




Background. The term early allograft dysfunction (EAD) identifies liver transplant (LT) allografts with initial poor function and portends poor allograft and patient survival. Aims of this study are to use EAD as an intermediate outcome measure in a large single center cohort and identify donor, recipient and peri-operative risk factors.
Material and methods. In 1950 consecutive primary LT, donor, recipient and peri-operative data were collected. EAD was defined by the presence of one or more of the following: total bilirubin ≥ 10 mg/dL (171 μmol/L) or, INR ≥ 1.6 on day 7, and ALT/AST > 2,000 IU/L within the first 7 days.
Results. The incidence of EAD was 26.5%. 1-, 3-, and 5-year allograft and patient survival for patients who developed EAD were significantly inferior to those who did not (P < 0.01 at all time points). Multivariate analysis demonstrated associations in the development of EAD with recipient pre-operative ventilator status, donation after cardiac death allografts, donor age, allograft size, degree of steatosis, operative time and intra-operative transfusion requirements (all P < 0.01). Patients with EAD had a significantly longer hospitalization at 20.9 ± 38.9 days (median: 9; range: 4-446) compared with 10.7 ± 13.5 days (median: 7; range: 3-231) in patients with no EAD (P < 0.01).
Conclusions. This is the largest single center experience demonstrating incidence of EAD and identifying factors associated with development of EAD. EAD is a useful intermediate outcome measure for allograft and patient survival. Balancing recipient pretransplant conditions, donor risk factors and intra-operative conditions are necessary for avoiding EAD.
Due to advances in our understanding of end-stage liver disease (ESLD), operative technique, and donor management, liver transplantation (LT) has become the definitive therapy for many patients with decompensated cirrhosis. Outcomes after LT are measured by final endpoints such as allograft loss and patient mortality. Early allograft dysfunction (EAD) has been previously described as a clinical tool for identifying initial poor function of a liver allograft.1 More recently, in a multi-center cohort study of 297 patients, this tool was modified and validated as an intermediate end-point for identifying patients at risk for allograft loss or mortality within 6 months after LT.2 In the latter study, using a multi-variate model, the authors found donor age and recipient Model for End-Stage Liver Disease (MELD) score at the time of LT as significant risk factors for development of EAD. While this study was limited by challenges that face many multicenter studies due to the heterogeneity of the datasets and the number of risk factors considered, its results supported the use of EAD as an intermediate end-point which was embraced as a target for therapeutic intervention to reduce mortality, morbidity and resource utilization.3–8 Despite this acceptance, our understanding of EAD remains limited since no single study has combined the granularity of recipient, donor and peri-operative data and the power of a large number of patients. Herein, we present a large single center experience of 1,950 consecutive LT recipients with the aim of identifying incidence and risk factors associated with the development of EAD as a modifiable outcome measure.
Material and MethodsAll primary LT cases performed between February 2002 and July 2013 at Mayo Clinic Florida (Jacksonville, FL) were reviewed retrospectively. Exclusion criteria for this study were recipients in whom follow-up was inadequate to assess for EAD or who had undergone liver retransplant. Approval for this study was obtained from the Mayo Clinic Institutional Review Board.
Detailed information regarding the donors and the recipients were obtained from the Mayo Clinic Florida transplant database. Surgical techniques for both procurement and recipient operation were previously described.9 Biological MELD score on the day of transplant was used in all cases. Donor risk index (DRI) was calculated for all liver allografts.10 Cold ischemia time (CIT) was defined as the time from infusion of cold preservation solution until implantation of the liver allograft in the recipient. Warm ischemia time (WIT) was the warming period of the liver allograft during implantation: the period between out of cold preservation solution to reperfusion through portal flow. A wedge biopsy 1 h after reperfusion was performed. This biopsy was reviewed by a liver pathologist. Using a definition previously described, moderate steatosis was defined by > 30% steatosis on histopathology.11
As previously described, data regarding EAD was defined by the presence of one or more of the following variables:1
- •
Total bilirubin ≥ 10 mg/dL (171 μmol/L) on postoperative day 7.
- •
INR ≥ 1.6 on postoperative day 7.
- •
ALT or AST > 2,000 IU/mL within the first 7 postoperative days.
