




The aim is comparing the quality of care at a typical American trauma center (USC) vs an equivalent European referral center in Spain (SRC), through the analysis of preventable and potentially preventable deaths.
MethodsComparative study that evaluated trauma patients older than 16 years old who died during their hospitalization. We cross-referenced these deaths and extracted all deaths that were classified as potentially preventable or preventable. All errors identified were then classified using the JC taxonomy.
ResultsThe rate of preventable and potentially preventable mortality was 7.7% and 13.8% in the USC and SRC respectively.
According to the JC taxonomy, the main error type was clinical in both centers, due to errors in intervention (treatment). Errors occurred mostly in the emergency department and were caused by physicians. In the USC, 73% of errors were therapeutic as compared to 59% in the SRC (P=.06). The SRC had a 41% of diagnosis errors vs just 18% in the USC (P=.001). In both centers, the main cause of error was human. At the USC, the most frequent human cause was ‘knowledge-based’ (44%). In contrast, at the SRC center the most common errors were ‘rule-based’ (58%) (P<.001).
ConclusionsThe use of a common language of errors among centers is key in establishing benchmarking standards. Comparing the quality of care of an American trauma center and a Spanish referral center, we have detected remarkably similar avoidable errors. More diagnostic and ‘ruled-based’ errors have been found in the Spanish center.
El objetivo del estudio es comparar la calidad asistencial de un trauma center americano (USC) vs un centro equivalente de referencia europeo (SRC) en España, a través del análisis de la mortalidad evitable.
MétodosEstudio comparativo que evalúa pacientes politraumatizados mayores de 16 años que han sido exitus durante su hospitalización. Se han identificado las muertes evitables o potencialmente evitables, analizando los errores en el manejo, clasificándolos según la taxonomía de la Joint Comission.
ResultadosLa incidencia de mortalidad evitable y potencialmente evitable fue del 7,7% en el USC, y del 13,8% en el SRC.
Según la taxonomía de la Joint Comission, el principal tipo de error fue clínico en ambos centros, debido a errores de intervención (tratamiento). Los errores ocurren en urgencias y fueron causados por médicos. En el USC, el 73% de los errores fue de tipo terapéutico comparado con el 59% en el SRC (p=0,06). El SRC tuvo un 41% de errores diagnósticos vs solo el 18% en el USC (p=0,001). En ambos centros, el principal tipo de error fue humano, siendo tipo knowledge-based el más frecuente en el USC (44%) vs rule-based en el SRC (58%) (p<0,001).
ConclusionesEl uso de un lenguaje común para analizar los errores de manejo es una clave esencial para establecer puntos de referencia estándares y universales. Comparando la calidad asistencial de un trauma center americano con la de un centro de referencia español, hemos detectado unos errores evitables extraordinariamente parecidos. Se han hallado más errores diagnósticos y de tipo ruled-based en el centro español.
Polytrauma continues to be one of the leading causes of death in people under the age of 40.1 Analyzing the quality of the treatment of polytrauma patients is essential in order to improve morbidity and mortality results, but it is not easy to establish quality standards. Evaluations of the quality of management of polytrauma patients reveal that it is frequently below recognized standards.2,3 An excellent way to determine quality is by analyzing preventable or potentially preventable deaths.
The definition of each type of mortality (preventable, potentially preventable, and inevitable) is controversial. According to a systematic review published by Costanti et al.,4 89.7% of publications define the 3 types of mortality according to the analysis of errors produced in the management of polytrauma patients based on clinical guidelines such as ATLS®,5 62.1% define them according to severity criteria like the Injury Severity Score (ISS),6 55.2% according to the probability of survival determined by the Trauma-Injury Severity Score (TRISS),7 and 3.4% by a combination of elements such as patient comorbidity, initial physiological conditions, anatomical injuries, etc. Following the classification of mortality according to the analysis of errors, preventable mortality is caused directly by an avoidable error, potentially preventable mortality could have been caused by an avoidable error, and inevitable mortality would have occurred regardless of the appearance of treatment errors in these patients.8–14
Most authors analyze errors that have caused avoidable or potentially avoidable deaths, using a classification of these errors.15–25 Although the analysis of errors is an essential mechanism to identify areas for improvement, the use of a non-standardized classification is a serious problem for the comparison of results among hospitals. The use of well-standardized terminology, such as that of the Joint Commission on Accreditation of Healthcare Organizations (JCAHO),26 widely applied in other clinical fields of medicine, allows errors to be recorded, analyzed and corrected. Only Ivatury et al. and Montmany et al.8,9 apply the taxonomy of JCAHO in the analysis of errors that cause preventable and potentially preventable mortality in polytrauma patients. The main limitation of the use of the JCAHO taxonomy is the use of unfamiliar and complex language until one becomes familiarized with it.
