




Childhood and adolescence are key stages to promote a healthy lifestyle.
ObjectiveTo analyse the relationship between weight status, physical activity and the Mediterranean diet in schoolchildren in the Region of Murcia.
MethodsCross-sectional descriptive study with 520 schoolchildren aged 8–17 years. The weight status was calculated through the body mass index. The Mediterranean diet was found through the KIDMED questionnaire and physical activity was estimated using the IPAQ-C and IPAQ-A questionnaires.
ResultsThe Mediterranean diet is not significantly associated with sex (p<0.537) or weight status (p<0.417) but it maintains a relationship of dependence with age (p<0.010) and the level of physical activity (p<0.000). Schoolchildren in normal weight and assets have a greater follow-up to the Mediterranean diet than their overweight and sedentary peers (p<0.000).
ConclusionThe fat but fit phenomenon applied to the Mediterranean diet is confirmed.
La infancia y la adolescencia son etapas clave para promocionar un estilo de vida saludable.
ObjetivoAnalizar la relación entre el estado de peso, la actividad física y la dieta mediterránea en escolares de la Región de Murcia.
MétodosEstudio descriptivo transversal con 520 escolares de 8-17 años. El estado de peso se calculó a través del índice de masa corporal. La adherencia a la dieta mediterránea se halló a través del cuestionario KIDMED, y la actividad física se estimó utilizando los cuestionarios IPAQ-C e IPAQ-A.
ResultadosLa dieta mediterránea no se asocia significativamente con el sexo (p<0,537) ni el estado de peso (p<0,417) pero sí mantiene una relación de dependencia con la edad (p<0,010) y el nivel de actividad física (p<0,000). Los escolares en normopeso y activos tienen un mayor seguimiento de la dieta mediterránea que sus pares en sobrepeso y sedentarios (p<0,000).
ConclusiónSe confirma el fenómeno «fat but fit» aplicado a la dieta mediterránea.
In Spain, the prevalence of children being overweight and leading a sedentary lifestyle is currently one of the highest in Europe.1,2 Such findings have led to the coining of the term “cardiodiabesity” to define and describe the well-known relationship between obesity, type 2 diabetes mellitus, metabolic syndrome and cardiovascular disease.3 A holistic approach to primary cardiodiabesity prevention measures has proposed examining all combined cardiovascular risk factors and their relationship with the Mediterranean diet (MD).4
It has been found that physical fitness helps to mediate the risk of obesity-related mortality.5 This phenomenon, known as “fat but fit”, which refers to obese individuals with a high level of fitness, suggests that cardiovascular fitness offsets the risk of metabolic and cardiovascular disease irrespective of body mass index, including among the obese population.6
The nutrigenetic effects of following the MD have been shown to improve the lipid profile.5 Recent studies have found that adherence to the MD mitigates the onset of cardiometabolic phenotypes in subjects who are genetically susceptible to cardiovascular disease, which is the primary cause of morbidity and mortality in the 21st century.6 Another beneficial effect of the MD directly associated with weight management and controlling weight status and protective mechanisms of the diet's intrinsic components was found to be the “Mediterranean paradox”,4 defined as a lower absolute risk of coronary heart disease despite the same level of exposure to a particular risk factor.6 A healthy MD has also been associated with greater life satisfaction,7 greater mental well-being5 and a greater socioeconomic status of parents.8,9 Some studies have compared the MD based on gender, revealing a higher quality diet in males than in females1 and greater adherence at a younger age compared to older children.10
Epidemiological studies have concluded that the MD, as well as being a model for a healthy diet, represents a lifestyle limited to a specific climate. In this sense, the changing tendency of the population towards a higher intake of processed foods, saturated fats and reduced consumption of plant-based foods and monounsaturated fatty acids largely reveals a loss of cultural heritage that the MD represents.11 The MD is defined as the eating habits prevalent at the beginning of the 1960s in Mediterranean countries where olives grow (Greece, southern Italy and Spain).12 It is characterised by a high intake of plant-based foods (primarily whole grains), olive oil as the primary source of fat, a moderate intake of dairy products, moderate consumption of fish and meat, moderate consumption of wine at meal times and an active lifestyle.13 Further aspects associated with lifestyle have recently been added, such as sociability, eating with family and friends and physical exercise.12