Allograft survival was timed from the transplant date until the date of retransplantation or death (whichever came first) and was censored for the date of the end of the study period or for the date of the last correspondence (for losses to follow-up). The allograft and patient survival rates were compared with Kaplan-Meier plots and logrank tests. Univariate analysis of clinical risk factor association with EAD was conducted using χ2 test for categorical variables and Wilcoxon signed-rank sum test for continuous variables after assessing for normality. A univariate Cox proportional hazard model predicting survival was performed. Significant variables were then used to perform a multivariate Cox proportional hazard model with backwards stepwise selection. A retention criterion of P < 0.05 level of significance during the backward stepwise search was used.12 A P-value of 0.05 following adjustment for confounding was considered statistically significant. All statistical analysis was performed with STATA 13 (StataCorp LP, College Station, TX).
ResultsBetween February 2002 and July 2013, 1,962 primary adult LT were performed at the Mayo Clinic Florida Transplant Program. Twelve LT were excluded due to lack of follow-up to assess for EAD. Data from 1,950 consecutive LT were reviewed. 1,307 (67%) recipients were male and 789 (40.4%) had hepatitis C virus as the primary diagnosis for ESLD. The mean recipient age was 56 years (median: 56, range: 19-80 years), the mean donor age was 46.1 years (median: 47, range: 2-90 years). The mean DRI was 1.66 (median: 1.60, range: 0.83-4.30). Post reperfusion liver biopsies were available in 1,902 cases. Moderate steatosis was identified in 8.9% of these biopsies. The mean follow-up time was 65.6 months (median: 61.6 months, range: 9 days-12 years). Two hundred and twenty-eight (11.7%) LT were performed using liver allografts from DCD donors.
Five hundred and eighteen (26.5%) recipients were found to have had EAD. The 1-, 3-, and 5- year patient survival for those who did not have EAD compared with those who did were 94.7% vs. 85.1%; 87.4% vs. 74.8%; and 78.8% vs. 65.2%, respectively (p < 0.01 at all time points). 1-, 3-, and 5-year allograft survival for patients who did not have EAD compared with those who did were 91.4% vs. 78.6%; 83.5% vs. 67.9%; and 74.8% vs. 57.2, respectively (p < 0.01 at all time points) (Figure 1). The sensitivity and specificity of EAD for 1 year mortality was 50.3% and 75.49% respectively. The negative and positive predictive values were 94.7% and 14.86%, respectively. The sensitivity and specificity of EAD for 1 year graft failure was 47.4% and 76.3% respectively. The negative and positive predictive values were 91.4% and 21.4%, respectively.
 patient survival and (B) allograft survival for LT recipients who did not experience and who did experience EAD.")
A subgroup sensitivity analysis for patients who had early graft failure in the first 30 days of transplant due to primary nonfunction or early technical issues was performed to confirm the impact of EAD on long term outcomes. A total of 55 (2.8%) patients had early graft loss within the first 30 days after transplant, of which 63% experienced EAD. After dropping these patients, the 1-, 3-, or 5- year patient survival for patients who did not have EAD vs. those who did were 95.2% vs. 86.8%; 87.7% vs. 77.5%; and 79.6% vs. 67.9%, respectively (p < 0.01 at all time points). 1-, 3-, and 5- year graft survival for patients who did not have EAD compared with those who did were 92.7% vs. 84.1%; 84.9% vs. 73.4%; and 76.5% vs. 62.5%, respectively (p < 0.01 at all time points). Even when excluding the patients who had early graft loss, the impact of EAD still had statistically significant differences in both long term patient and allograft survival.