The aim of this study is to compare the mortality analysis from an American trauma center8 and one from a Spanish referral hospital.9 Errors were classified by the same person at both hospitals, thereby ensuring that the same language was used within the JCAHO taxonomy.
MethodsThis is a comparative, retrospective and descriptive study including patients who were prospectively registered in a protected database at a US trauma center between 2002 and 20108 and a Spanish referral hospital from 2006 to 2016.9
The trauma center records data from all patients over the age of 16 treated under the polytrauma code, while the Spanish referral hospital registers all patients over the age of 16 treated and admitted to the critical care unit.
The study analyzes only the patients registered in the database who were deceased, excluding those under the age of 16 (treated by pediatric medical teams at both centers) and those who had died before arrival at the hospital (due to lack of data that would impede the analysis of their quality of care).
The inclusion criteria for our study are polytrauma patients who were deceased and had been treated at the American trauma center or the critical care unit at the Spanish referral hospital. At both hospitals, we have included patients who died before being admitted to the corresponding hospitalization areas.
At both medical centers, the following variables were recorded for each case: age, sex, mechanism of action, ISS,6 revised trauma score (RTS),27 prehospital and hospital vital signs, complementary tests, diagnosis and treatment of each injury, complications, date and cause of death.
The Trauma Center at Penn is a level-1 trauma center located in downtown Philadelphia, associated with the Hospital of the University of Pennsylvania (HUP), a third-level university hospital. The Hospital Universitari Parc Taulí is located 25km from Barcelona, and is one of the referral hospitals for polytrauma patients in Catalonia, Spain. It is a third-level university hospital associated with the Autonomous University of Barcelona. Both centers have trauma care teams trained in accordance with ATLS®5 guidelines, as well as immediate availability of blood products, 128-slice computed tomography (CT) and arteriography available 24h a day. Both centers use the same criteria and protocols for diagnosis and treatment in the care of polytrauma patients.
Three types of mortality have been defined: preventable, potentially preventable and inevitable. Preventable mortality is that caused by an avoidable error; potentially preventable mortality is the result of avoidable errors, but clear causality cannot be confirmed; and inevitable mortality is not caused by any errors, whether or not they occur in the management of the patient.
The avoidable errors are established according to different criteria: probability of survival, hemodynamic stability of patients upon arrival to the emergency room and, above all, the errors produced by not following the guidelines established in the clinical protocol of the ATLS®.5
In multidisciplinary sessions, all cases of mortality were analyzed, detecting avoidable errors and determining whether the error was the cause of death or not, thereby classifying each case as preventable, potentially preventable or unavoidable death.
Each of these errors was analyzed and classified according to the taxonomy of JCAHO26 at each center and by the same person.
Statistical AnalysisThe collected data have been registered in an Access® database in protected format. The descriptive analysis is presented as mean and standard deviation for continuous variables and as percentages for categorical variables. The Student's t and Chi squared test were used to compare groups after confirming the normality of the variables and the homoscedasticity of the variance. SPSS IBM 21.0® was used for the different statistical calculations. A P value <.05 was considered statistically significant.
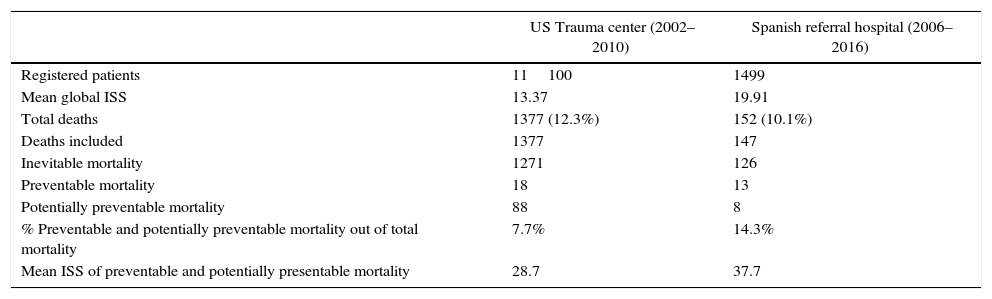
ResultsOver the course of a 9-year period, 11100 polytrauma patients were registered in the US trauma center, with a mean ISS of 13.37 and a mortality rate of 12.4%. The Spanish referral hospital registered 1499 patients, with a mean ISS of 19.91 and a mortality rate of 10.1%. For the current study, 4 patients were excluded as they had been transferred from another hospital to receive specific treatment and then returned to the original hospital post-procedure. In addition, we also excluded a cirrhotic patient transferred from another hospital one month after admission for melena, who died of encephalopathy.