Higher consumption of vegetables and vegetable oils, pasta, rice, fish, white meat and wine have been associated with people who are more physically active.14 This approach takes into account the probable interactions between components of the diet and other lifestyle habits, and may be better suited to identifying behavioural factors that could lead to improved health.4 A healthier diet, characterised by “fruit, vegetables and fish”, coupled with moderate physical activity (PA) in women and vigorous PA in men may be associated with improved health.15–18 However, some studies have found no correlation between the MD, weight status and gender.19,20
Other studies have shown inverse correlations between weight status parameters and the MD, as well as associations between the MD and vigorous PA in primary school children.5 Overall, a low incidence of obesity and being overweight has been found in school children and adolescents with low adherence to the MD and low levels of physical activity.21
This highlights the importance of conducting studies and research to identify the causes that are most associated with childhood obesity and being overweight,2 generating data of general interest that could help to prevent and raise awareness of these types of disease. This is particularly relevant as, in Spain, like in many other European countries, the Mediterranean diet is unfortunately being increasingly abandoned.5
Based on the above findings, the following study hypotheses were considered: (a) there is no correlation between gender, age and the MD; (b) weight status is not associated with the MD; (c) adherence to the MD is higher in school children who are more physically active; (d) regardless of weight status, adherence to the MD is higher in school children who are more physically active (“fat but fit” phenomenon). The aim of this study was to analyse if weight status (normal weight, overweight or obese), PA level (low, moderate or high) and the MD (low, moderate or high) are correlated in school children aged 8–17 years.
Material and methodParticipantsA retrospective, descriptive, cross-sectional study was designed with a representative sample of school children from three state schools in the Region of Murcia (Spain) with a medium-high socioeconomic status. A total of 520 children took part in the study (219 boys and 301 girls, mean±standard deviation: 12.81 years±2.997), who were selected non-randomly and for convenience. The personal data of the respondents was protected in order to safeguard their rights, safety and well-being. All the school children took part voluntarily in accordance with the ethical principles of the Declaration of Helsinki (2013).
Variables and instrumentsWeight and height were measured using an electronic balance (TANITA TBF 300A, USA) and a stadiometer (SECA A800, USA), accurate to 100g and 1mm, respectively, following the protocol of the International Society for the Advancement of Kinanthropometry (ISAK), by level i qualified personnel. Nutritional status was diagnosed by age- and gender-adjusted body mass index.22 The participants were categorised into three nutritional status groups (normal weight, overweight and obese).
The MD was evaluated using the KIDMED Mediterranean diet Adherence Test, comprising 16 dichotomous questions that must be answered either affirmatively or negatively (yes/no). The participants’ mean score for each item was calculated to produce an overall assessment, categorising the school children into three groups: low, X≤3; moderate, 3<X>8; and high, X≥8. Affirmative answers to questions that represent a positive aspect score one point, while one point is subtracted for affirmative answers to questions that represent a negative connotation. No points are given for negative answers.23
The Physical Activity Questionnaire for Children aged 8–14 years (PAQ-C)24 and the Physical Activity Questionnaire for Adolescents aged 15–17 years (PAQ-A)25 were used to assess PA. Both questionnaires are very easy to complete and assess the children's PA over the previous seven days. The results of these questionnaires were given in metabolic equivalents (MET), which enabled the population to be categorised into three levels of activity depending on certain PA intensity and duration criteria: low, moderate and high.26
Statistical analysisThe normality and homoscedasticity of the distributions was obtained using the Kolmogorov–Smirnov test and Levene's test, respectively. As non-normal distribution was observed in some of the PA and MD adherence score distributions, a non-parametric analysis was conducted depending on the various levels of gender and body mass index variables. Percentages were calculated for categorical variables. Contingency tables and Pearson's χ2 test were used, with analysis of residuals for the categorical variables. The Kruskal–Wallis test was used to compare the independent samples. The effect size (r) was calculated by applying the formula Z/√N (Z divided by the square root of N). The level of significance was established at 5% (p≤0.05). The data were analysed using the SPSS statistical software package (v.24.0 by SPSS Inc., Chicago, Illinois, USA) for Windows.