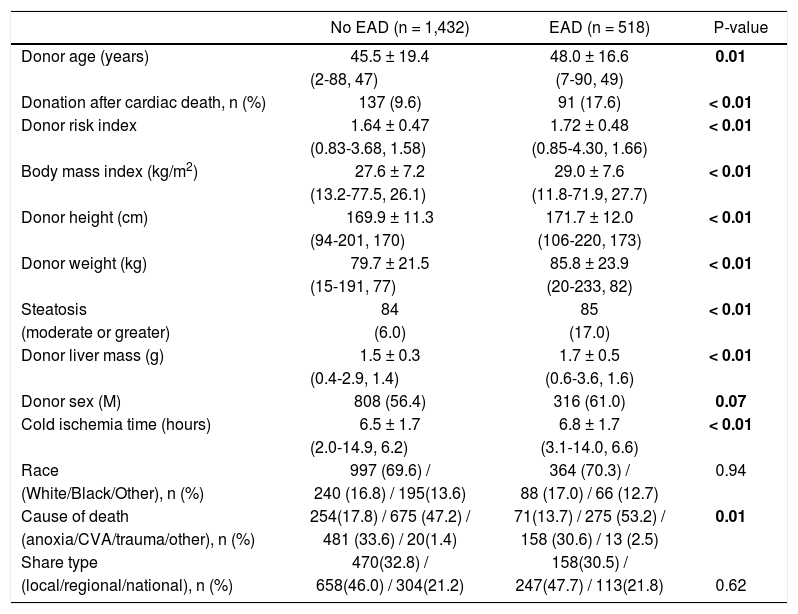
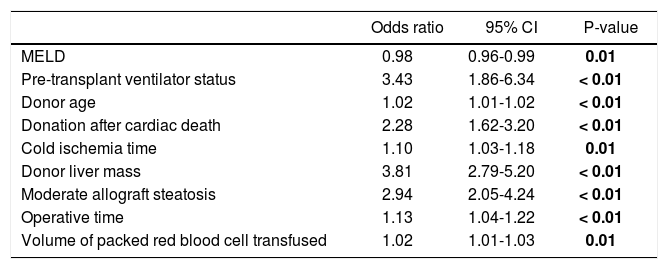
The donor, recipient and intra-operative risk factors associated with EAD are presented in tables 1-3. These variables were then analyzed with a step-wise Cox proportional hazard model, which demonstrated significant association of the development of EAD with the recipient’s pre-LT ventilator status (OR: 3.43; 95% CI: 1.86-6.34; p < 0.01). Regarding other variables there was a statistically significant association with the development of EAD and donor age (OR: 1.02; 95% CI: 1.01-1.02; p < 0.01), DCD status (OR: 2.28; 95% CI: 1.62-3.20; p < 0.001), Donor liver mass (OR: 3.81; 95% CI: 2.79-5.20; p < 0.01), and moderate steatosis in allograft (OR: 2.94; 95% CI: 2.05-4.24; p < 0.01), CIT (OR: 1.10; 95% CI: 1.03-1.18, p = 0.01), volume of packed red blood cells (PRBC) transfused (OR: 1.02; 95% CI: 1.01-1.03; p = 0.01), and operative time (OR: 1.13; 95% CI: 1.04-1.22; p < 0.01) (Table 4).
Donor characteristics.
| No EAD (n = 1,432) | EAD (n = 518) | P-value | |
|---|---|---|---|
| Donor age (years) | 45.5 ± 19.4 | 48.0 ± 16.6 | 0.01 |
| (2-88, 47) | (7-90, 49) | ||
| Donation after cardiac death, n (%) | 137 (9.6) | 91 (17.6) | < 0.01 |
| Donor risk index | 1.64 ± 0.47 | 1.72 ± 0.48 | < 0.01 |
| (0.83-3.68, 1.58) | (0.85-4.30, 1.66) | ||
| Body mass index (kg/m2) | 27.6 ± 7.2 | 29.0 ± 7.6 | < 0.01 |
| (13.2-77.5, 26.1) | (11.8-71.9, 27.7) | ||
| Donor height (cm) | 169.9 ± 11.3 | 171.7 ± 12.0 | < 0.01 |
| (94-201, 170) | (106-220, 173) | ||
| Donor weight (kg) | 79.7 ± 21.5 | 85.8 ± 23.9 | < 0.01 |
| (15-191, 77) | (20-233, 82) | ||
| Steatosis | 84 | 85 | < 0.01 |
| (moderate or greater) | (6.0) | (17.0) | |
| Donor liver mass (g) | 1.5 ± 0.3 | 1.7 ± 0.5 | < 0.01 |
| (0.4-2.9, 1.4) | (0.6-3.6, 1.6) | ||
| Donor sex (M) | 808 (56.4) | 316 (61.0) | 0.07 |
| Cold ischemia time (hours) | 6.5 ± 1.7 | 6.8 ± 1.7 | < 0.01 |
| (2.0-14.9, 6.2) | (3.1-14.0, 6.6) | ||
| Race | 997 (69.6) / | 364 (70.3) / | 0.94 |
| (White/Black/Other), n (%) | 240 (16.8) / 195(13.6) | 88 (17.0) / 66 (12.7) | |
| Cause of death | 254(17.8) / 675 (47.2) / | 71(13.7) / 275 (53.2) / | 0.01 |
| (anoxia/CVA/trauma/other), n (%) | 481 (33.6) / 20(1.4) | 158 (30.6) / 13 (2.5) | |
| Share type | 470(32.8) / | 158(30.5) / | |
| (local/regional/national), n (%) | 658(46.0) / 304(21.2) | 247(47.7) / 113(21.8) | 0.62 |
Continuous variables are presented as means and standard deviations (with ranges and medians in parentheses). Categorical values are presented in numbers and percentages (in parentheses). Significant p-values are in bold.
