





To describe the outcomes of phacoemulsification with the implant of an acrylic intraocular lens (IOL) in cataracts of adult patients with and without uveitis.
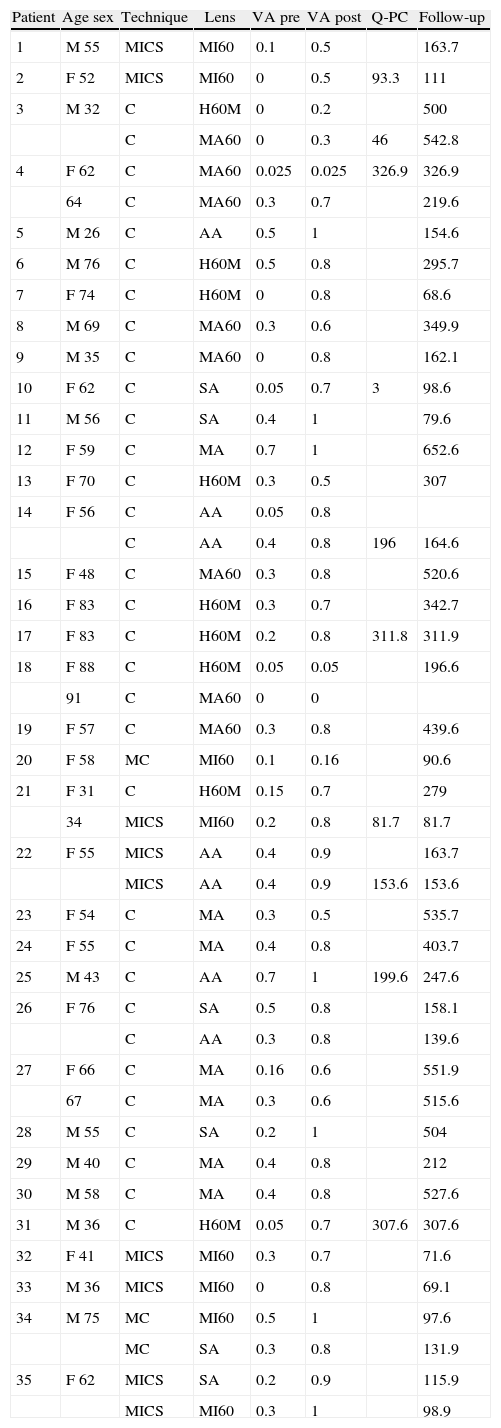
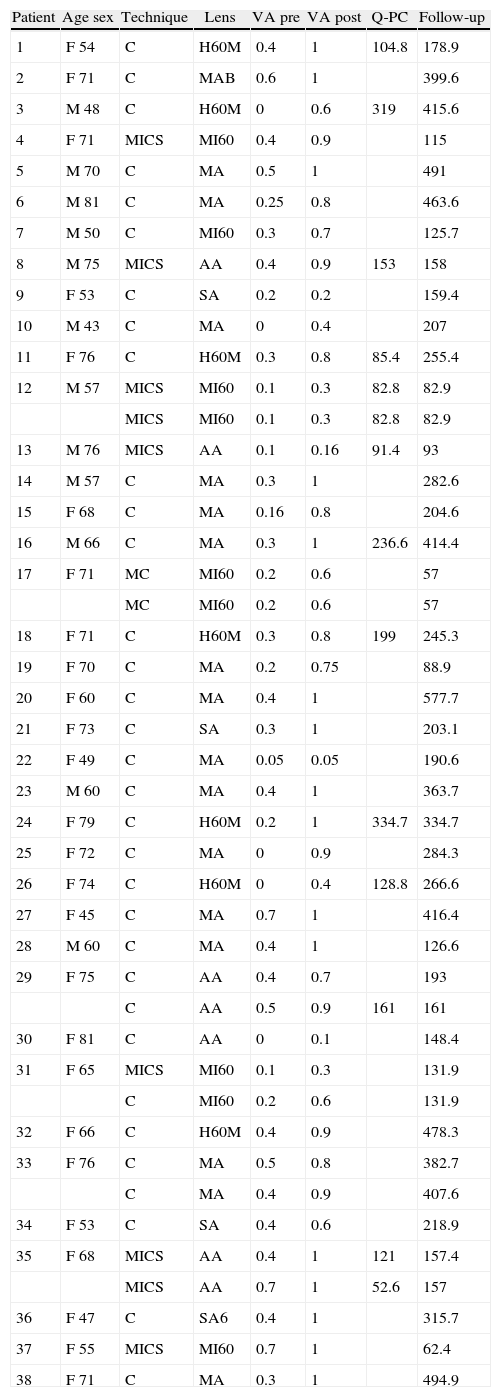
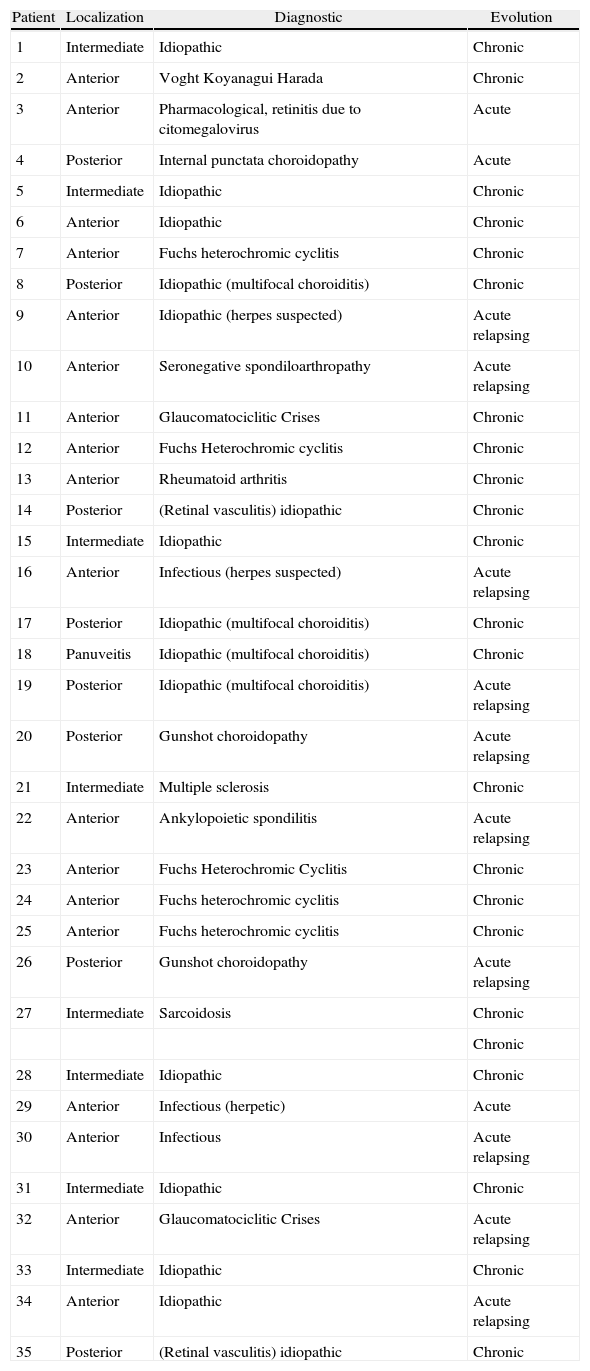
MethodsDescriptive retrospective comparative study of 35 patients (45 eyes) with uveitis (group 1) and 38 (44 eyes) control patients (group 2), who were operated on by the same surgeon, and were homogeneous as regards sex, surgical technique, IOL (hydrophobic or hydrophilic) and follow-up. The pre-surgical characteristics of risk, the difficulties and intra-surgical and postsurgical complications, the date of posterior capsulotomy and the pre- and post-surgical visual acuity (VA), were analyzed.
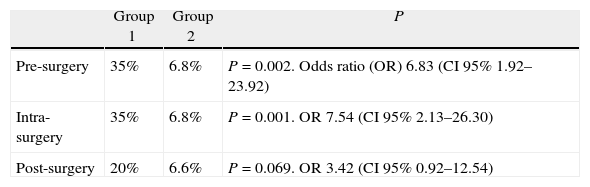
ResultsIn both groups the coaxial phacoemulsification was used in 75% of the eyes, bimanual microincision cataract surgery (MICS) in 20% and micro-coaxial in the rest. The pre-surgical risk factors (P=0.002, OR 6.83), the surgical difficulties and complications (P=0.001, OR 7.54) and postsurgical complications (P=0.069, OR 3.42) were more frequent in the uveitis group. In both 93% and 91%, respectively, of eyes improved 2 or more lines of VA. After an average follow-up of 4.9 years in both groups, 22.7% and 32% eyes (log-rank P=0.357) needed PC. The hydrophilic IOLs needed PC earlier than the hydrophobic ones (log rank P=0.001), neither the location nor the uveitis course influenced the PC rate.
ConclusionsThe consequences because of previous ocular inflammation make cataract surgery in uveitis more difficult, but with postsurgical complications, visual results and need of PC similar to our patients without inflammation.
