







Data on epidemiology of liver diseases in Brazil is scarce. This study aimed to estimate the burden of chronic viral hepatitis and liver cirrhosis in the country.
Materials and MethodsThe indicator used was disability-adjusted life year (DALY), a sum of years of life lost due to premature mortality (YLL) and years lived with disability (YLD). Liver cirrhosis was analyzed in etiologic categories and cirrhosis of viral origin was considered part of the burden of chronic hepatitis.
ResultsThere were 57,380 DALYs (30.3 per 100,000 inhabitants) attributable to chronic hepatitis B and cirrhosis due to hepatitis B, with 41,262 DALYs in men. Most burden was caused by YLL (47,015 or 24.8/100,000) rather than YLD (10,365 or 5.5/100,000). Chronic hepatitis C and cirrhosis due to hepatitis C were responsible for 207,747 DALYs (109.6/100,000), of which 137,922 were YLL (72.7/100,000) and 69,825 (36.8/100,000) were YLD, with a higher proportion of DALYs in men (73.9%). Cirrhosis due to alcohol or other causes had a total of 536,169 DALYs (1,4% of total DALYs in Brazil), with 418,272 YLL (341,140 in men) and 117,897 YLD (97,965 in men). Highest DALYs’ rates occurred at ages 60-69 in chronic hepatitis and at ages 45-59 in cirrhosis due to alcohol or other causes.
ConclusionChronic viral hepatitis and liver cirrhosis are responsible for a significant burden in Brazil, affecting mainly men and individuals still in their productive years. Most burden is related to non-viral causes of cirrhosis, with a major contribution of alcohol.
Liver diseases are a relevant health problem in the world.1-5 According to the Global Burden of Disease Study 2010 (GBD 2010), cirrhosis was the 17th cause of death globally, being responsible for approximately one million deaths in this year.6 In GBD 2013, cirrhosis was the 13th cause of years of life lost in the world.7
Cirrhosis represents the end-stage of chronic liver dis-ease8,9 and is characterized by an asymptomatic or compensated phase and a progressive or decompensated phase.8 The development of complications such as ascites, gastrointestinal bleeding, encephalopathy and spontaneous bacterial peritonitis mark the beginning of the decompensated phase, which has a survival of approximately 2 years compared to a median survival of more than 12 years in compensated cirrhosis.8 Chronic viral hepatitis are important causes of cirrhosis.10,11
Despite the importance of chronic liver disease, there is still paucity of data on the epidemiology of this group of diseases in developing countries.12 In Brazil, there were 853,571 hospital admissions attributed to liver disease from 2001 to 2010, which corresponded to 0.72% of all admissions in the country in the same period.13 Data on specific causes of liver disease in Brazil, however, is scarce.
The burden of disease methodology is an approach that considers both premature death as well as the non-fatal health consequences of disease and injury, through the indicator called Disability Adjusted Life Year (DALY).14 The latter corresponds to the sum of Years of Life Lost (YLL) and Years Lived with Disability (YLD).14
The aim of this study was to describe the burden of chronic viral hepatitis B and C and liver cirrhosis in Brazil in 2008 through estimates of DALY, YLL and YLD.
Materials and MethodsData presented is part of the Brazilian Burden of Disease Study for the year 2008 (Estudo de Carga de Doença no Brasil-2008/ECDB-2008).15 This study evaluated approximately 100 diseases and injuries, which were classified into three groups according to the Global Burden of Disease Study (GBD):14 communicable, maternal, neonatal and nutritional diseases (Group I), noncommunicable diseases (Group II) and injuries (Group III).15
The indicator used to summarize the burden of premature mortality and disability was the disability-adjusted life year (DALY), which corresponds to the sum of years of life lost due to premature mortality (YLL) and years lived with disability (YLD).14
YLL estimatesTo estimate YLL in ECDB-2008, deaths from 2007 to 2009 were obtained from the Brazilian Mortality Information System (Sistema de Informação de Mortalidade – SIM), which includes the main cause of death from all death certificates in the country. Causes of death are registered according to the tenth version of the International Classification of Diseases (ICD-10) codes. Deaths in 2008 were considered the mean of the three years and a correction for underreporting was applied according to sex and age in each state of Brazil. In the whole country, the correction was of 27% for deaths under one year of age and 13% for deaths at the age of one or older. Garbage codes (10.5% of deaths in Brazil in 2008) and deaths from ill-defined causes (7.4% of deaths in the country in that year) were proportionately redistributed according to state, sex, age and cause of death.