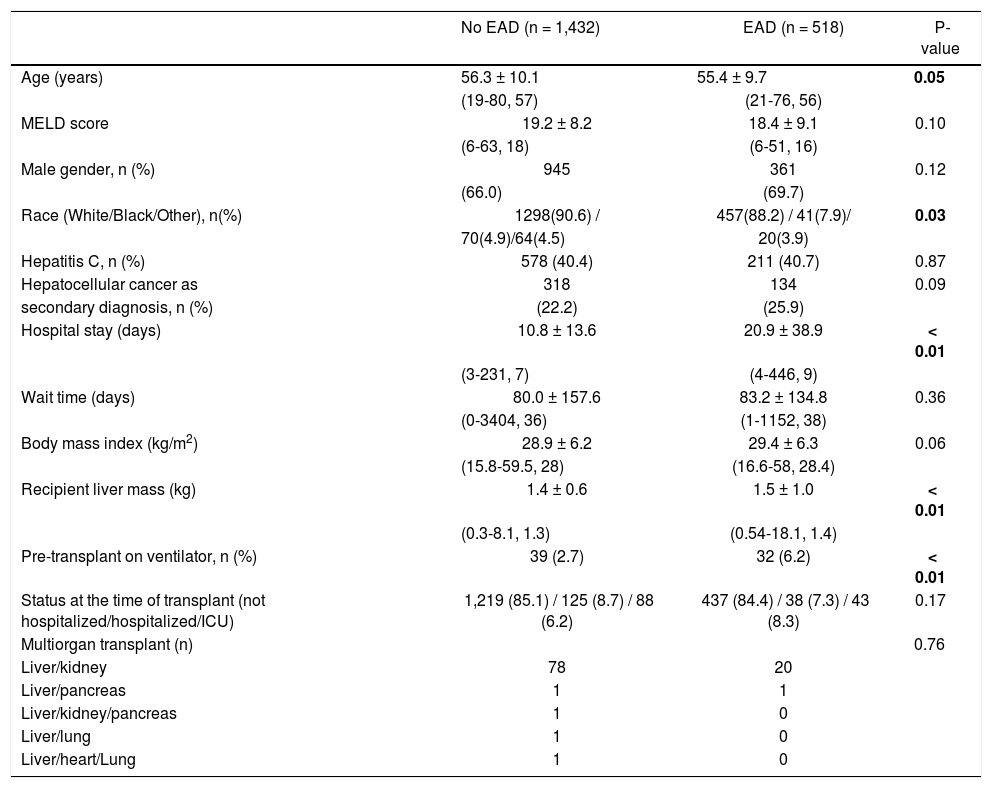
Recipient characteristics.
