






Dyslipidemias are a significant risk factor for cardiovascular diseases. In Peru, nutritional transition and lifestyle changes may be contributing to an increase in the incidence of these metabolic disorders, particularly among the working population.
ObjectiveTo determine the incidence of dyslipidemias and evaluate associated occupational factors in Peruvian workers.
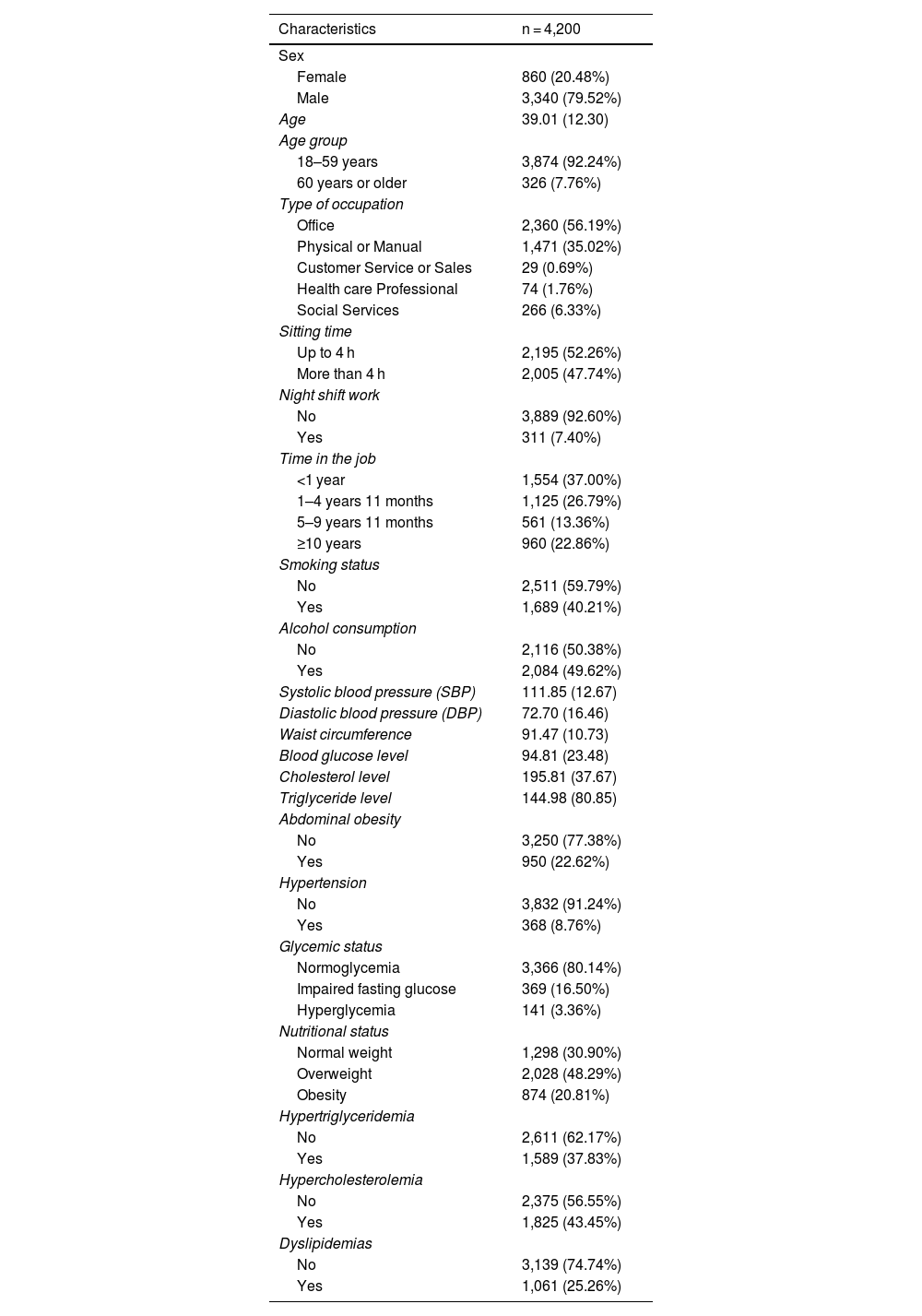
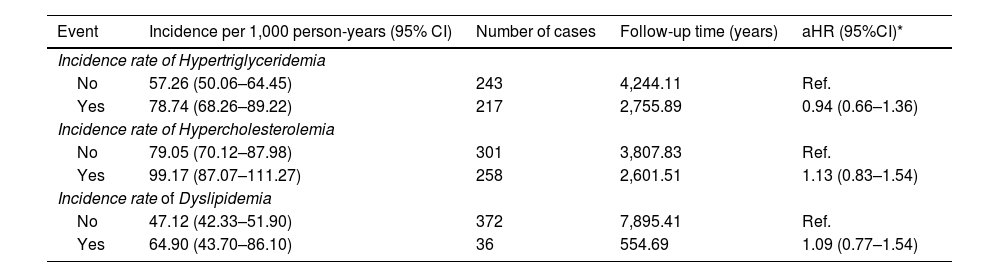
MethodsA retrospective cohort study was conducted using electronic medical records from 4,200 workers attending an occupational health clinic between 2013 and 2022. Incidence rates of hypertriglyceridemia, hypercholesterolemia, and combined dyslipidemia were calculated. Specific occupational factors (type of work, sitting time, and night shift work) were analyzed using Cox regression models adjusted for age (with splines) and sex.
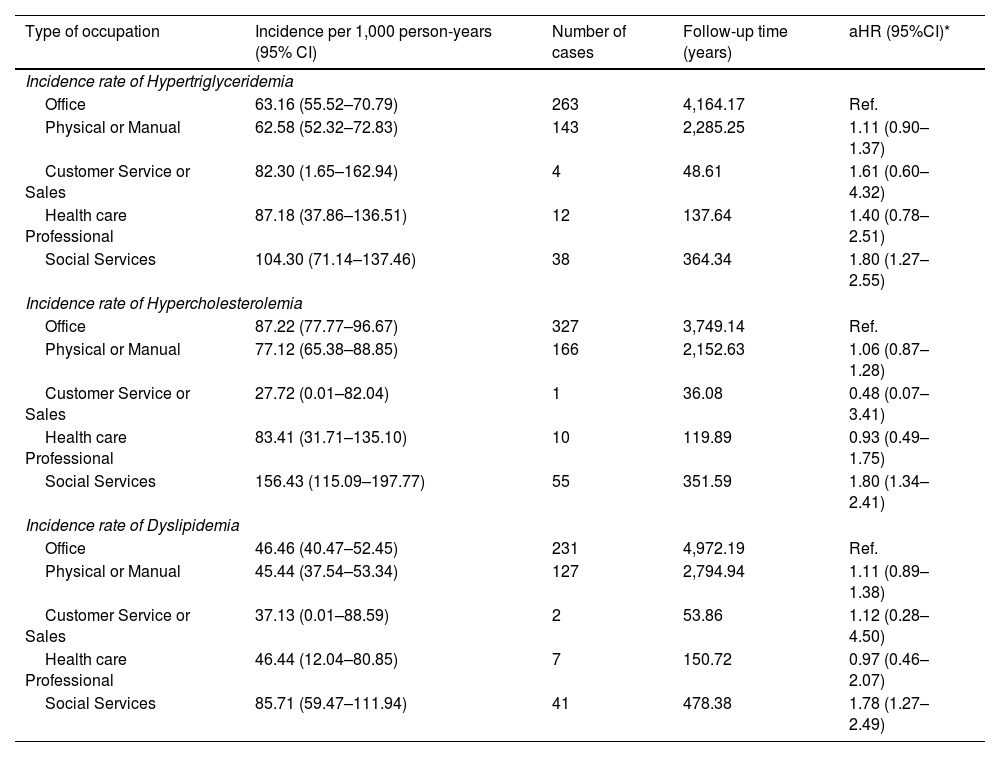
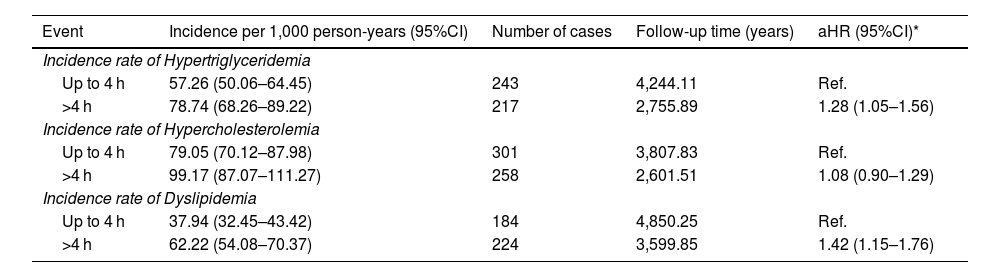
ResultsThe incidence of hypercholesterolemia (87.22 cases per 1,000 person-years; 95% CI: 79.99–94.45) was significantly higher than that of hypertriglyceridemia (65.71 cases per 1,000 person-years; 95% CI: 59.71–71.72). Combined dyslipidemia showed an incidence of 48.28 cases per 1,000 person-years (95% CI: 43.60–52.97). Workers in social services