ICD-10 codes that would refer to deaths from chronic hepatitis B, chronic hepatitis C and liver cirrhosis were defined by an expert panel including hepatologists from university hospitals in different regions of Brazil and members of the ECDB-2008 research group. A consensus meeting was organized and a proposal of distribution of codes based on previous literature review was sent to invited experts before the event. Codes defined as attributable to cirrhosis were further distributed into four etiologic categories: “alcohol”, “hepatitis C”, “hepatitis B” and “other causes”. This distribution was made based on a previous cirrhosis national inquiry conducted by the Brazilian Society of Hepatology in 2001, which described cir-rhotic patients followed in Hepatology Services around the country (data not published). This inquiry found that hepatitis C and hepatitis B were responsible for about 37% and 11% of cases of liver cirrhosis, respectively. Alcohol was the etiology of cirrhosis in 31% of patients and other causes and unknown causes of cirrhosis accounted for approximately 20% of cases.
YLD estimatesYLD estimates are based on incidence, duration of the condition and disability weights.14Since data on incidence of viral hepatitis and cirrhosis in Brazil is scarce, prevalence of these conditions in the country was first estimated and then used for modelling of disease in Dismod II, a World Health Organization's software tool. Other parameters included in the modelling strategy were mortality and remission. Incidence and duration of the conditions were obtained from the modelling process. Disability weights in this study were the ones described in the original Global Burden of Disease Study.7,14
Prevalence estimates of chronic hepatitis B and C were based on a recent viral hepatitis national survey, a population-based study which included individuals in all capital cities and the federal district.16,17 Since the study included only symptom-free subjects, prevalence of hepatitis B surface antigen (HbsAg) obtained in the survey was considered the prevalence of chronic hepatitis B. Sex and age distributions were the same as the survey. For hepatitis C, it was considered that 70% of antibody to hepatitis C virus (anti-HCV) prevalence in the survey represented cases of chronic hepatitis. Sex distribution was the same as the survey while age distribution followed a study from the city of São Pau-lo18 because the survey described only two age strata.
Prevalence estimates of cirrhosis considered three etio-logic categories: “hepatitis B”, “hepatitis C” and “non-viral cirrhosis”. For the first two categories, prevalence estimates of hepatitis B and C from the survey were used. After the consensus conference, it was decided that approximately 30% of HBsAg positive patients would represent cases of chronic active hepatitis and about 20% of these would develop cirrhosis. It was then decided that 6% of HBsAg positive patients in the survey would represent cases of cirrhosis. For hepatitis C, the same consensus established that 70% of anti-HCV positive patients would represent chronic hepatitis cases and approximately 20% would result in cirrhosis. This way, it was decided that 14% of anti-HCV positive patients would represent cases of cirrhosis.
Fractional contribution of each etiology of cirrhosis was defined according to previous cirrhosis national inquiry conducted by the Brazilian Society of Hepatology in 2001 (data not published). This inquiry found that approximately 37% of cases of cirrhosis in Brazil were derived from hepatitis C and 11% from hepatitis B. Thus, it was considered that cirrhosis of viral origin represented 48% of all cirrhosis cases in Brazil, with the remainder (52%) being due to alcohol and other causes of cirrhosis (non-viral cirrhosis). For this later category, age and gender distribution was based on the distribution of fatalities from alcoholic cirrhosis in SIM in the period of study.