Describir los resultados de la facoemulsificación con implante de lente acrílica en cataratas de pacientes adultos con y sin uveítis.
MétodosEstudio comparativo descriptivo retrospectivo de 35 pacientes (45 ojos) con uveítis (grupo 1) y 38 (44 ojos) sin uveítis (grupo 2) intervenidos por el mismo cirujano, homogéneos en cuanto a sexo, técnica quirúrgica, tipo de lente implantada (hidrofóbica o hidrofílica) y seguimiento. Se recogen las características pre-quirúrgicas de riesgo, dificultades y complicaciones intra-quirúrgicas y postquirúrgicas, la fecha de capsulotomía posterior y la agudeza visual previa y posterior a la cirugía.
ResultadosEn ambos grupos la facoemulsificación coaxial se utilizó en el 75% de los ojos, MICS bimanual en el 20% y microcoaxial en el resto. Los factores de riesgo prequirúrgicos (p=0,002, OR 6,83), las dificultades y complicaciones intraquirúrgicas (p=0,001, OR 7,54) y postquirúrgicas (p=0,069, OR 3,42) fueron más frecuentes en el grupo 1. El 93% y 91% respectivamente de ojos ganaron 2 o más líneas de AV. Tras un seguimiento medio de 4,9 años en ambos grupos, el 22,7% y el 32% (log-rank p=0,357) necesitaron capsulotomía posterior (CP). Las lentes hidrofílicas precisaron, en ambos grupos, capsulotomía más temprana que las hidrofóbicas (log rank p=0,001), ni la localización ni el curso de la uveítis se relacionaron con la necesidad de CP.
ConclusionesLas secuelas características de la inflamación previa hacen que la cirugía de la catarata en pacientes con uveítis sea más dificultosa, pero con complicaciones postquirúrgicas, resultados visuales y necesidad de CP similares al de nuestros pacientes sin inflamación.
