstico fue de 47,7 (15,7) años, siendo significativamente mayor en los varones que en las mujeres, 49,3 (15) versus 47,3 (15,8); p=0,02. El 88,9% eran carcinomas papilares. El tamaño del tumor fue de 21,5 (16) mm, siendo significativamente menor en las mujeres que en los hombres, 20,1 (14,5) mm y 26,6 (20,3) mm, respectivamente (p<0,001). Tras un seguimiento de 5,5 (3,8) años, se disponía de la situación final en 1.355 pacientes. De ellos, 1.065 (78,6%) se encontraban libres de enfermedad, 239 (17,6%) mantenían enfermedad activa y 51 (3,8%) habían fallecido. El riesgo de no estar libre de enfermedad se relacionaba de forma significativa con: mayor edad al diagnóstico, sexo masculino, mayor tamaño del tumor, metástasis linfáticas iniciales, ausencia de signos de tiroiditis en el resto de la glándula, y presencia de invasión vascular y/o extraglandular del tumor.
ConclusionesLos resultados muestran que las características del CDT de la cohorte son similares a las descritas en otros ámbitos geográficos.
Differentiated thyroid cancer (DTC) is the most common endocrine neoplasm, and one of the tumors with the greatest increase in incidence in the past 20 years. According to the International Agency for Research on Cancer (IARC), DTC is among the eight most common malignant tumors in European women.1 This same source also stated that the age-standardized rate in Spain is 2.6 and 4.1 per 100,000 in males and females, respectively.1 DTC continues to be a disease with a low prevalence, and collaborative work by hospitals on both care and research strategies is essential. The Consortium for the Study of Thyroid Cancer (CECaT) has recently been created in Catalonia. Comprising 20 Catalan hospitals and one research institute, its purpose is to promote scientific knowledge and to improve the quality of care of patients with DTC. Toward this end, a thyroid cancer register has been created to prospectively record the clinical and pathological characteristics of all cases of DTC. The collection of both histological and blood samples, which will be made available for all researchers in the group, has also been started. Finally, an additional purpose of CECaT is to prepare consensus documents about disease management in order to homogenize the various medical protocols as much as possible.
One of the first initiatives of CECaT has been to conduct a retrospective study of the characteristics of patients treated for DTC over a 15-year period (1998–2012) at the hospitals in the consortium. The purpose of this study was to characterize the profile of DTC in our region. This article reports the study results.
Patients and methodsHospitals integrated in the CECaT were asked if they had records of patients with DTC from the study period. Hospitals having such records were asked to update their data during 2013. We were finally able to include 11 hospitals in the study. Subsequently, the databases were unified and study variables were established based on the following three preconditions having been met: (1) that when codified the different records would be unified into a single record for maximum homogenization of the criteria; (2) that there were at least 500 patients with data available for that variable; and (3) that the variable was relevant from the clinical and histological viewpoint. Patients not undergoing surgery in the 1998–2012 period and those with a diagnosis of thyroid cancer other than follicular epithelium neoplasms were excluded. The following variables were finally recorded: year of birth, age at surgery, sex, year of surgery, result of fine needle aspiration, type of surgery, lymphadenectomy, final histology, histological variant, tumor size, multifocality, vascular and/or extraglandular invasion, regional nodal involvement, distant metastasis, radioiodine therapy, radioiodine dose, follow-up time, persistence/recurrence, final status (according to three categories: disease-free patients, patients with persistent disease, and deceased patients). Persistent/recurrent disease was defined as the presence of disease in any patient who had previously been found to be free of disease. Disease-free was in turn defined as negative findings in the physical examination, neck ultrasound, tests for plasma thyroglobulin and thyroglobulin antibodies and, if applicable, a whole body scan with radioiodine or any other imaging test.
Quantitative variables were presented as mean and standard deviation (SD) or as median and interquartile range (IQR). Categorical variables were given as frequencies and percentages. The inferential study was performed using a Student's t-test and an analysis of variance for quantitative values and with a chi-square test for categorical data. A bivariate analysis was performed to study potential variables related to the final status of the subjects; a multivariate study could not be done because of the small number of patients for some of the variables. A value of p<0.05 was considered statistically significant. Minitab (version 17, Spanish edition) and R (version 3.0.2) software were used. Patient data were collected and processed according to the ethical protocols of each hospital.
