






To evaluate the utility of the ROLL (Radioguided Occult Lesion Localization) technique as a method of excisional biopsy in hypermetabolic lesions suspected of malignancy evidenced in [18F]Fluordeoxiglucose PET/CT scans.
Material and methods33 patients were retrospectively evaluated referred for metabolic studies due to tumoral pathology or suspected neoplastic process and presenting hypermetabolic adenopathies with high probability of malignancy. The group consisted of 19 women and 14 men, ranging from 23 to 77 years old. Patients were performed a ROLL technique for localization and removal the selected adenopathies, through the injection of [99mTc] macro-aggregates of albumin guided by ultrasound or CT. A detection probe and a portable gamma camera were used during the surgical procedure.
ResultsIn 31 patients (94%) the location and removal of the radiolabeled adenopathies was achieved. In one patient the location of the lesion was not possible and a second patient was not operated due to inadequate dose injection confirmed by gammagraphy study. The result of the anatomopathological study of adenopathies resulted in 23 tumor affections and 8 benign processes, including a granulomatous process.
ConclusionThe ROLL technique proved its utility as a radioguided excisional biopsy method for the study of lesions suspected of malignancy evidenced in patients undergoing PET/CT studies. The technique allowed to confirm the persistence of oncological process in some cases and the existence of false positives from the imaging study in others, modifying the patients therapeutic management.
Valorar la utilidad de la técnica ROLL (Radioguided Occult Lesion Localization) como método de biopsia excisional en lesiones hipermetabólicas sospechosas de malignidad evidenciadas en exploraciones [18F]Fluordesoxiglucosa PET/TC.
Material y métodosSe valoraron retrospectivamente 33 pacientes remitidos para la realización de un estudio metabólico por patología tumoral conocida o por sospecha de proceso neoplásico y que presentaban adenopatías hipermetabólicas con alta probabilidad de malignidad. El grupo estaba constituido por 19 mujeres y 14 hombres, con rango de 23 a 77 años. Los pacientes fueron sometidos a la técnica ROLL para la localización y extirpación de las adenopatías seleccionadas, mediante inyección de [99mTc] macroagregados de albúmina guiada con ecográfica o TC. Durante el acto quirúrgico se utilizaron una sonda de detección y una gammacámara portátil.
ResultadosEn 31 pacientes (94%) se consiguió la localización y extirpación de las adenopatías radiomarcadas. En un paciente no fue posible la localización de la lesión y un segundo paciente no fue operado al confirmarse en estudio gammagráfico previo la inyección inadecuada de la dosis. El resultado del estudio anatomopatológico de las adenopatías dio como resultado 23 afectaciones tumorales y 8 procesos benignos, incluyendo un proceso granulomatoso.
ConclusiónLa técnica ROLL demostró su utilidad como método de biopsia excisional radiodirigida para el estudio de lesiones sospechosas de malignidad evidenciadas en pacientes sometidos a estudios PET/TC. La técnica permitió confirmar la persistencia de proceso oncológico en unos casos y la existencia de falsos positivos del estudio de imagen en otros, modificando el manejo terapéutico de los pacientes.
In recent years, the use of radioguided surgery (a nuclear medicine application) has grown more than other techniques, with the exception of positron emission tomography (PET).1 The term ‘radioguided surgery’ refers to a group of techniques aimed at optimizing minimally invasive tumor surgery. Recently, these techniques have been included as part of the GOSTT (Guided intraOperative Scintigraphic Tumor Targeting) techniques.2
PET/CT currently plays an important role in the management of cancer patients, and [18F]Fluorodeoxyglucose (FDG) is used as a metabolic radiopharmaceutical in most cases. In addition to the staging of processes and the assessment of the response to treatment, this technique is also indicated to guide biopsies in the event of suspected neoplastic pathology.3 Although the metabolic study is highly accurate, there are false positives due to inflammatory-infectious or reactive processes; therefore, depending on the circumstances, histological confirmation of the findings is necessary.4
Fine needle aspiration (FNA) or core needle biopsy (CNB) are used to evaluate suspicious lesions. However, the histological study may be compromised by insufficient material obtained or by the presence of numerous reactive cells and few tumor cells in the lesion, so excisional biopsy is proposed as the first option.5,6 But, if the hypermetabolic lesions found on PET/CT are not palpable, they can be difficult to find intraoperatively.