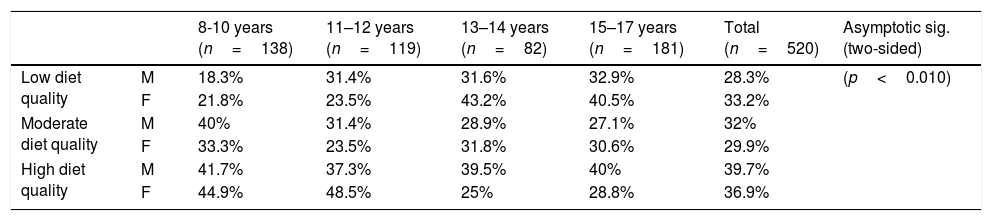
ResultsThe sample comprised 520 school children (57.8% female and 42.2% male) aged between 8 and 17 years. The quality of the MD according to gender and age is analysed in Table 1. Differences in MD quality were observed between the different age groups (X2(1)=11,403; p<0.010). MD quality was found to be highest in the 8–10 and 15–17 age groups (Md=60), followed by the 11–12 age group (Md=52) and the 13-14 age group (Md=26).
Correlation between diet quality, age and gender.
| 8-10 years (n=138) | 11–12 years (n=119) | 13–14 years (n=82) | 15–17 years (n=181) | Total (n=520) | Asymptotic sig. (two-sided) | ||
|---|---|---|---|---|---|---|---|
| Low diet quality | M | 18.3% | 31.4% | 31.6% | 32.9% | 28.3% | (p<0.010) |
| F | 21.8% | 23.5% | 43.2% | 40.5% | 33.2% | ||
| Moderate diet quality | M | 40% | 31.4% | 28.9% | 27.1% | 32% | |
| F | 33.3% | 23.5% | 31.8% | 30.6% | 29.9% | ||
| High diet quality | M | 41.7% | 37.3% | 39.5% | 40% | 39.7% | |
| F | 44.9% | 48.5% | 25% | 28.8% | 36.9% |
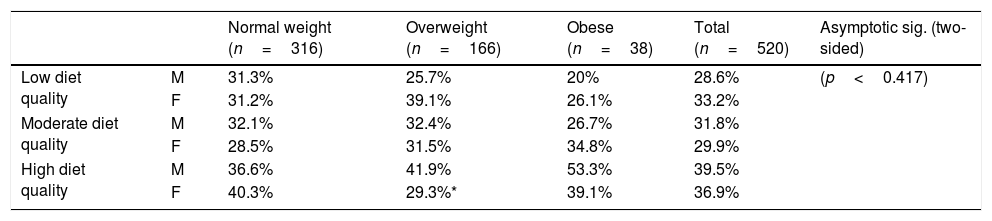
As shown in Table 2, no correlation was found between MD quality and weight status (X2(1)=1.750; p<0.417). However, weight increase was associated with a decline in low diet quality.
Correlation between diet quality and weight status.
| Normal weight (n=316) | Overweight (n=166) | Obese (n=38) | Total (n=520) | Asymptotic sig. (two-sided) | ||
|---|---|---|---|---|---|---|
| Low diet quality | M | 31.3% | 25.7% | 20% | 28.6% | (p<0.417) |
| F | 31.2% | 39.1% | 26.1% | 33.2% | ||
| Moderate diet quality | M | 32.1% | 32.4% | 26.7% | 31.8% | |
| F | 28.5% | 31.5% | 34.8% | 29.9% | ||
| High diet quality | M | 36.6% | 41.9% | 53.3% | 39.5% | |
| F | 40.3% | 29.3%* | 39.1% | 36.9% |
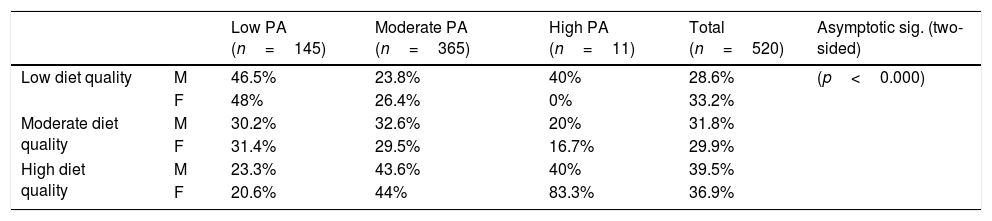
Table 3 highlights the relationship between MD quality and level of PA (X2(1)=32,653; p<0.000). Greatest MD quality was found in the moderate PA group (Md=160), followed by the low PA group (Md=31) and finally the high PA group (Md=7).