| No EAD (n = 1,432) | EAD (n = 518) | P-value | |
|---|---|---|---|
| Age (years) | 56.3 ± 10.1 | 55.4 ± 9.7 | 0.05 |
| (19-80, 57) | (21-76, 56) | ||
| MELD score | 19.2 ± 8.2 | 18.4 ± 9.1 | 0.10 |
| (6-63, 18) | (6-51, 16) | ||
| Male gender, n (%) | 945 | 361 | 0.12 |
| (66.0) | (69.7) | ||
| Race (White/Black/Other), n(%) | 1298(90.6) / | 457(88.2) / 41(7.9)/ | 0.03 |
| 70(4.9)/64(4.5) | 20(3.9) | ||
| Hepatitis C, n (%) | 578 (40.4) | 211 (40.7) | 0.87 |
| Hepatocellular cancer as | 318 | 134 | 0.09 |
| secondary diagnosis, n (%) | (22.2) | (25.9) | |
| Hospital stay (days) | 10.8 ± 13.6 | 20.9 ± 38.9 | < 0.01 |
| (3-231, 7) | (4-446, 9) | ||
| Wait time (days) | 80.0 ± 157.6 | 83.2 ± 134.8 | 0.36 |
| (0-3404, 36) | (1-1152, 38) | ||
| Body mass index (kg/m2) | 28.9 ± 6.2 | 29.4 ± 6.3 | 0.06 |
| (15.8-59.5, 28) | (16.6-58, 28.4) | ||
| Recipient liver mass (kg) | 1.4 ± 0.6 | 1.5 ± 1.0 | < 0.01 |
| (0.3-8.1, 1.3) | (0.54-18.1, 1.4) | ||
| Pre-transplant on ventilator, n (%) | 39 (2.7) | 32 (6.2) | < 0.01 |
| Status at the time of transplant (not hospitalized/hospitalized/ICU) | 1,219 (85.1) / 125 (8.7) / 88 (6.2) | 437 (84.4) / 38 (7.3) / 43 (8.3) | 0.17 |
| Multiorgan transplant (n) | 0.76 | ||
| Liver/kidney | 78 | 20 | |
| Liver/pancreas | 1 | 1 | |
| Liver/kidney/pancreas | 1 | 0 | |
| Liver/lung | 1 | 0 | |
| Liver/heart/Lung | 1 | 0 |
Continuous variables are presented as means and standard deviations (with ranges and medians in parentheses). Categorical values are presented in numbers (with percentages in parentheses). Significant p-values are in bold.
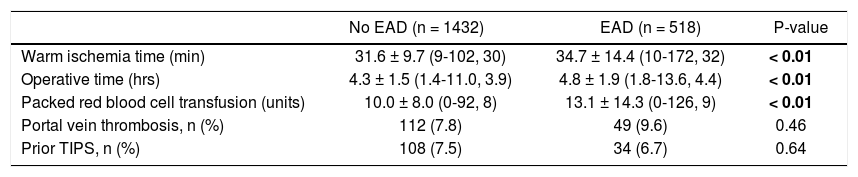
Intraoperative variables.
| No EAD (n = 1432) | EAD (n = 518) | P-value | |
|---|---|---|---|
| Warm ischemia time (min) | 31.6 ± 9.7 (9-102, 30) | 34.7 ± 14.4 (10-172, 32) | < 0.01 |
| Operative time (hrs) | 4.3 ± 1.5 (1.4-11.0, 3.9) | 4.8 ± 1.9 (1.8-13.6, 4.4) | < 0.01 |
| Packed red blood cell transfusion (units) | 10.0 ± 8.0 (0-92, 8) | 13.1 ± 14.3 (0-126, 9) | < 0.01 |
| Portal vein thrombosis, n (%) | 112 (7.8) | 49 (9.6) | 0.46 |
| Prior TIPS, n (%) | 108 (7.5) | 34 (6.7) | 0.64 |
Continuous variables are presented as means and standard deviations (with ranges and medians in parentheses). Categorical values are presented in numbers and percentages (in parentheses). Significant p-values are in bold.
Multivariate analysis of risk factors for EAD.
| Odds ratio | 95% CI | P-value | |
|---|---|---|---|
| MELD | 0.98 | 0.96-0.99 | 0.01 |
| Pre-transplant ventilator status | 3.43 | 1.86-6.34 | < 0.01 |
| Donor age | 1.02 | 1.01-1.02 | < 0.01 |
| Donation after cardiac death | 2.28 | 1.62-3.20 | < 0.01 |
| Cold ischemia time | 1.10 | 1.03-1.18 | 0.01 |
| Donor liver mass | 3.81 | 2.79-5.20 | < 0.01 |
| Moderate allograft steatosis | 2.94 | 2.05-4.24 | < 0.01 |
| Operative time | 1.13 | 1.04-1.22 | < 0.01 |
| Volume of packed red blood cell transfused | 1.02 | 1.01-1.03 | 0.01 |
Patients with EAD had a significantly longer hospitalization at 20.9 ± 38.9 days (median: 9; range: 4-446) compared with 10.7 ± 13.5 days (median: 7; range: 3-231) in patients with no EAD (P < 0.01).