In this context, the ROLL (Radioguided Occult Lesion Localization) technique can play an important role, allowing us to confirm the findings seen in the metabolic study. Originally described for hidden breast lesions and included within the GOSTT, it is a type of radioguided surgery based on the injection of radioactive particles that are retained at the injection site.7
The aim of our study was to assess the usefulness of this technique as a radioguided excisional biopsy method in hypermetabolic lesions suspected of malignancy detected in patients undergoing PET/CT scans. The study was based on previous research by our group that included a limited number of patients.8
MethodsStudy patientsThis study is a retrospective assessment of 33 patients referred to our department for PET/CT study due to tumor pathology or suspected neoplastic process. All patients who presented hypermetabolic lymphadenopathies with a high probability of malignancy were evaluated retrospectively. The study period covered 6.5 years, from January 2012 to July 2019.
The group consisted of 19 women and 14 men, with a mean age of 54 (range 23−77 years). The indications for performing the metabolic test were: suspected tumor recurrence (20 patients); staging and/or biopsy guidance (8 patients); and assessment of response to treatment (5 patients).
PET/CT studyAll patients were administered an intravenous dose of 5MBq per kg of weight of [18F]FDG, 60min before the PET/CT study. The studies were acquired in a hybrid Discovery ST system (General Electric Medical Systems, Milwaukee, USA) with standard acquisition parameters. First, a full-body CT study was acquired with a voltage of 110 KeV and an amperage modulation with a maximum of 80mA. The PET study was performed by acquiring 20-cm-long 3D images with a 3-min duration in each sequence and subsequent iterative reconstruction.
In all patients, we observed one or more lymphadenopathies with elevated glycidic activity, and excisional biopsy was proposed for the nodes with better surgical access and greater metabolic activity (Fig. 1). The performance of FNAB or CNB prior to surgery was not considered for any patient.
 Patient with a history of ocular melanoma and suspected tumor recurrence. A hypermetabolic lymphadenopathy is observed in the right obturator chain, with a histology result after the ROLL technique of reactive follicular hyperplasia (1). A later PET study was negative (2). B) Patient with palpable lymphadenopathies and constitutional syndrome. In the metabolic study ordered for staging and to guide biopsy, several hypermetabolic lymphadenopathies were observed above and below the diaphragm (3). The histology result after ROLL of a right lateral cervical lymphadenopathy was large-cell lymphoma B. After chemotherapy, a second PET confirmed complete response (4).")
Coronal slices of PET and fusion image: A) Patient with a history of ocular melanoma and suspected tumor recurrence. A hypermetabolic lymphadenopathy is observed in the right obturator chain, with a histology result after the ROLL technique of reactive follicular hyperplasia (1). A later PET study was negative (2). B) Patient with palpable lymphadenopathies and constitutional syndrome. In the metabolic study ordered for staging and to guide biopsy, several hypermetabolic lymphadenopathies were observed above and below the diaphragm (3). The histology result after ROLL of a right lateral cervical lymphadenopathy was large-cell lymphoma B. After chemotherapy, a second PET confirmed complete response (4).
After signing an informed consent form, the patients underwent the ROLL technique for localization and removal of the selected lymphadenopathies, performed 1–12 weeks after the PET/CT study. The protocol involved the injection in the center of the lesion under ultrasound guidance (28 cases) or CT guidance (5 cases) of a dose of 37MBq of [99mTc] macroaggregated albumin (MAA) in a volume of 0.1mL the day before surgery. Planar scintigraphy confirmed the focal deposition of the radiopharmaceutical and the absence of skin contamination immediately after the administration of the radiopharmaceutical. Likewise, in some patients a multimodality SPECT/CT study was acquired to locate the lesion anatomically.
