





The case is described of a 46 year old female alcoholic, presenting with confusion, jaundice and reduced level of consciousness. The patient was hyponatraemic on admission and despite gradual correction of serum sodium the patient deteriorated neurologically. Magnetic Resonance Imaging scan of the brain revealed characteristic findings of Central Pontine Myelinolysis (CPM). We provide an overview of the first published cases of CPM. The clinical and pathological features of CPM are described. No specific therapy has been shown to improve outcome; current literature advocates supportive management. Identification of patients at risk and gradual correction of hyponatraemia is recommended.
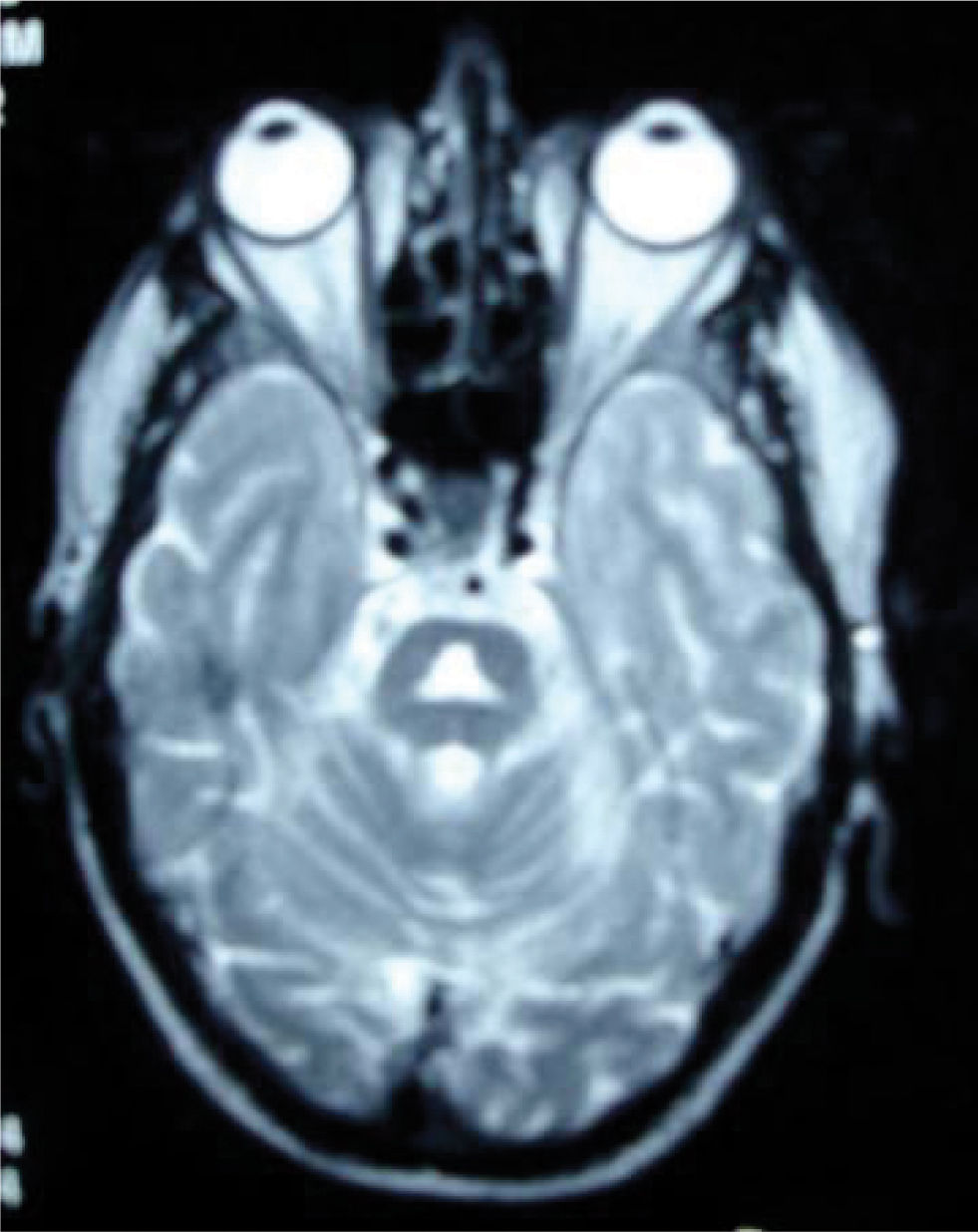
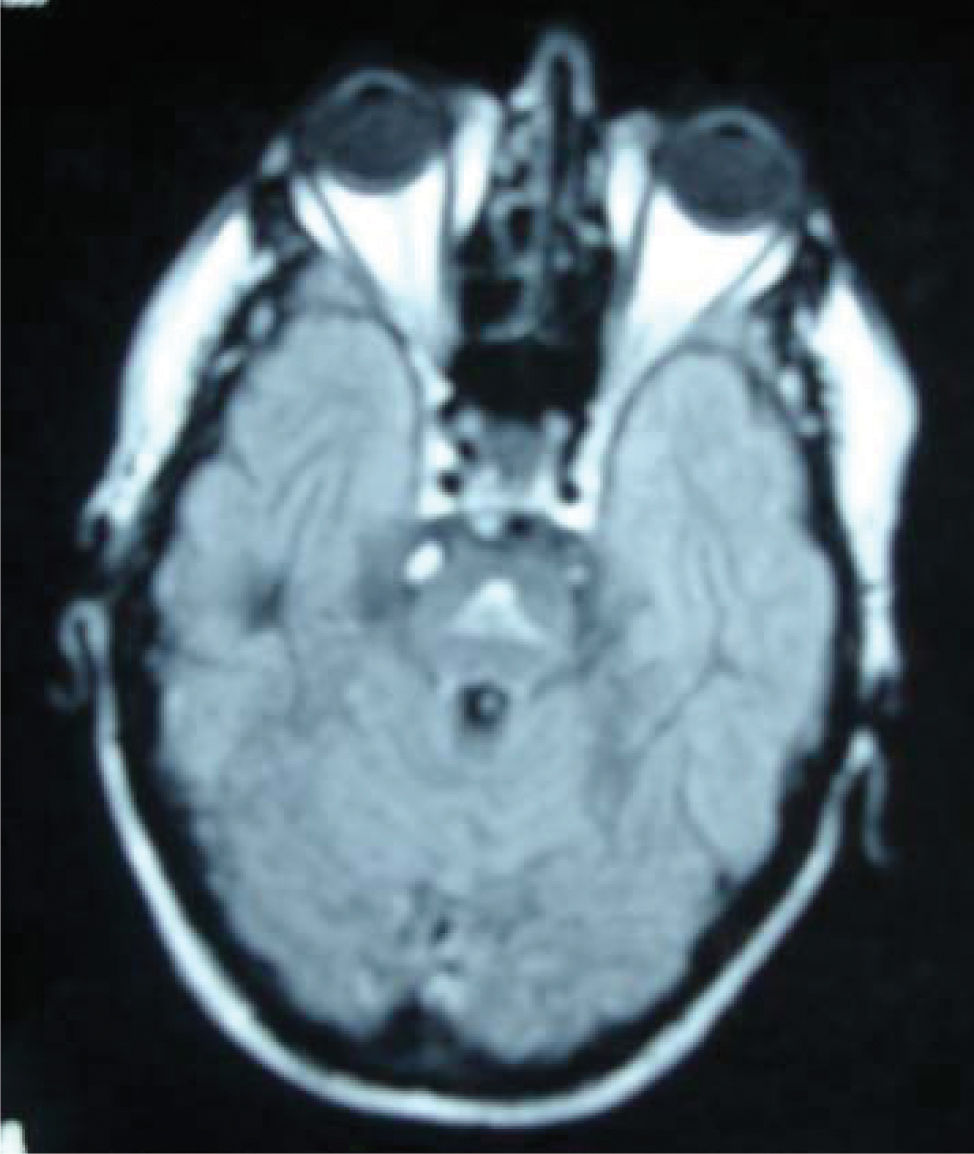
A 46-year-old patient was admitted to hospital with confusion, jaundice, bruising and serum sodium of 129 mmol/L. She had a long history of alcohol abuse. Examination revealed signs of chronic liver disease, reduced level of consciousness but no focal neurological deficit. Renal function was otherwise normal and liver function tests were in keeping with alcohol abuse. She was treated for hepatic encephalopathy and alcohol withdrawal with appropriate doses of lactulose and IV vitamins. Serum sodium was corrected gradually. Unfortunately her conscious level declined further and she required intubation. In the intensive care unit she was successfully weaned-off ventilation and Magnetic Resonance Imaging of her brain showed a triangular shaped area of high T2W signal return (Figures 1and2) lying centrally within the pons. Signal return from rest of brain was normal. Appearances were suggestive of central pontine myelinolysis.