The population studied is comprised of 1377 deceased patients who had been treated at the American trauma center and 147 deceased patients at the Spanish referral hospital.
The trauma center presented a 0.95% rate of avoidable or potentially avoidable mortality of the total number of registered patients, and 7.7% of the total of patients who had died. The mean ISS of the group of patients with preventable and potentially preventable mortality was 28.7. The Spanish referral hospital had a 1.4% rate of avoidable or potentially avoidable mortality out of the total number of patients registered, and 14.3% of the total number of patients who had died, with a mean ISS of 37.7 (Table 1).
Mortality.
| US Trauma center (2002–2010) | Spanish referral hospital (2006–2016) | |
|---|---|---|
| Registered patients | 11100 | 1499 |
| Mean global ISS | 13.37 | 19.91 |
| Total deaths | 1377 (12.3%) | 152 (10.1%) |
| Deaths included | 1377 | 147 |
| Inevitable mortality | 1271 | 126 |
| Preventable mortality | 18 | 13 |
| Potentially preventable mortality | 88 | 8 |
| % Preventable and potentially preventable mortality out of total mortality | 7.7% | 14.3% |
| Mean ISS of preventable and potentially presentable mortality | 28.7 | 37.7 |
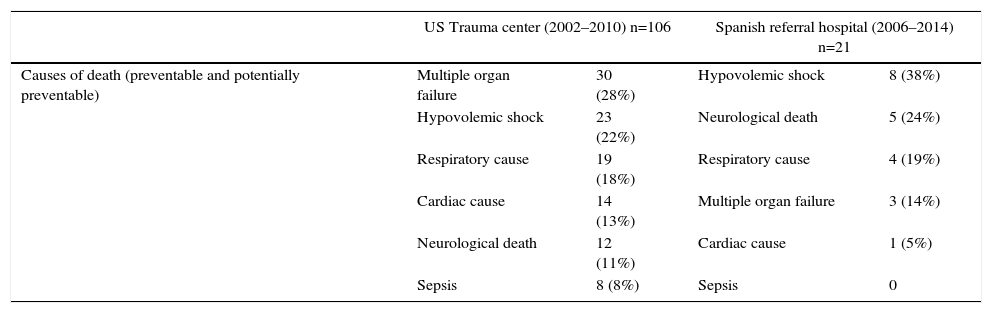
The main causes of death in preventable and potentially preventable death at the American trauma center were multiple organ failure (28%) and hypovolemic shock (21%). At the Spanish referral hospital, hypovolemic shock (38%) and neurological death (24%) were the main causes (Table 2).
Causes of Mortality.
| US Trauma center (2002–2010) n=106 | Spanish referral hospital (2006–2014) n=21 | |||
|---|---|---|---|---|
| Causes of death (preventable and potentially preventable) | Multiple organ failure | 30 (28%) | Hypovolemic shock | 8 (38%) |
| Hypovolemic shock | 23 (22%) | Neurological death | 5 (24%) | |
| Respiratory cause | 19 (18%) | Respiratory cause | 4 (19%) | |
| Cardiac cause | 14 (13%) | Multiple organ failure | 3 (14%) | |
| Neurological death | 12 (11%) | Cardiac cause | 1 (5%) | |
| Sepsis | 8 (8%) | Sepsis | 0 | |
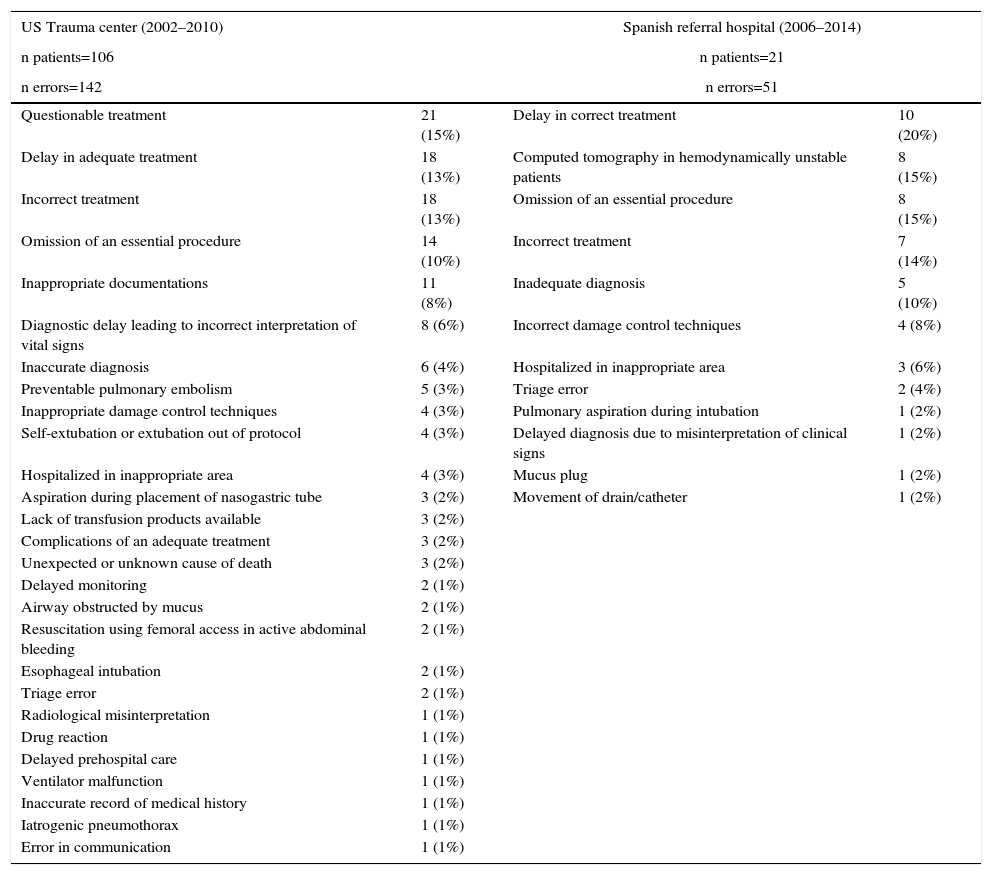
In patients with preventable or potentially preventable death, 142 avoidable errors were detected in the 106 patients from the trauma center and 51 avoidable errors in the 21 patients of the Spanish referral hospital. Therapeutic errors were the main types of errors at both centers. At the Spanish referral hospital, there was also a high percentage of errors due to incorrect diagnosis (10%) or due to performing computed tomography (CT) in hemodynamically unstable patients (15%), errors that practically did not occur at the trauma center (Table 3).