ResultsThe final study cohort comprised 1855 patients, 1470 (79.2%) females. Mean age at diagnosis was 47.7 (15.7) years, and was significantly older in males as compared to females, 49.3 (15) versus 47.3 (15.8); (p=0.02). By contrast, there were no significant differences between the various hospitals regarding the different variables collected.
All patients underwent total thyroidectomy, with or without lymphadenectomy. PTC was found in 88.9% of the patients, and no differences were seen in the papillary/follicular carcinoma ratio during the 15-year period. Among the 1111 patients with PTC for whom information was available, 702 (63.2%) were diagnosed with classical variants, while 277 (24.9%) had the follicular variant of PTC. The remaining patients had other less common histological variants. Mean tumor size was 21.5 (16)mm, with significant sex differences. Thus, size was 20.1 (14.5)mm in females, but reached 26.6 (20.3)mm in males (p<0.001). By contrast, there were no size differences depending on patient age (Fig. 1). Fig. 2 shows other baseline tumor characteristics. Among the 896 patients for which data were available, 353 (39.4%) had regional lymphatic metastases at baseline. The mean number of lymph nodes resected by patient was 12.5 (12), and the mean number of lymph nodes invaded by tumor was 3.6 (5.6).

, multifocality (B), extraglandular or vascular invasion (C), and thyroiditis associated with peritumoral tissue (D). NA=patients for whom no data were available.")
Radioiodine ablation of remnant thyroid was performed in 890 of 1056 patients (84.3%) for which data were available, with an initial dose of 117 (35) mCi.
Mean follow-up of the total cohort was 5.5 (3.8) years. During this time, 276 of the 1158 patients (23.8%) with evaluable data had some type or tumor disease persistence and/or recurrence. In addition, 72 (5.78%) had distant metastases.
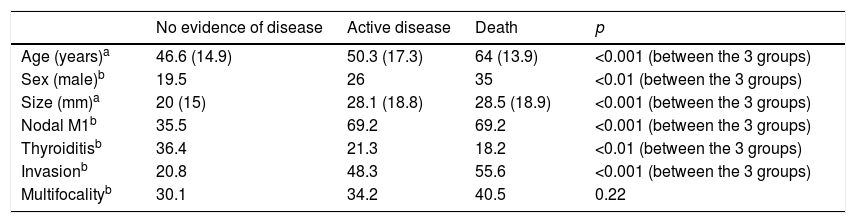
Status at the end of the follow-up period was available for 1355 patients. Of these, 1065 (78.6%) were free of disease, 239 (17.6%) had active disease, and 51 (3.8%) had died (the cause of death was not available in some cases). Finally, an analysis was made of the variables potentially related to the final patient status. A bivariate analysis showed that the risk of not being free of disease at the end of the follow-up period was significantly related to older age at diagnosis, male sex, greater tumor size, lymphatic metastases at baseline, no signs of thyroiditis in the rest of the thyroid gland, and vascular and/or extraglandular invasion by the tumor (Table 1).
Analysis of variables related to final patient status after a mean follow-up of 5.5 (3.8) years.
| No evidence of disease | Active disease | Death | p | |
|---|---|---|---|---|
| Age (years)a | 46.6 (14.9) | 50.3 (17.3) | 64 (13.9) | <0.001 (between the 3 groups) |
| Sex (male)b | 19.5 | 26 | 35 | <0.01 (between the 3 groups) |
| Size (mm)a | 20 (15) | 28.1 (18.8) | 28.5 (18.9) | <0.001 (between the 3 groups) |
| Nodal M1b | 35.5 | 69.2 | 69.2 | <0.001 (between the 3 groups) |
| Thyroiditisb | 36.4 | 21.3 | 18.2 | <0.01 (between the 3 groups) |
| Invasionb | 20.8 | 48.3 | 55.6 | <0.001 (between the 3 groups) |
| Multifocalityb | 30.1 | 34.2 | 40.5 | 0.22 |
Relevant changes have occurred in all aspects related to thyroid cancer in the past 30 years.2,3 Multiple epidemiological studies have shown an increase in the incidence of these tumors, especially in women.4–6 The reasons for this increase are not clear, however, and it has been attributed to both a true increase in incidence and to the improvement and greater use of imaging techniques such as neck ultrasound7–9 On the other hand, a change has also been noted in the proportions of the different histological subtypes, with a clear increase in papillary carcinomas.6,10 Finally, significant changes have also occurred in both treatment approach and follow-up protocols. There is a current trend to an individualized approach, so that more aggressive protocols are only used for patients with a high risk of a poor prognosis.11,12
In recent years, the characteristics of patients with DTC from different regions of the world have been reported.13–20 Analysis of these studies has demonstrated some differences, especially in tumor incidence. As mentioned above, CECaT was created in order to prospectively record and analyze all cases diagnosed in Catalonia. However, its first initiative has been to retrospectively collect the characteristics of patients treated in the 1998–2012 period. The results show a clear female predominance and some differences at diagnosis between the sexes (age and tumor size). A clear predominance of papillary carcinoma (accounting for virtually 90% of DTCs) and the excellent prognosis of this type of cancer are also seen. The relationship between the presence of thyroiditis and the course of the disease is controversial in the literature.21,22 In this study, the absence of signs of thyroiditis in the rest of the thyroid gland was significantly associated with the risk of disease persistence. It should be noted, however, that this data was only recorded for 775 samples.