DiscussionThis report describes the incidence and risk factors associated with the development of EAD in the largest series to date of LT recipients. In addition, the current analysis links the development of EAD with short- and long-term outcomes after LT. In 1,950 consecutive recipients of liver allografts, those recipients who developed EAD had a significant patient and allograft survival disadvantage compared to those who did not experience EAD. This survival disadvantage had a long term effect on 1-,3-, and 5- year patient and allograft survival and persisted even when patients who had early graft loss (in the first 30 days after LT) were excluded.
The term EAD implies poor liver allograft function within the first week of transplantation. Using objective criteria to define EAD, Deschenne, et al. identified a subset of patients who eventually had a higher risk of losing their allograft or risk of death within 6 months after LT.1 More recently Olthoff, et al. modified the original criteria in a multicenter retrospective analysis, and identified donor age and recipient MELD score as risk factors for the development of EAD.2 While this study was important in demonstrating EAD as an objective measure that can be used to track outcomes and perhaps be used as an intermediate outcome measure, it was limited due to the number of subjects and number of risk factors considered. If the development of EAD is a clear risk factor for poor outcomes in the short- and long-term, then investigating all potential contributing factors has value. Identifying potentially modifiable risk factors may encourage the development of early interventions that could decrease the incidence or mitigate the course of EAD. Therefore in our study, we undertook the current analysis in a larger cohort of patients in a single center retrospective study. To identify risk factors, we chose a contemporary cohort of LT recipients after implementation of the MELD score in organ allocation.
The current analysis demonstrates the critical interplay between donor risk factors, recipient characteristics, and intra-operative events. In multivariate analysis, statistically significant risk factors for the development of EAD included recipient ventilator status before LT, donor age, allograft steatosis, allograft mass, DCD status, CIT, intra-operative PRBC transfusion, and operative time. While MELD score is a widely used objective measure of mortality risk associated with ESLD, it has not been consistently found to be a major risk factor for the development of EAD.1,13-15 In our study, MELD score did not appear to have an impact on the risk of EAD. While the multivariate analysis showed a statistically significant increased odds ratio for EAD in patients with lower MELD scores, the MELD score difference of 0.8 is likely negligible in a clinical setting. This finding is more likely a statistical anomaly related to the tight distribution of MELD scores in our practice, which makes interpretation difficult. A larger multi-institutional study with a broader distribution of MELD scores would be necessary to fully understand this. However, another important variable, the recipient’s ventilator status, was found to be a major factor. Unlike ICU status before LT, ventilator status before LT correlated with an increased risk for developing EAD. Our analysis indicates that ventilator support regardless of MELD score is a more accurate and objective measure of the patient’s medical condition immediately prior to transplant. These findings may be considered an extrapolation of findings in a previously published multi-center cohort of 2,982 pediatric LT recipients, in which the only statistically significant risk factor for early graft loss was the intubated ICU recipient.16 In another study by Olthoff, et al., who intended to characterize cytokine expression in EAD, the authors found an association between pre-LT levels of proinflammatory cytokines (IL-6 and IL-2R) and the risk of EAD.17 Taken together, we believe these findings suggest that EAD is not limited to donor and intraoperative events, but also the recipient’s preoperative condition.