Life expectancy used in this study was 80 years for men e 82.5 years for women. A discount rate of 3% was applied in YLL, YLD, and DALY estimates, according to the Global Burden of Disease original methodology.14 Age-weighting was not incorporated in this study, since it seems to add complexity without great impact on results.19
Burden of cirrhosis due to hepatitis B and hepatitis C was included as part of burden of chronic hepatitis B and chronic hepatitis C, respectively. Burden of non-viral cirrhosis was considered as a separate category. On tables, figures and in the whole text, the term “Hepatitis B” refers to chronic hepatitis B and cirrhosis due to hepatitis B virus while “Hepatitis C” refers to chronic hepatitis C and cirrhosis due to hepatitis C virus. “Non-viral cirrhosis” includes alcoholic cirrhosis and cirrhosis due to other non-viral causes.
ResultsIn 2008, in Brazil, chronic hepatitis B and cirrhosis due to hepatitis B caused 57,380 DALYs. Chronic hepatitis C and cirrhosis due to hepatitis C were responsible for 207,747 DALYs while non-viral cirrhosis was responsible for 536,169 DALYs in the country in the same period.
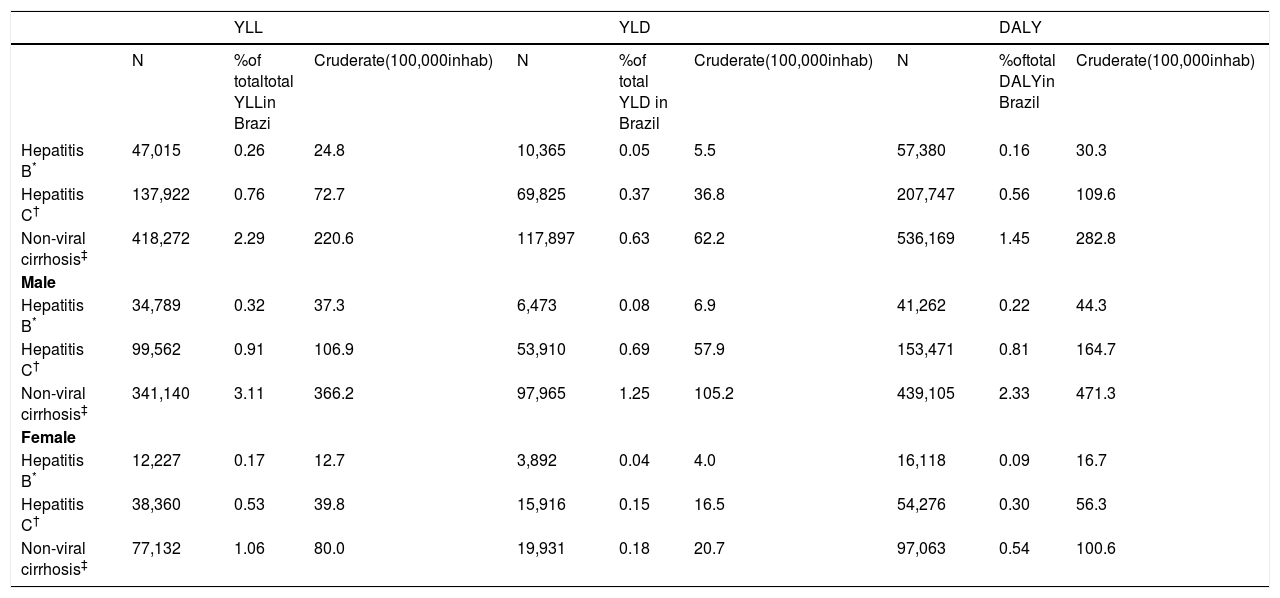
YLL, YLD and DALY attributed to each disease are displayed on Table 1, which also includes the distribution by gender of each estimate. The three conditions had the greatest proportion of DALY due to its premature mortality component (YLL). Men had higher rates of DALY, YLL and YLD in all diseases. Male/female ratio was greater in non-viral cirrhosis when compared to hepatitis B and hepatitis C, respectively: 4.42 vs. 2.83 and 2.59 for YLL; 4.92 vs. 1.66 and 3.38 for YLD and 4.52 vs. 2.55 and 2.82 for DALY. Non-viral cirrhosis was the 7th cause of YLL in men and the 19th in women. In men it was also one of the most frequent causes of YLD (17th) and DALY (11th).