The ROLL technique was performed under general anesthesia and using minimally invasive surgery. A Europrobe® detection probe and a Minicam® portable gamma camera were used during the surgical procedure, both with a cadmium telluride detector. The most frequent locations of the lymphadenopathies resected were in the axillae, lateral cervical spaces, external or inguinal iliac chains, and supraclavicular spaces. After verifying the absence of residual activity in the surgical field, they were referred for a delayed histological and immunohistochemical study.
Statistical analysisThe data were analyzed with the SPSS® statistical program (IBM, New York, USA), version 5.0.1.
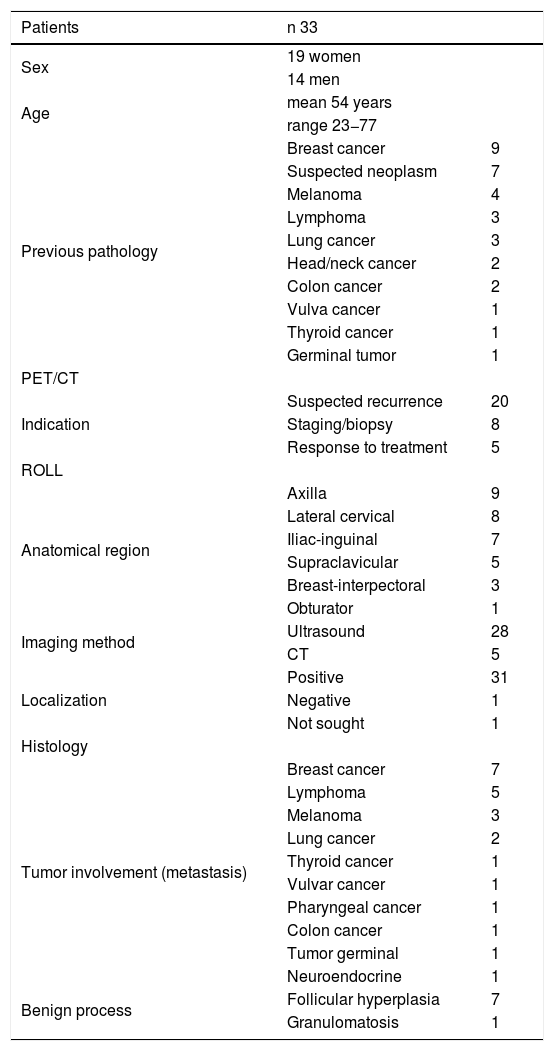
ResultsTable 1 lists the clinical characteristics, diagnoses, PET/CT findings and surgery, as well as the evolution of the patients under study. In 31 patients (94%), the radiolabeled lymphadenopathies were located and removed. In one patient, it was not possible to locate the radioactive dose (in the left lateral cervical location), while a second patient excision was not done because the SPECT/CT showed that the radiopharmaceutical was injected in an inappropriate location.
Clinical characteristics, PET/CT findings, surgery and evolution of study patients.