Description of Errors: Therapeutic Errors, Diagnostic Errors and Various Errors.
| US Trauma center (2002–2010) | Spanish referral hospital (2006–2014) | ||
|---|---|---|---|
| n patients=106 | n patients=21 | ||
| n errors=142 | n errors=51 | ||
| Questionable treatment | 21 (15%) | Delay in correct treatment | 10 (20%) |
| Delay in adequate treatment | 18 (13%) | Computed tomography in hemodynamically unstable patients | 8 (15%) |
| Incorrect treatment | 18 (13%) | Omission of an essential procedure | 8 (15%) |
| Omission of an essential procedure | 14 (10%) | Incorrect treatment | 7 (14%) |
| Inappropriate documentations | 11 (8%) | Inadequate diagnosis | 5 (10%) |
| Diagnostic delay leading to incorrect interpretation of vital signs | 8 (6%) | Incorrect damage control techniques | 4 (8%) |
| Inaccurate diagnosis | 6 (4%) | Hospitalized in inappropriate area | 3 (6%) |
| Preventable pulmonary embolism | 5 (3%) | Triage error | 2 (4%) |
| Inappropriate damage control techniques | 4 (3%) | Pulmonary aspiration during intubation | 1 (2%) |
| Self-extubation or extubation out of protocol | 4 (3%) | Delayed diagnosis due to misinterpretation of clinical signs | 1 (2%) |
| Hospitalized in inappropriate area | 4 (3%) | Mucus plug | 1 (2%) |
| Aspiration during placement of nasogastric tube | 3 (2%) | Movement of drain/catheter | 1 (2%) |
| Lack of transfusion products available | 3 (2%) | ||
| Complications of an adequate treatment | 3 (2%) | ||
| Unexpected or unknown cause of death | 3 (2%) | ||
| Delayed monitoring | 2 (1%) | ||
| Airway obstructed by mucus | 2 (1%) | ||
| Resuscitation using femoral access in active abdominal bleeding | 2 (1%) | ||
| Esophageal intubation | 2 (1%) | ||
| Triage error | 2 (1%) | ||
| Radiological misinterpretation | 1 (1%) | ||
| Drug reaction | 1 (1%) | ||
| Delayed prehospital care | 1 (1%) | ||
| Ventilator malfunction | 1 (1%) | ||
| Inaccurate record of medical history | 1 (1%) | ||
| Iatrogenic pneumothorax | 1 (1%) | ||
| Error in communication | 1 (1%) | ||
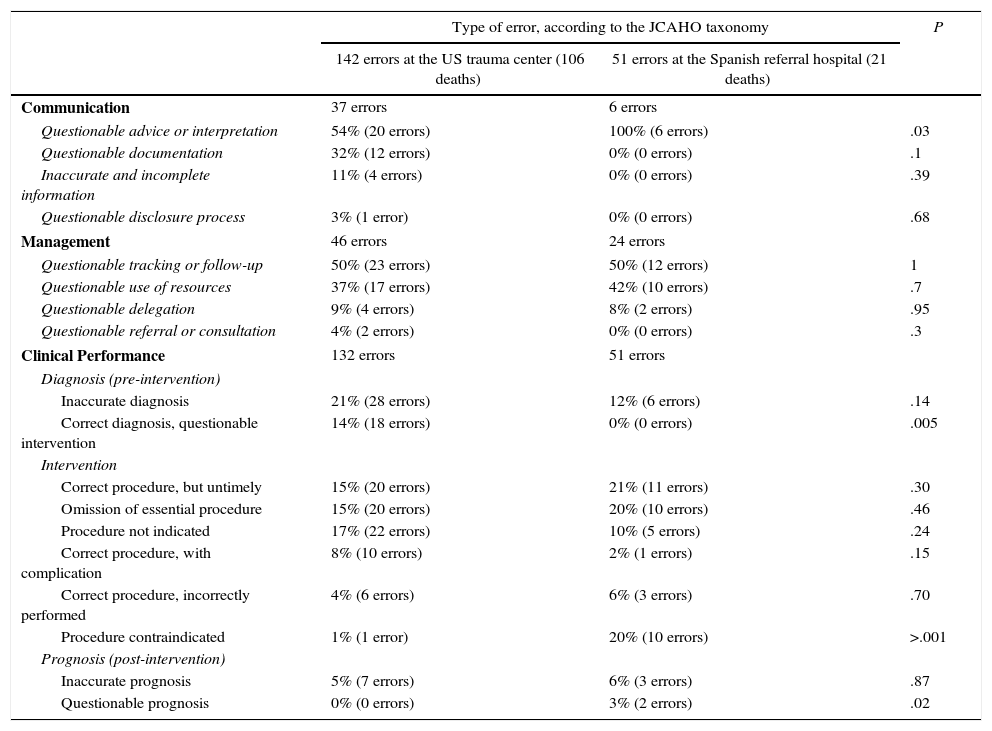