had a higher risk of developing dyslipidemias (aHR: 1.78; 95% CI: 1.27–2.49) compared to office workers. Prolonged sitting time (>4 h) was significantly associated with an increased risk of hypertriglyceridemia (aHR: 1.28; 95% CI: 1.05–1.56) and combined dyslipidemia (aHR: 1.42; 95% CI: 1.15–1.76).
ConclusionsThe high incidence of dyslipidemias—particularly hypercholesterolemia—may reflect the increasing consumption of ultra-processed foods and the ongoing nutritional transition in the Peruvian population. Occupational factors play a crucial role in the development of these metabolic disorders, highlighting the need for specific preventive strategies in the workplace.
Las dislipidemias constituyen un factor de riesgo significativo para enfermedades cardiovasculares. En Perú, la transición nutricional y los cambios en los estilos de vida podrían estar incrementando la incidencia de estas alteraciones metabólicas, especialmente en la población trabajadora.
ObjetivoDeterminar la incidencia de dislipidemias y evaluar los factores ocupacionales asociados en trabajadores peruanos.
MetodologíaEstudio de cohorte retrospectivo basado en registros médicos electrónicos de 4,200 trabajadores atendidos en una clínica ocupacional entre 2013 y 2022. Se calcularon las tasas de incidencia de hipertrigliceridemia, hipercolesterolemia