| Patients | n 33 | |
|---|---|---|
| Sex | 19 women | |
| 14 men | ||
| Age | mean 54 years | |
| range 23−77 | ||
| Previous pathology | Breast cancer | 9 |
| Suspected neoplasm | 7 | |
| Melanoma | 4 | |
| Lymphoma | 3 | |
| Lung cancer | 3 | |
| Head/neck cancer | 2 | |
| Colon cancer | 2 | |
| Vulva cancer | 1 | |
| Thyroid cancer | 1 | |
| Germinal tumor | 1 | |
| PET/CT | ||
| Indication | Suspected recurrence | 20 |
| Staging/biopsy | 8 | |
| Response to treatment | 5 | |
| ROLL | ||
| Anatomical region | Axilla | 9 |
| Lateral cervical | 8 | |
| Iliac-inguinal | 7 | |
| Supraclavicular | 5 | |
| Breast-interpectoral | 3 | |
| Obturator | 1 | |
| Imaging method | Ultrasound | 28 |
| CT | 5 | |
| Localization | Positive | 31 |
| Negative | 1 | |
| Not sought | 1 | |
| Histology | ||
| Tumor involvement (metastasis) | Breast cancer | 7 |
| Lymphoma | 5 | |
| Melanoma | 3 | |
| Lung cancer | 2 | |
| Thyroid cancer | 1 | |
| Vulvar cancer | 1 | |
| Pharyngeal cancer | 1 | |
| Colon cancer | 1 | |
| Tumor germinal | 1 | |
| Neuroendocrine | 1 | |
| Benign process | Follicular hyperplasia | 7 |
| Granulomatosis | 1 | |
| Follow-up | |
| Tumor involvement | |
| PET with response to treatment | 12 |
| PET with disease persistence | 6 |
| CT with response to treatment | 3 |
| CT with disease persistence | 1 |
| Exitus | 1 |
| Benign process | |
| PET without findings | 5 |
| Clinical follow-up | 2 |
| CT without findings | 1 |
The mean operative time was 34min (range 23−52min). Postoperative complications were rare, with one patient presenting a keloid, another a local infection of a suture, and a third a fistulous path to the skin.
The results of the pathological study of the lymphadenopathies reported 23 with tumor involvement and eight benign processes, including one granulomatous process. In this manner, the technique made it possible to confirm the existence of false positives in the PET/CT study of these latter patients. Likewise, the results obtained indicated the administration of chemo or radiotherapy to 19 patients and surgical treatment in another two.
Patient evolution was assessed by clinical examination, analytical and radiological studies and/or a new PET/CT scan. The minimum evolution time for this evaluation was six months. None of the patients with benign process histology in the lesion showed symptoms of recurrence or tumor process, and the follow-up PET/CT study did not show pathological findings in 5 patients. Finally, the patient diagnosed with granulomatous disease showed an adequate response to treatment with corticosteroids.
DiscussionRadioguided surgery includes sentinel lymph node detection techniques and the ROLL technique, all of this within the GOSTT concept. Since the first publication carried out by Cabañas in 1977 to the present, the detection of the sentinel node has become widespread, and its indication is being accepted in breast, head and neck tumors, melanoma or gynecological neoplasms.1,9
The ROLL technique allows for lesions marked with radioactive isotopes to be identified intraoperatively when they otherwise would be difficult to locate due to their size or anatomical situation. The method is based on the intralesional injection of a radiopharmaceutical that, due to its size, remains at the site of administration. The surgeon verifies complete removal of the lymphadenopathy by confirming absence of tracer activity in the surgical site after the excisional biopsy using the detection probe.2
The technique began to be used in occult breast cancer, and there are numerous publications that confirm its advantages, including easier excision and more comfort for the patient compared to metal guidewires.10,11 Currently, it is also applied in thyroid cancer that presents non-palpable cervical lymphadenopathies, pulmonary nodules or in colonic lesions.12,13
The PET/CT study is considered one of the most useful imaging tests for the diagnosis and follow-up of cancer patients, providing staging of the process or its use to guide biopsy. The most representative and accessible hypermetabolic lesions are easily identified for histological study.14
Although there are numerous radiopharmaceuticals, the most widely used in clinical practice is [18F]FDG, whose uptake is based on the elevated glycidic metabolism that the tumor cell presents. However, inflammatory, infectious or granulomatous processes can be the cause of false positives as the tracer also accumulates. PET studies in lymphomas acquired after two cycles of chemotherapy present false positives in up to 30% due to these etiologies, which may lead to unnecessary examinations or treatments.15 Thus, several authors have applied the ROLL technique as an excisional biopsy method or as a rescue surgery technique after PET/CT study, showing good results.6,13,16,17
Our results concur with these studies. Radioguided surgery confirmed the persistence of neoplastic activity in 23 patients, which resulted in modifications to their therapeutic management. Likewise, it revealed eight false positives from the metabolic study, thereby avoiding the need for additional complementary tests and the administration of unnecessary treatments.