In the current analysis, four donor factors (donor age, allograft steatosis, donor liver mass, DCD status), were found to be associated with EAD. Prior studies have established older donors and allograft steatosis as risk factors in overall outcomes as well as the development of EAD.2,7 In our study where there was a large number of available post-reperfusion allograft biopsies, we confirm the effect of allograft steatosis as a risk factor. As the general population in the United States ages and the incidence of obesity is increasing, these two donor factors will likely impact the number of liver allografts available as well as outcomes after LT. We believe it is critical to mitigate these by appropriate donor-recipient matching and by using therapeutic maneuvers to decrease the incidence of EAD. While some of the donor factors may currently appear to be unmodifiable, new methods to resuscitate liver allografts, such as the wider use of cold/warm liver perfusion methods, may prove very valuable in the successful implantation of higher risk organs.18-20 We previously demonstrated a higher incidence of EAD when allografts from DCD donors were used.21 It is likely that DCD allografts sustain more injury due to the ischemic insult that occurs at the time of donor withdrawal phase. The high incidence of EAD in recipients of DCD liver allografts shows that at the present time they should indeed be considered marginal donors. Similar to donor age and allograft steatosis, DCD rates will likely increase in the future: we believe that it is incumbent on the transplant community to identify appropriate methods to successfully utilize these allografts.22 A novel finding in our study is that larger allograft mass was found to be a risk factor. Shorter recipient height as a risk factor for EAD development, a tangentially related finding in a previous report, may point to the challenges associated with using larger grafts in smaller recipients.9 In the context of EAD, a larger allograft may have more hepatocyte mass and may be at higher risk for injury due to increased intraabdominal pressure or compression after the case is completed.23 Intra-abdominal hypertension, for which larger allografts are at increased risk, is an often underappreciated phenomenon after LT and may be playing a role in the development of EAD. To further explore this issue would require prospective study and intra-abdominal pressure measurements, which are beyond the scope of this manuscript. Regardless, a larger allograft may also add complexity to the transplant operation, as exposure becomes more difficult with a larger liver.
Technically more challenging operations were associated with the development of EAD. We think that proxies for a challenging operation included increased CIT, operative time and intraoperative blood transfusion requirements. While we observed a statistical association, it is unclear from our data whether there was a causal relationship between operative time and intraoperative blood utilization with the development of EAD. An alternative explanation is that those allografts that were destined to have EAD already showed signs of initial poor function at the time of LT, resulting in an increased transfusion requirement, as well as longer operative time spent to establish hemostasis.
Understanding the causes and consequences of EAD can help a transplant center improve its overall outcomes. In our study, EAD was most affected by donor selection. While EAD is certainly a risk factor for allograft loss and mortality, post-LT mortality and morbidity should be carefully balanced against the risk of death on the wait list, especially in regions where organ donation rates are low. There is evidence that declining potential liver allografts is detrimental for those on the waiting list, and this behavior may be the largest driver for waitlist mortality.24,25 As a result of increasing numbers of extended criteria donors, the liver transplant community will have to adapt by implementing strategies to decrease complications related to liver allografts coming from such donors. Identifying the appropriate recipient and operative risk to match the donor risk should lead to improvements in the incidence of EAD and transplant outcomes. Understanding the variation in transplant center mortality in patients with EAD may allow for opportunities for investigation in “failure to rescue”.26 Other preventative and therapeutic measures to increase allograft and patient survival using allografts at risk of EAD should be the focus of future investigation. From an individual patient standpoint, a more granular prognosis could be provided by transplant providers. In those patients with a diagnosis of EAD, medium to long-term patient care protocols could be modified in order to minimize effects of EAD.
Hospital length of stay after LT, a proxy for resource utilization, was significantly different between patients who developed EAD compared with those who did not. A more detailed analysis will be considered in the future to better characterize the increased resource utilization associated with EAD.
Our study involving a large cohort of patients at a single transplant center provides insight into EAD as an intermediate endpoint in the care of LT recipients. Strengths of the study include the size of the patient population, inclusion of LT after implementation of MELD score and a uniform practice within our center, including surgical technique and medical management as well as standardized data collection. The single center nature of the dataset may be regarded as a weakness. Future multi-center studies involving additional subjects will complement our findings and may identify other risk factors. Molecular markers also may provide targets for future therapeutic interventions in patients at particular risk for developing EAD.
In summary, this large single center study provides new insights into the utility of EAD as an intermediate end-point in LT. The development of EAD was associated with inferior allograft and patient outcomes as well as increased resource utilization post-LT. Identifying measures to minimize EAD should be a focus of the transplant community. For future quality initiatives, EAD should be considered as a reportable metric for transplant centers so that patient outcomes are measured by more than just allograft loss or mortality.