Upon analyzing the errors of the preventable and potentially preventable deaths according to the JCAHO taxonomy, we found that the error types are remarkably similar in both centers (Table 4). The errors were mainly caused by questionable clinical interpretations (questionable advice or interpretation, questionable tracking or follow-up and inaccurate diagnosis) and intervention errors (correct procedure but untimely, omission of essential procedure, and procedure not indicated). The main statistically significant difference is that at the Spanish referral hospital there was a considerable percentage of contraindicated procedures that did not appear at the trauma center, where there was a higher percentage of procedures without indications (Table 4).
Type of Error in Preventable and Potentially Preventable Death.
| Type of error, according to the JCAHO taxonomy | P | ||
|---|---|---|---|
| 142 errors at the US trauma center (106 deaths) | 51 errors at the Spanish referral hospital (21 deaths) | ||
| Communication | 37 errors | 6 errors | |
| Questionable advice or interpretation | 54% (20 errors) | 100% (6 errors) | .03 |
| Questionable documentation | 32% (12 errors) | 0% (0 errors) | .1 |
| Inaccurate and incomplete information | 11% (4 errors) | 0% (0 errors) | .39 |
| Questionable disclosure process | 3% (1 error) | 0% (0 errors) | .68 |
| Management | 46 errors | 24 errors | |
| Questionable tracking or follow-up | 50% (23 errors) | 50% (12 errors) | 1 |
| Questionable use of resources | 37% (17 errors) | 42% (10 errors) | .7 |
| Questionable delegation | 9% (4 errors) | 8% (2 errors) | .95 |
| Questionable referral or consultation | 4% (2 errors) | 0% (0 errors) | .3 |
| Clinical Performance | 132 errors | 51 errors | |
| Diagnosis (pre-intervention) | |||
| Inaccurate diagnosis | 21% (28 errors) | 12% (6 errors) | .14 |
| Correct diagnosis, questionable intervention | 14% (18 errors) | 0% (0 errors) | .005 |
| Intervention | |||
| Correct procedure, but untimely | 15% (20 errors) | 21% (11 errors) | .30 |
| Omission of essential procedure | 15% (20 errors) | 20% (10 errors) | .46 |
| Procedure not indicated | 17% (22 errors) | 10% (5 errors) | .24 |
| Correct procedure, with complication | 8% (10 errors) | 2% (1 errors) | .15 |
| Correct procedure, incorrectly performed | 4% (6 errors) | 6% (3 errors) | .70 |
| Procedure contraindicated | 1% (1 error) | 20% (10 errors) | >.001 |
| Prognosis (post-intervention) | |||
| Inaccurate prognosis | 5% (7 errors) | 6% (3 errors) | .87 |
| Questionable prognosis | 0% (0 errors) | 3% (2 errors) | .02 |
JCAHO: Joint Commission on Accreditation of Healthcare Organizations.26
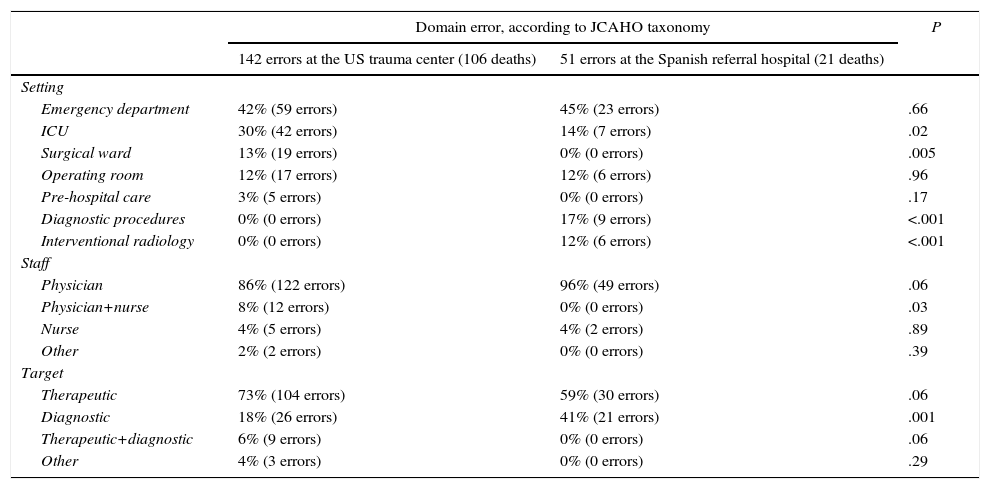