There are other non-isotopic techniques for marking non-palpable lesions, including the insertion of metallic materials or the use of other substances. The guidewire technique uses flexible needles that are anchored in the lesion. To minimize the possibility of mobilization, placement must be performed the same day as surgery. There is a risk of puncture during the procedure and in the histological study; remains of the material may stay in the tissue, causing infection or bleeding. Likewise, its use determines the surgical route and, with it, the aesthetic result of the procedure.18
The use of lipiodol, a type of radiopaque contrast, has the disadvantage of being able to diffuse outside the lesion and generate unwanted reactions in the body.19 Lastly, a suspension of activated carbon has been used as a marking substance. Among its drawbacks are the appearance of skin tattoos, possible granulomatous reactions and histological samples altered by the substance itself.20
The ROLL technique was precise, simple and easy to apply. The use of ultrasound to guide the administration of the radiopharmaceutical has proven to be a simple, inexpensive and effective method. The acquisition of a scintigraphy image prior to surgery made it possible to verify the quality of the injection and the absence of skin contamination. The PET/CT images were used as an anatomical guide for the surgery, and the use of [99mTc]MAA made it possible to perform surgery the day after injection. The high signal in the marked lesion, with no background activity, facilitated both the location of the radiopharmaceutical and the confirmation of its complete removal, thereby achieving short surgical times and few postoperative complications.
The ROLL technique has some limitations that must be considered. Its accuracy depends on adequate puncture of the lesion and surgical accessibility.21 In our study, one patient was not operated on because the radiopharmaceutical was not found in the correct location. In a second patient, the lymph node under study was not located during surgery, which was attributed to an inadequate puncture. These cases represented 6% of patients, which is a lower value compared to the results from using ROLL in breast pathology.22
In patients with multiple lesions suspicious of malignancy observed on PET/CT, it is impossible to perform an excisional biopsy of all of them. Likewise, the lack of accessibility of a lymphadenopathy for injection requires considering other possibilities. In these cases, different authors have used [18F]FDG as a tracer, obviating the need for puncture of the lesions, since this radiopharmaceutical accumulates in the tumor tissue after intravenous injection.16,17 The use of a positron-emitting isotope with a limited half-life, like [18F], significantly reduces the time window for surgery.17 On the other hand, it is necessary to use a high-energy surgical probe, consider the presence of significant background activity and the problems derived from the radioprotection of healthcare personnel. In this context, the use of [99mTc]MAA minimizes the radiation exposure of patients, surgeons and pathologists, as it is well below the limits recommended by the International Commission on Radiological Protection.23
In our case, some patients had numerous hypermetabolic lymphadenopathies in the imaging study. Despite this, the lymphadenopathy selected in each patient for puncture and subsequent excision proved to be adequate, as confirmed by both the clinical evolution and subsequent metabolic studies.
In conclusion, the ROLL technique has been shown to be useful as a radioguided excisional biopsy method for the study of patients with lesions suspicious for malignancy on PET/CT studies. The technique made it possible to confirm the persistence of the oncological process in some cases and the existence of false positives in the imaging study in others, which led to modifications in the therapeutic management of these patients.
Conflicts of interestThe authors have no conflict of interests to declare.
Please cite this article as: Infante JR, Rayo JI, Serrano J, Jiménez JL, Moreno M, Martínez A, et al. Aplicación de la técnica ROLL como método de biopsia excisional en patología oncológica. Cir Esp. 2021;99:49–54.