Years of Life Lost (YLL), Years Lived with Disability (YLD) and Disability Adjusted Life Years (DALY) for chronic hepatitis and liver cirrhosis including distribution by gender - Brazil, 2008.
| YLL | YLD | DALY | |||||||
|---|---|---|---|---|---|---|---|---|---|
| N | %of totaltotal YLLin Brazi | Cruderate(100,000inhab) | N | %of total YLD in Brazil | Cruderate(100,000inhab) | N | %oftotal DALYin Brazil | Cruderate(100,000inhab) | |
| Hepatitis B* | 47,015 | 0.26 | 24.8 | 10,365 | 0.05 | 5.5 | 57,380 | 0.16 | 30.3 |
| Hepatitis C† | 137,922 | 0.76 | 72.7 | 69,825 | 0.37 | 36.8 | 207,747 | 0.56 | 109.6 |
| Non-viral cirrhosis‡ | 418,272 | 2.29 | 220.6 | 117,897 | 0.63 | 62.2 | 536,169 | 1.45 | 282.8 |
| Male | |||||||||
| Hepatitis B* | 34,789 | 0.32 | 37.3 | 6,473 | 0.08 | 6.9 | 41,262 | 0.22 | 44.3 |
| Hepatitis C† | 99,562 | 0.91 | 106.9 | 53,910 | 0.69 | 57.9 | 153,471 | 0.81 | 164.7 |
| Non-viral cirrhosis‡ | 341,140 | 3.11 | 366.2 | 97,965 | 1.25 | 105.2 | 439,105 | 2.33 | 471.3 |
| Female | |||||||||
| Hepatitis B* | 12,227 | 0.17 | 12.7 | 3,892 | 0.04 | 4.0 | 16,118 | 0.09 | 16.7 |
| Hepatitis C† | 38,360 | 0.53 | 39.8 | 15,916 | 0.15 | 16.5 | 54,276 | 0.30 | 56.3 |
| Non-viral cirrhosis‡ | 77,132 | 1.06 | 80.0 | 19,931 | 0.18 | 20.7 | 97,063 | 0.54 | 100.6 |
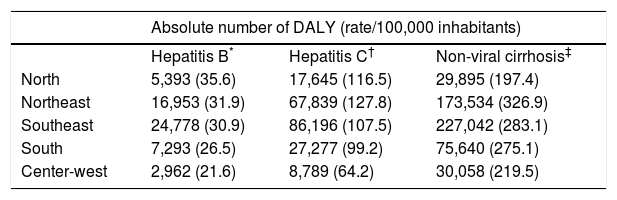
Regional distribution of DALY of chronic hepatitis and liver cirrhosis in Brazil is shown on table 2. Although the Southeast region had the highest absolute numbers of DALY for hepatitis B, hepatitis C and cirrhosis, the highest rates were observed in the North region for hepatitis B and in the Northeast for hepatitis C and non-viral cirrhosis.
Regional distribution of Disability Adjusted Life Years (DALY) for chronic hepatitis and liver cirrhosis – Brazil, 2008.
| Absolute number of DALY (rate/100,000 inhabitants) | |||
|---|---|---|---|
| Hepatitis B* | Hepatitis C† | Non-viral cirrhosis‡ | |
| North | 5,393 (35.6) | 17,645 (116.5) | 29,895 (197.4) |
| Northeast | 16,953 (31.9) | 67,839 (127.8) | 173,534 (326.9) |
| Southeast | 24,778 (30.9) | 86,196 (107.5) | 227,042 (283.1) |
| South | 7,293 (26.5) | 27,277 (99.2) | 75,640 (275.1) |
| Center-west | 2,962 (21.6) | 8,789 (64.2) | 30,058 (219.5) |
Figures 1 to 3 are mosaic plots of DALY for hepatitis B, hepatitis C and non-viral cirrhosis, respectively. These mosaic plots are divided into rectangles which represent the proportion of DALY according to gender (on the left of x-axis) and the distribution of YLL and YLD (on the right of the x-axis). Vertical lengths of each rectangle are proportional to the proportion of each age strata in each level of the x-axis. For hepatitis B, hepatitis C and non-viral cirrhosis, the greatest proportion of DALY was in the age group of 45-59 years, followed by the age group of 30-44 years. Male preponderance occurred in all age groups. DALY had a greater contribution of YLL in all diseases analyzed. For hepatitis B, the proportion of YLD decreased progressively as age groups rose. For hepatitis C, the proportion of YLD was higher in the age groups of 15-29 and 30-44 years. For non-viral cirrhosis, the proportion of YLD rose until the age group of 45-59 years, descending progressively thereafter.