At both hospitals, the main errors were committed in the emergency department (42% and 45%), caused by the medical specialist (86% and 96%), and they were mostly therapeutic at both medical centers (73% and 59%). Although at the Spanish referral hospital (similar to the American trauma center) therapeutic errors were more frequent, incorrect diagnosis also occurred at an important rate (41% of errors), compared to only 18% of the errors at the US trauma center, which was a statistically significant difference (P=.001) (Table 5).
Domain Error in Preventable and Potentially Preventable Death.
| Domain error, according to JCAHO taxonomy | P | ||
|---|---|---|---|
| 142 errors at the US trauma center (106 deaths) | 51 errors at the Spanish referral hospital (21 deaths) | ||
| Setting | |||
| Emergency department | 42% (59 errors) | 45% (23 errors) | .66 |
| ICU | 30% (42 errors) | 14% (7 errors) | .02 |
| Surgical ward | 13% (19 errors) | 0% (0 errors) | .005 |
| Operating room | 12% (17 errors) | 12% (6 errors) | .96 |
| Pre-hospital care | 3% (5 errors) | 0% (0 errors) | .17 |
| Diagnostic procedures | 0% (0 errors) | 17% (9 errors) | <.001 |
| Interventional radiology | 0% (0 errors) | 12% (6 errors) | <.001 |
| Staff | |||
| Physician | 86% (122 errors) | 96% (49 errors) | .06 |
| Physician+nurse | 8% (12 errors) | 0% (0 errors) | .03 |
| Nurse | 4% (5 errors) | 4% (2 errors) | .89 |
| Other | 2% (2 errors) | 0% (0 errors) | .39 |
| Target | |||
| Therapeutic | 73% (104 errors) | 59% (30 errors) | .06 |
| Diagnostic | 18% (26 errors) | 41% (21 errors) | .001 |
| Therapeutic+diagnostic | 6% (9 errors) | 0% (0 errors) | .06 |
| Other | 4% (3 errors) | 0% (0 errors) | .29 |
JCAHO: Joint Commission on Accreditation of Healthcare Organizations.26
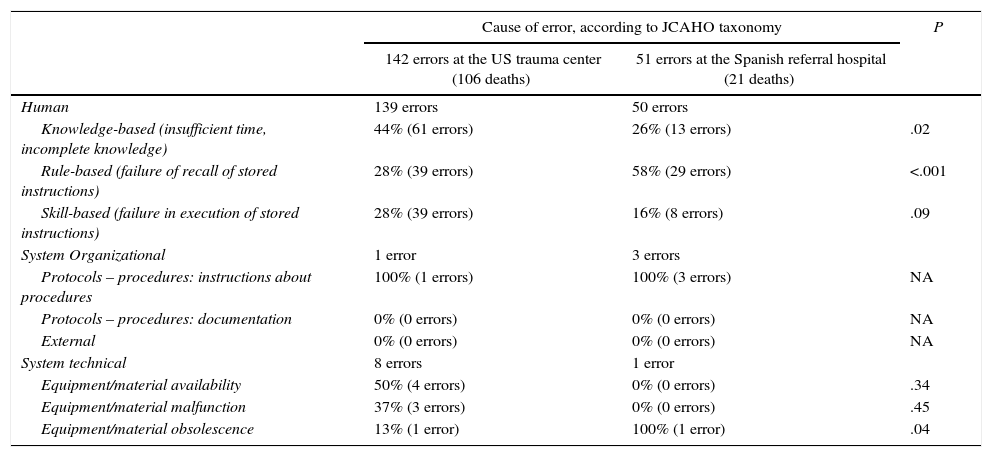
At both hospitals, the most frequent error was categorized as “human cause”. At the trauma center, the most frequent human errors were knowledge-based, meaning errors related with incorrect timing or incomplete knowledge (44% of errors). Meanwhile, at the Spanish referral hospital, the errors were rule-based, meaning that they were related with not following established established protocols (58% of errors) (Table 6).
Cause of Error in Preventable and Potentially Preventable Death.
| Cause of error, according to JCAHO taxonomy | P | ||
|---|---|---|---|
| 142 errors at the US trauma center (106 deaths) | 51 errors at the Spanish referral hospital (21 deaths) | ||