y dislipidemia combinada. Se analizaron factores ocupacionales específicos (tipo de trabajo, tiempo sentado y trabajo nocturno) mediante modelos de regresión de Cox ajustados por edad (en splines) y sexo.
ResultadosLa incidencia de hipercolesterolemia (87.22 casos/1,000 personas-año; IC 95%: 79.99–94.45) fue significativamente mayor que la de hipertrigliceridemia (65.71 casos/1,000 personas-año; IC 95%: 59.71–71.72). La dislipidemia combinada presentó una incidencia de 48.28 casos/1,000 personas-año (IC 95%: 43.60–52.97). Los trabajadores de servicios sociales mostraron mayor riesgo de desarrollar dislipidemias (HRa: 1.78; IC 95%: 1.27–2.49) comparados con trabajadores de oficina. El tiempo sentado prolongado (>4 horas) se asoció significativamente con mayor riesgo de hipertrigliceridemia (HRa: 1.28; IC 95%: 1.05–1.56) y dislipidemia combinada (HRa: 1.42; IC 95%: 1.15–1.76).
ConclusionesLa alta incidencia de dislipidemias, particularmente hipercolesterolemia, refleja posiblemente el incremento en el consumo de alimentos ultraprocesados y la transición nutricional en la población peruana. Los factores ocupacionales juegan un papel determinante en el desarrollo de estas alteraciones metabólicas, subrayando la necesidad de implementar estrategias preventivas específicas en el ámbito laboral.