 distribution according to gender, the proportion of Years of Life Lost (YLL) and Years Lived with Disability (YLD) and age groups (bars width indicate the proportion of each age group).")
Chronic hepatitis B and cirrhosis due to hepatitis B – Brazil, 2008: Disability Adjusted Life Years (DALY) distribution according to gender, the proportion of Years of Life Lost (YLL) and Years Lived with Disability (YLD) and age groups (bars width indicate the proportion of each age group).
 distribution according to gender, the proportion of Years of Life Lost (YLL) and Years Lived with Disability (YLD) and age groups (bars width indicate the proportion of each age group).")
Chronic hepatitis C and cirrhosis due to Hepatitis C – Brazil, 2008: Disability Adjusted Life Years (DALY) distribution according to gender, the proportion of Years of Life Lost (YLL) and Years Lived with Disability (YLD) and age groups (bars width indicate the proportion of each age group).
 distribution according to gender, the proportion of Years of Life Lost (YLL) and Years Lived with Disability (YLD) and age groups (bars width indicate the proportion of each age group).")
Figure 4 shows rates of YLL, YLD and DALY according to age group for hepatitis C, hepatitis B and non-viral cirrhosis. In each panel, the curves of non-viral cirrhosis reach a maximum rate at the age group of 45-59 years while the curves of hepatitis C have their greatest rate at ages 60-69. Curves of hepatitis B are flatter and do not have a “peak”, although rates rise after ages 30-44.
, Years Lived with Disability (YLD) and Disability Adjusted Life Years (DALY) according to age groups for Hepatitis B,* Hepatitis C† and non-viral cirrhosis‡. Brazil, 2008. * Includes chronic hepatitis B and cirrhosis due to hepatitis B. †Includes hepatitis C and cirrhosis due to hepatitis C. ‡Includes cirrhosis from alcohol and other non-viral causes of cirrhosis.")
Years of Life Lost (YLL), Years Lived with Disability (YLD) and Disability Adjusted Life Years (DALY) according to age groups for Hepatitis B,* Hepatitis C† and non-viral cirrhosis‡. Brazil, 2008. * Includes chronic hepatitis B and cirrhosis due to hepatitis B. †Includes hepatitis C and cirrhosis due to hepatitis C. ‡Includes cirrhosis from alcohol and other non-viral causes of cirrhosis.
In the age group of 30-44 years, non-viral cirrhosis was the 5th cause of YLL in men and the 10th in women. It was also the 8th cause of DALY in men of this age group. In men of the following age strata (45-59 years), it was the 3rd cause of YLL, 8th of YLD and 5th of DALY. In the age group of 60-69 years, non-viral cirrhosis was the 8th cause of YLL and DALY in males.
DiscussionThis is the first study that evaluates liver disease in Brazil applying the concept of DALY and the results show their burden in 2008 was significant. Chronic hepatitis B and C, cirrhosis related to these viruses and cirrhosis due to alcohol and other causes accounted for 801,296 DALYs, which represented 2.17% of total DALYs in the country. In the Global Burden of Disease Study in 2010,20 cirrhosis accounted for 1.2% of global DALY.