| Human | 139 errors | 50 errors | |
| Knowledge-based (insufficient time, incomplete knowledge) | 44% (61 errors) | 26% (13 errors) | .02 |
| Rule-based (failure of recall of stored instructions) | 28% (39 errors) | 58% (29 errors) | <.001 |
| Skill-based (failure in execution of stored instructions) | 28% (39 errors) | 16% (8 errors) | .09 |
| System Organizational | 1 error | 3 errors | |
| Protocols – procedures: instructions about procedures | 100% (1 errors) | 100% (3 errors) | NA |
| Protocols – procedures: documentation | 0% (0 errors) | 0% (0 errors) | NA |
| External | 0% (0 errors) | 0% (0 errors) | NA |
| System technical | 8 errors | 1 error | |
| Equipment/material availability | 50% (4 errors) | 0% (0 errors) | .34 |
| Equipment/material malfunction | 37% (3 errors) | 0% (0 errors) | .45 |
| Equipment/material obsolescence | 13% (1 error) | 100% (1 error) | .04 |
JCAHO: Joint Commission on Accreditation of Healthcare Organizations26; NA: not applicable.
Analyzing the quality of care received by polytrauma patients is fundamental to improve their management and consequently their morbidity and mortality rates. It is essential to use a common language for this quality analysis in order to establish standard and universal parameters. Our study aims to compare the mortality analysis performed at an American trauma center8 with an analysis from a Spanish referral hospital,9 using a common language established by the JCAHO taxonomy.26
The initial registry of the patients is different at both centers: the American trauma center registers absolutely all polytrauma patients (11100 patients, with a mean ISS of 13.37), while the Spanish referral hospital registers polytrauma patients in the critical care unit (1499 patients, with a mean ISS of 19.91). Despite this difference, the group of patients that was compared (patients with avoidable and potentially avoidable mortality) is a group of severe patients at both centers, with a mean ISS greater than 25 (28.7 at the US trauma center and 37.7 at the Spanish referral hospital).
Despite the large difference in the number of patients treated per center, the similarity of the results and overall mortality over a similar time period is striking.
The overall mortality of both medical centers (12.4% at the trauma center and 10.1% at the Spanish referral hospital) is within accepted parameters for normality (9% in patients with a mean ISS of 12.8; <10% in patients with ISS ≤15, or >20% in patients with ISS >25).