The results of this study are based on retrospective data collection from several hospitals. Both factors imply significant bias. Thus, this is not a study from which epidemiological conclusions may be drawn. However, the large sample studied represented a sample of the characteristics of patients treated in our region. To minimize bias resulting from the different origin of cases (11 hospitals), an attempt was made to include variables for which codification could not lead to error and for which data were available from more than 500 patients. In the inferential study of factors possibly associated with the course of the disease, the bivariate analysis has a substantial robustness, given the number of patients included. A multivariate study could not be performed, however, because of the small number of patients for whom all study variables were available. Despite these limitations, this is the retrospective study including the highest number of cases of DTC in Spain. The results show that the characteristics of DTC in the cohort are similar to those reported in other regions. The collaboration of the different hospitals to integrate registers of diseases with a low prevalence, such as thyroid cancer, is essential to achieve the data volume required for further research studies.23
Conflict of interestThe authors state that they have no conflicts of interest.
Hospital Arnau de Vilanova (Lleida): Lola Santos, Esmeralda Castelblanco, Ferran Rius. Hospital de Granollers (Granollers): Ignasi Castells. Hospital Germans Trias i Pujol (Badalona): Manel Puig, Jordi L Reverter, Dídac Mauricio. Hospital Vall d’Hebron (Barcelona): Amparo García-Burillo, Carmela Iglesias, Carles Zafon. Hospital Parc Taulí (Sabadell): Maria Rosa Bella, Santi Barcons, Ismael Capel. Hospital Clínic i Provincial, Universitat de Barcelona (Barcelona): Irene Halperin, Mireia Porta, Francisco Lomeña. Hospital Josep Trueta (Girona): Josefina Biarnés. Hospital Joan XXIII (Tarragona): Ana Megía. Hospital Mútua de Terrassa (Terrassa): José Manuel González, Luís García Pascual. Hospital Mataró (Mataró): Enric Ballestar, Eduarda Pizarro, María Teresa Julián. Hospital de la Santa Creu i Sant Pau (Barcelona): Cintia González, Alberto de Leiva, Anna Aulinas. Remaining hospitals and CECaT coordinators: IDIBGI (Girona): Aina Rodríguez. Hospital de Bellvitge (L’Hospitalet de Ll.): Jordi Puig. Hospital Moisés Broggi (Sant Joan Despí): Yolanda Torres. Hospital Santa Tecla i Sant Pau (Tarragona): Mariela Varsavsky. Hospital de Reus (Reus): José María Manzanares. Hospital del Mar (Barcelona): Jaume Puig. Clínica Quirón-Teknon (Barcelona): José Manuel González. Hospital Althaia (Manresa): Eulàlia Colomé. Hospital Universitari de Vic (Vic): Ignasi Saigí. Hospital de Terrassa (Terrassa): Joan Sala.
Please cite this article as: Zafon C, Puig-Domingo M, Biarnés J, Halperin I, Bella MR, Castells I, et al. Estudio descriptivo de las características del cáncer diferenciado de tiroides en Cataluña en el periodo 1998-2012. Registro CECaT. Endocrinol Nutr. 2015;62:264–269.
