





More than 50% of first cardiovascular events (CVE) occur in populations identified as at low or intermediate risk by the risk equations, so the inclusion of additional variables, such as polygenic risk scores (PRS), has been proposed to improve the predictive capacity of these equations. The aim of this study was to assess whether a PRS, independently or with clinical risk equations, is associated with the presence, severity and extent of subclinical atherosclerosis.
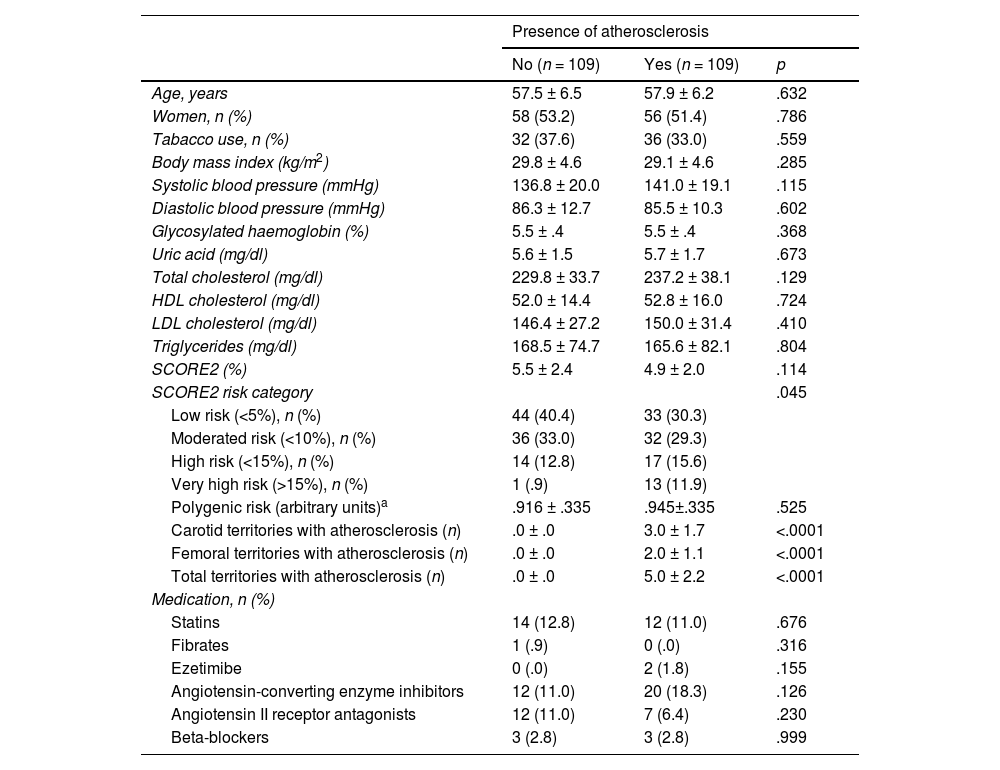
Methods109 subjects with atherosclerosis were selected from the ILERVAS cohort (primary prevention) and matched with 109 participants without atherosclerosis of the same age, sex and SCORE2 risk level. Atherosclerosis was assessed and quantified by arterial wall vascular ultrasound in 12 territories, and PRS was estimated using the Cardio inCode Score®. The predictive capacity of the presence of subclinical atherosclerosis was estimated, as well as the association between the extent and severity of atherosclerosis with PRS and clinical risk (SCORE2).
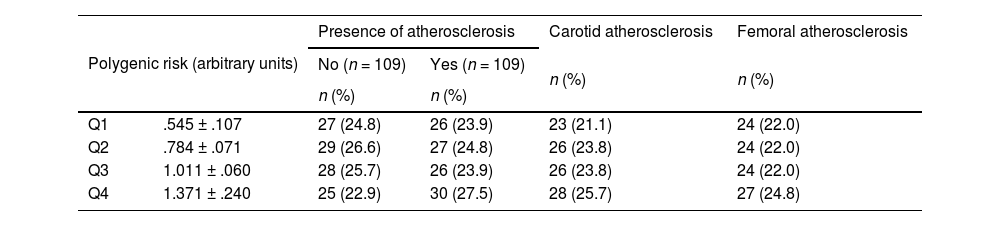
ResultsPRS was similar between participants with or without atherosclerosis (P = .525). We did not find an association between PRS and SCORE2 (r = −.29, P = .709), and the addition of PRS to SCORE2 did not improve the prediction of atherosclerosis [AUC (95% CI) = .566 (.477, .654, P = .148). The extent of atherosclerosis was related to SCORE2 (P = .009), but not to PRS (P = .709).
ConclusionsThe Selected PRS is not associated with the presence of atherosclerosis or clinical risk, suggesting that its additional contribution to CVE risk would be mediated by mechanisms independent of the development of atherosclerosis. Additional biomarkers are needed to improve the prediction of subclinical atherosclerosis without using imaging tests as a first step in personalised assessment.
Más de un 50% de primeros eventos cardiovasculares (ECV) ocurren en población identificada como de riesgo bajo o intermedio por las ecuaciones de riesgo, por lo que se ha propuesto la inclusión de variables adicionales, como puntuaciones de riesgo poligénicos (PRP), para mejorar la capacidad predictiva de estas ecuaciones. El objetivo de este estudio fue evaluar si una PRP, independientemente o junto a las ecuaciones de riesgo clínico, se asocia a la presencia, gravedad y extensión de aterosclerosis subclínica.
MétodosSe seleccionaron 109 sujetos con aterosclerosis de la cohorte ILERVAS (prevención primaria) y se aparearon con 109 participantes sin aterosclerosis de la misma edad, sexo y nivel de riesgo SCORE2. Se evaluó y cuantificó la aterosclerosis en 12 territorios mediante ecografía vascular de pared arterial y se estimó la PRP mediante el Cardio inCode Score®. Se estimó la capacidad de predicción de presencia de aterosclerosis subclínica, y la asociación entre la extensión y gravedad de la aterosclerosis con la PRP y el riesgo clínico (SCORE2).
ResultadosLa PRP fue similar entre participantes con o sin aterosclerosis (P = 0.525). No encontramos una asociación entre la PRP y el SCORE2 (r= -0.29, P = 0.709), y la adición de la PRP al SCORE2 no mejoró la predicción de aterosclerosis [AUC (95% IC)= 0.566 (0.477, 0.654, P = 0.148). La extensión de la aterosclerosis se relacionó con el SCORE2 (P = 0.009), pero no con la PRP (P = 0.709).
ConclusionesLa PRP seleccionada no se asocia con la presencia de aterosclerosis ni con el riesgo clínico, sugiriendo que su contribución adicional al riesgo de ECV se mediaría por mecanismos independientes al desarrollo de aterosclerosis. Se necesitan biomarcadores adicionales para mejorar la predicción de aterosclerosis subclínica sin recurrir a pruebas de imagen como primer paso en la evaluación personalizada.