Following transfer to the ward she made a steady recovery with the aid of adequate nutrition and physiotherapy. Electrolyte levels have remained satisfactory and a gradual neurological improvement has been noted.
DiscussionCentral pontine myelinolysis (CPM) was described by Adams et al in 1959 as a disease affecting alcoholics and the malnourished.1,2 Reports of similar lesions, occurring outside the pons, started to appear in the medical literature and the entity of extrapontine myelinolysis (EPM) was eventually established.3,4
Tomlinson et al in 1976, described two cases of middle aged women who presented with protracted vomiting and drowsiness.5 Both had significant hyponatraemia but no underlying malignancy, alcoholism, malnutrition or other serious disease was found. Eventually, correction of the electrolyte abnormalities was accompanied by deterioration in patient level of consciousness and development of a neurological syndrome characterized by quadriparesis, dysphasia and mutism. It was few years later though when, the link of CPM and rapid correction of hyponatraemia was established.
Pathologically, CPM is defined as a symmetric area of myelin disruption in the centre of the basis pontis.7 It is caused by large intracellular shifts in water associated with rapid correction of hyponatraemia. Clinical presentation is with flaccid paralysis, altered consciousness and often facial or bulbar weakness.2
Despite the fact that hyponatraemia is the most common electrolyte abnormality in clinical practice only a minor proportion of patients develop CPM. The mechanism underlying the entity is still unclear but the recorded associations are known to be: alcoholism, malnutrition, prolonged diuretic use, psychogenic polydipsia, burns (infrequent, and often in the context of hypernatraemia), post-liver transplant (well recognized), post-pituitary surgery (rare), post-urological surgery/gynaecological surgery, especially if involving glycine infusions.2 It very rarely occurs in the absence of another significant illness.
The typical patient with decompensated liver disease and CPM has often undergone a biphasic clinical course. The initial presentation will be that of encephalopathy and confusion, sometimes accompanied by seizures due to acute alcohol withdrawal or hyponatraemia, which will resolve as normonatraemia is restored. Neurological deterioration often occurs several days later.
In alcoholics it is often seen despite gradual correction of hyponatraemia. Chronic alcoholics may be predisposed to CPM due to metabolic deficiencies causing an oligodendroglial pro-apoptotic state.8
CPM should be suspected when an alcoholic or malnourished patient develops confusion, quadriplegia, pseudobulbar palsy, or reduced level of consciousness over a period of several days.6
MRI produces characteristic pontine lesions that aid the diagnosis. Prevention involves identifying patients at risk. In this group the correction of serum sodium should be at no more than 2-3 mmol/day. No specific trials for treatment have been performed and supportive treatment is all that is currently recommended. Case reports and case series have often shown a high mortality.2 However the prognosis of CPM is variable and depends on the cause. Some patients make a full neurological recovery.