In our study, the prevalence of preventable and potentially preventable mortality was 7.7% at the trauma center and 14.3% at the Spanish referral hospital. The differences between the two medical centers are most probably due to the number of patients being treated and the experience of each center, although we must also take into account that, at the Spanish referral hospital, the patients were somewhat more severe than at the trauma center (mean ISS 37.7 vs 28.7). By analyzing the publications that define preventable and potentially preventable mortality with the same criteria that we used in our study, we observed that the prevalence of avoidable and potentially avoidable mortality of the total number of deaths ranged from 2.5% to 34%.8–11,18,21–24
Coinciding with Tien et al.28 and Ivatury et al.,10 the most frequent cause of preventable and potentially preventable death at the Spanish referral hospital was hypovolemic shock (38%), which was the second most frequent cause at the US trauma center (22%) (Table 2). To reduce errors in the initial management of hypovolemic shock, adequate training in protocols such as ATLS® is essential. Navarro et al.29 recorded a progressive reduction in avoidable mortality as the number of professionals trained in this protocol increased.
Using our own definition for errors in the management of polytrauma patients, the conclusions we have made may be limited and not at all comparable with other series (Table 3).
Following the JCAHO taxonomy,26 we found that the classification and distribution of errors at both medical centers were fairly homogeneous. There were small differences in the type of error: the Spanish referral hospital had more contraindicated procedures, such as transferring hemodynamically unstable patients for a CT scan, whereas the US trauma center had a high percentage of non-indicated procedures, like performing an unnecessary thoracotomy in a patient in hypovolemic shock of abdominal origin. The difference between contraindicated and non-indicated procedures can be very subtle, so they could be considered the same type of error. Most importantly, at both hospitals, errors are mostly caused by questionable clinical interpretations (questionable advice or interpretation, questionable tracking or follow-up and inaccurate diagnosis) and errors of intervention (correct procedure but untimely and omission of essential procedure).
At both medical centers, errors occurred mainly in the emergency room, performed by the medical specialist, and were therapeutic in nature. However, at the Spanish referral hospital, the percentage of diagnostic errors was 41%, while at the trauma center it was below 20%.
The main difference between the two hospitals was found by analyzing the cause of the error, and both centers coincided in human error as the main cause (Table 6). However, at the American trauma center the errors were mainly knowledge-based, meaning errors due to inappropriate timing or incomplete knowledge. For example, undetected lesions such as a liver injury with contrast extravasation that went unnoticed on the abdominal CT study.
At the Spanish referral hospital, coinciding with Ivatury et al.,10 the errors were mainly rule-based, meaning they occurred by not adhering to established protocols. For example, not activating the polytrauma patient care code when it should have been activated, or performing incorrect damage control techniques.
The predominance of rule-based errors at the Spanish referral hospital may be conditioned by the idiosyncrasy of the Spanish population to follow their instincts and improvise, rather than follow established norms, which is a more evident characteristic of the American population. We must not forget that the fewer patients treated, the more important it should be to closely follow these clinically established protocols. At the American trauma center, the degree of compliance with clinical protocols and guidelines was much greater; for this reason, the number of rule-based errors was lower, while the number of knowledge-based type errors was higher, which is much more difficult to eradicate.
The analysis of quality management of polytrauma patients is fundamental to improve their treatment and consequently their morbidity and mortality rates. It is essential to use a common language for this quality analysis in order to establish standard and universal parameters.
Preventable and potentially preventable mortality represented 8%–14% of the total of patients who had died. The avoidable errors analyzed at the American trauma center and the Spanish referral hospital were remarkably similar. Differences were found in the percentage of diagnostic errors, which appeared to be higher at the Spanish referral hospital. Although the preventable errors were mainly due to human causes at both hospitals, at the trauma center they were mostly of a knowledge-based type, while at the Spanish hospital the errors were rule-based.
Authorship- -
Sandra Montmany: study design, data collection, analysis and interpretation of the results, article composition, critical review and approval of the final version.
- -
Jose L. Pascual: study design, analysis and interpretation of the results, critical review and approval of the final version.
- -
Patrick K. Kim: study design, critical review and approval of the final version.
- -
Janet McMaster: data collection, critical review and approval of the final version
- -
Anna Pallisera: data collection, critical review and approval of the final version.
- -
Pere Rebasa: analysis and interpretation of the results, critical review and approval of the final version.
- -
Alexis Luna: data collection, critical review and approval of the final version.
- -
Salvador Navarro: study design, analysis and interpretation of the results, article composition, critical review and approval of the final version.
There were no conflicts of interest.
Please cite this article as: Montmany S, Pascual JL, Kim PK, McMaster J, Pallisera A, Rebasa P, et al. Comparación de la mortalidad evitable de un trauma center americano vs. un centro de referencia europeo. Cir Esp. 2017;95:457–464.
