





Colorectal cancer (CRC) is one of the most frequent neoplasms in both men and women. It is the fourth cause of cancer death in our setting. Meanwhile, renal cancer represents 2% of all tumors, and renal cell carcinoma (RCC) is the most frequent type.1
The simultaneous presentation of renal cell and colorectal cancer is exceptional, with a prevalence that ranges between 0.03% and 4.85%.2 The systematic use of non-invasive imaging tests like computed tomography (CT) has increased the diagnosis of asymptomatic renal tumors. This favors subclinical diagnosis at early stages of the disease.3
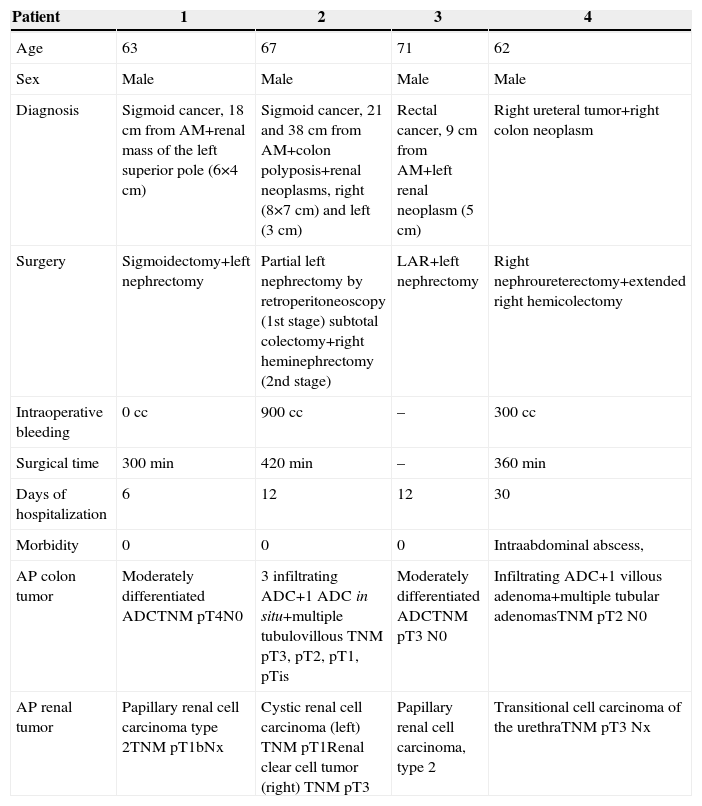
Currently, the laparoscopic approach of CRC and RCC is well established. Simultaneous colectomy and partial nephrectomy have been achieved anecdotally. Below, we present 4 clinical cases, which are included in Table 1.
Cases Reported.
| Patient | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Age | 63 | 67 | 71 | 62 |
| Sex | Male | Male | Male | Male |
| Diagnosis | Sigmoid cancer, 18cm from AM+renal mass of the left superior pole (6×4cm) | Sigmoid cancer, 21 and 38cm from AM+colon polyposis+renal neoplasms, right (8×7cm) and left (3cm) | Rectal cancer, 9cm from AM+left renal neoplasm (5cm) | Right ureteral tumor+right colon neoplasm |
| Surgery | Sigmoidectomy+left nephrectomy | Partial left nephrectomy by retroperitoneoscopy (1st stage) subtotal colectomy+right heminephrectomy (2nd stage) | LAR+left nephrectomy | Right nephroureterectomy+extended right hemicolectomy |
| Intraoperative bleeding | 0cc | 900cc | – | 300cc |
| Surgical time | 300min | 420min | – | 360min |
| Days of hospitalization | 6 | 12 | 12 | 30 |
| Morbidity | 0 | 0 | 0 | Intraabdominal abscess, |
| AP colon tumor | Moderately differentiated ADCTNM pT4N0 | 3 infiltrating ADC+1 ADC in situ+multiple tubulovillous TNM pT3, pT2, pT1, pTis | Moderately differentiated ADCTNM pT3 N0 | Infiltrating ADC+1 villous adenoma+multiple tubular adenomasTNM pT2 N0 |
| AP renal tumor | Papillary renal cell carcinoma type 2TNM pT1bNx | Cystic renal cell carcinoma (left) TNM pT1Renal clear cell tumor (right) TNM pT3 | Papillary renal cell carcinoma, type 2 | Transitional cell carcinoma of the urethraTNM pT3 Nx |
AM: anal margin; ADC: adenocarcinoma; AP: anatomic pathology; LAR: lower anterior resection.
The association between CRC and RCC is uncommon. There is no correlation, except in so-called hereditary conditions, such as Lynch syndrome, although none of our patients met the criteria.
In our series, both the ipsilateral and contralateral approaches were used. The latter posed greater technical difficulties, including the change in the position of the trocars and the patient. One patient was diagnosed with colon cancer and double kidney cancer, which has not been previously reported in the literature.2,4–7 In this case, partial left nephrectomy was performed by retroperitoneoscopy, with the intention of leaving the peritoneal cavity untouched for the following intervention. This approach was not recommended in the right tumor due to its large size, which made it technically more complex (especially because renorrhaphy using a retroperitoneal approach is more complicated due to the lack of space and triangulation). Few days later, laparoscopic subtotal colectomy was performed in supine decubitus, and subsequently the position was changed to left lateral decubitus for right partial nephrectomy. In spite of the tumor size and due to the surgical history in the contralateral kidney, nephron-sparing surgery was considered to preserve renal function (Fig. 1).

Most of our patients presented a postoperative period without complications, except for the last patient who presented intraabdominal abscesses, which made us suspect possible anastomotic dehiscence. The patient was treated conservatively and had a favorable recovery.
One of the advantages of the procedure is being able to treat 2 neoplasms at the same time. In this manner, treatment of the second neoplasm would not be delayed if postoperative complications were to appear after the first surgery. Furthermore, simultaneous treatment avoids a second anesthetic procedure and reduces discomfort for both patients and family members. And, as a second hospitalization is avoided, it is also a more cost-effective option.
Nonetheless, combined surgery in 2 different organs poses tactical difficulties. A synchronous approach is a greater biological aggression than performing two separate interventions, and hospitalization is lengthened. It is possible though, especially when both procedures are simple, as documented in other series,8–10 or when done at a high-level hospital centers with resources for satisfactory management.
Thus, simultaneous laparoscopic treatment of renal and colon cancer is feasible and reproducible. The greatest advantage of this technical option is that it allows for both lesions to be treated at the same time, thereby eliminating the delay of treating the lesions in sequential surgeries.
Please cite this article as: Martin Arnau AB, Ochoa Vargas C, Peña Gonzalez JA, Targarona Soler EM. Colectomía y nefrectomía simultánea en tumores sincrónicos. Cir Esp. 2015;93:266–268.