Correlation between diet quality and level of PA.
| Low PA (n=145) | Moderate PA (n=365) | High PA (n=11) | Total (n=520) | Asymptotic sig. (two-sided) | ||
|---|---|---|---|---|---|---|
| Low diet quality | M | 46.5% | 23.8% | 40% | 28.6% | (p<0.000) |
| F | 48% | 26.4% | 0% | 33.2% | ||
| Moderate diet quality | M | 30.2% | 32.6% | 20% | 31.8% | |
| F | 31.4% | 29.5% | 16.7% | 29.9% | ||
| High diet quality | M | 23.3% | 43.6% | 40% | 39.5% | |
| F | 20.6% | 44% | 83.3% | 36.9% |
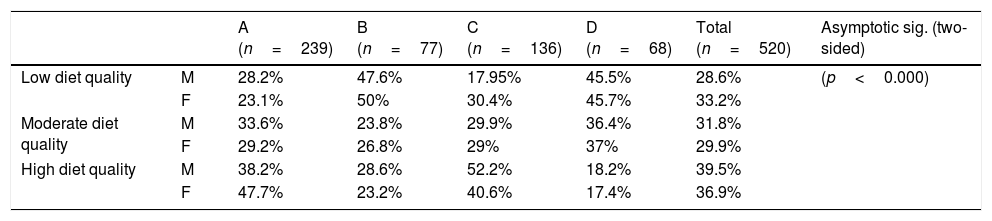
To complete the analysis, it was also determined whether MD quality was related to weight status and PA level together (Table 4). Differences in the MD were found when compared with weight status and PA level (X2(1)=31.799; p<0.000). The MD quality was highest in the normal weight/active group (Md=104), followed by the overweight-obese/active group (Md=63), the normal weight/inactive group (Md=19) and the overweight-obese/inactive group (Md=12).
Combined association between weight status and physical activity, and diet quality.
| A (n=239) | B (n=77) | C (n=136) | D (n=68) | Total (n=520) | Asymptotic sig. (two-sided) | ||
|---|---|---|---|---|---|---|---|
| Low diet quality | M | 28.2% | 47.6% | 17.95% | 45.5% | 28.6% | (p<0.000) |
| F | 23.1% | 50% | 30.4% | 45.7% | 33.2% | ||
| Moderate diet quality | M | 33.6% | 23.8% | 29.9% | 36.4% | 31.8% | |
| F | 29.2% | 26.8% | 29% | 37% | 29.9% | ||
| High diet quality | M | 38.2% | 28.6% | 52.2% | 18.2% | 39.5% | |
| F | 47.7% | 23.2% | 40.6% | 17.4% | 36.9% |
A=normal weight/active; B=normal weight/inactive; C=overweight-obese/active; D=overweight-obese/inactive.
The aim of this study was to analyse if weight status (normal weight, overweight or obese), PA level (low, moderate or high) and adherence to the MD (low, moderate or high) were correlated in a sample of Spanish school children aged 8–17 years. The χ2 and Kruskal–allis H tests performed revealed a positive association between PA and the MD, confirming the hypothesis that adherence to the MD is higher in more physically active school children, regardless of their weight (see Table 4). These findings can be explained by the “fat but fit” phenomenon, which reflects the paradox that people who are overweight or obese but undertake acceptably high levels of PA may experience health benefits both now and in the future, compared to people who are equally overweight or obese but are not physically fit.27
This would suggest that appropriate levels of physical fitness should be the primary strategy followed to reduce the risk of mortality in the broader overweight and obese population,5 and to help achieve a healthy body weight.6
The Mediterranean region has recently undergone a transition towards a more westernised diet, with significant differences recorded between the various Mediterranean countries depending on their agricultural and cultural context.4 For this reason, some studies hypothesise that this association between PA and MD may be conditioned by the geographical area in which the participants live, their nationality, socioeconomic status and level of PA,28,29 since living close to facilities that lend themselves to physical exercise, and in an environment that promotes a balanced diet, helps to maintain a healthy lifestyle.2
The results are even more important when considering a child and adolescent population, as the evidence suggests that lifestyle habits acquired during childhood and adolescence will persist in adulthood. As a result, during these key periods in which an individual's personality and lifestyle are being moulded and consolidated, it is vital to understand the influence of the MD and risk factors for health, and to promote the “Mediterranean paradox”.6,14
This study also found that age influences the MD (p<0.010). Greater MD quality was seen in the 8–10 and 15–17 age groups (Md=60) than in the 11–2 and 13–4 age groups (Md=52; Md=26, respectively). It should also be noted that the percentage of children eating a low-quality MD increased with age and that there were higher percentages of children eating a high-quality MD for both genders (see Table 1). Other studies that have analysed the MD based on age and gender in European populations reveal similar findings, with most concluding that school children adhere to an optimal MD with no significant differences between the genders,2,5,20 and identifying a clear trend towards abandonment of the Mediterranean lifestyle,29 which may be influencing the obesity epidemic affecting school-aged children.2
However, no clear trend was identified on analysing anthropometric values against the MD, as most studies that evaluated these parameters found no significant differences in MD between the various groups.19,28,30,31 This is consistent with the results of this study, which found no correlation between the MD and weight status (p<0.417). However, weight increase was associated with a decline in low MD quality, with overweight-obese boys tending to adhere to a higher-quality MD than girls (see Table 2). The lack of consistency in these correlations could be explained by overweight or obese participants changing their diets during the study, the influence of other factors such as the effects detailed above, or differences in PA.28
Although the general population is increasingly aware of the importance of maintaining a normal weight, it continues to be one of the most controversial social topics of our time, which is why longitudinal experimental studies on weight gain and its causes in today's society need to be conducted.9
An association between the MD and PA level (p<0.000) is shown in Table 3, with a higher quality MD recorded in the moderate PA group (Md=160). Furthermore, higher percentages of respondents of both genders from the high PA group adhered to a high quality MD. These results differ from some studies31 and are consistent with others, highlighting the role PA plays in influencing the association between the MD and lipid profile.4 These correlations indicate that children with healthy eating habits are more likely to be physically active and lead a less sedentary lifestyle.9,14
Therefore, increasing adherence to the MD and vigorous PA may be effective educational strategies for preventing subsequent obesity-related comorbidities, since the implementation of programmes designed to increase PA levels has resulted in reduced weight gain and increased MD quality.10,32,33
There are two types of obesity prevention strategies in schools: on the one hand, strategies focussed on increasing levels of PA and, on the other, strategies that also include an educational element and nutritional assessment.34 The possibility of including diet and nutrition classes in the national curriculum should be considered in order to encourage school children to adopt optimal lifestyles to improve their health.14,35 Physical Education departments should encourage the acquisition of these healthy habits and behaviours that will last a lifetime.19,36 Furthermore, it should be incumbent upon families, schools and healthcare professionals to create a favourable environment that increases participation in physical activity.14,37
The MD has been studied in children and adolescents in a number of countries, but this is the first study to examine the possible combined association between the MD, and weight status and PA together in a broad sample of school children aged from 8 to 17 years in the Region of Murcia, Spain. Other studies have reported the cause–effect relationship of adherence to the MD, employing more objective methods like the level of physical fitness, blood pressure, anthropometric measurements and healthy habits associated with following the MD. Nevertheless, both the International Physical Activity Questionnaire (IPAQ) and the KIDMED test are validated questionnaires and appropriate measuring tools for use in a variety of contexts.23–25
An inherent limitation of diet-based studies is that reporting bias due to the social propensity of over-reporting consumption of healthier foods and under-reporting consumption of less favourable foods cannot be ruled out. Future studies should take the socioeconomic status of the family into account, as this variable could influence the degree of association with the MD.
In light of the results obtained, it can be concluded that the MD is not influenced by gender or weight, but that a correlation does exist between the MD and physically active school children of a normal weight. The study also confirmed that the “fat but fit” phenomenon applies to the MD. As such, given the link between a healthy lifestyle and improved mental well-being, the MD should be promoted to young people worldwide. Emphasis should be placed on increasing levels of PA, reducing sedentary behaviour and promoting healthy eating habits.5,37,38
Ethical responsibilitiesProtection of people and animalsThe authors declare that the procedures followed conformed to the ethical standards of the responsible human experimentation committee and to the World Medical Association and the Declaration of Helsinki.
Data confidentialityThe authors declare that they have followed the protocols implemented in their place of work regarding the publication of patient data.
Right to privacy and informed consentThe authors have obtained the informed consent of the patients and/or subjects referred to in the article. This document is in the possession of the corresponding author.
Conflicts of interestNo conflicts of interest.
Please cite this article as: Rosa Guillamón A, Carrillo López PJ, García Cantó E, Perez Soto JJ, Tarraga Marcos L, Tarraga López PJ. Dieta mediterránea, estado de peso y actividad física en escolares de la Región de Murcia. Clin Investig Arterioscler. 2019;31:1–7.