Most of the burden of hepatitis B, hepatitis C and non-viral cirrhosis in Brazil was due to the premature mortality component of DALY, a finding similar to that observed in the Global Burden of Disease Study 2010.6,20,21 A study in Spain22 also found that most burden of disease attributed to hepatitis B and hepatitis C in 2006 had a greater contribution of premature death than of disability. This is probably related to the natural history of both viral hepatitis and liver cirrhosis.8,10,11 Chronic viral hepatitis may have a long asymptomatic phase before progression to chronic liver disease, cirrhosis and hepatocellular carcinoma, which ultimately lead to death.10,11 Liver cirrhosis has a compensated phase, which is asymptomatic and longer than the decompensated phase (median of more than 12 years and approximately 2 years respectively).8
Male preponderance was observed in all three diseases with the greatest male:female ratio in non-viral cirrhosis.
This reflects a higher prevalence in men of risk factors for viral hepatitis or cirrhosis.23-25 Injection of illicit drugs, an important risk factor for viral hepatitis, is more prevalent in male gender.24,25 In all regions of the world, consumption of alcohol is greater in men than in women.23,26 In ECDB-2008, alcohol abuse and dependence was an important cause of DALY in men.27
Another important result in this study is the higher burden of disease in young or middle-age individuals. Some studies suggest that in countries where the main risk factor for HCV infection is injection drug use, younger ages at time of infection are observed.4,5 When nosocomial and blood products sources of infection are the most common risk factors, the bulk of infection occurs at older age.4,5 Blood transfusion and use of illicit drugs are recognized as important risk factors for viral hepatitis in Brazil, but the contribution of each factor is not known.28-30 A study on mortality of viral hepatitis in the United States found that in 2007 most deaths related to hepatitis B and hepatitis C occurred in patients aged 45 to 54 and 55 to 64, respectively.31
DALYs had an uneven regional distribution in Brazil. The southeast region, which is the most populated and urbanized region of the country, had the highest absolute numbers of DALY for hepatitis B, hepatitis C and non-viral cirrhosis. The highest rates, however, were observed in the North and Northeast, which are less developed and lower income regions. This might reflect differences in access to healthcare system and probably later diagnosis and treatment, for instance. Additionally, the North region has the highest prevalence of hepatitis B in the country.1,28
In the Global Burden of Disease Study 2010, cirrhosis was analyzed in four etiologic categories: “hepatitis B”, “hepatitis C”, “alcohol” and “other causes”20. ECDB-2008, however, considered only three etiologic categories for cirrhosis, since “alcohol” and “other causes” could not be analyzed separately, due to lack of information on sex and age distribution of the latter. While “hepatitis B”, “hepatitis C” and “alcohol” contributed with similar proportions to the burden of cirrhosis globally,20 the category “non-viral cirrhosis” accounted for approximately two thirds of the burden of liver disease in Brazil. Since the category “non-viral cirrhosis” is composed mainly of cases of alcoholic cirrhosis, results highlight the importance of alcohol as a risk factor for liver disease in Brazil. According to the World Health Organization,23 alcohol-attributable fractions for liver cirrhosis in Brazil is 62.6% for men and 60.2% for women.23 In 2008, alcohol abuse and dependence accounted for 1,1 million DALYs in Brazil, being the second, third and sixth cause of DALY in men in the age ranges of 15-29, 30-44 and 45-59, re-spectively.27 This way, alcohol seems to be the leading cause of cirrhosis in Brazil, although globally hepatitis C is considered the main etiology of end-stage liver disease.10
Due to paucity of data, neither hepatitis D virus infection nor coinfection of hepatitis B, hepatitis C and HIV were included in this study. Another disease not included in ECDB-2008 was hepatocellular carcinoma, which might have caused underestimation of deaths from viral hepatitis and cirrhosis. Other burden of disease studies have included this neoplasm in their analysis. García-Fulgueiras, et al.22 included hepatocellular carcinoma in their strategy to estimate burden of viral hepatitis in Spain. In GBD 2010, liver cancer mortality was analyzed in separate categories according to the etiology involved (hepatitis B, hepatitis C, alcohol and other).6
Non-alcoholic steatohepatitis (NASH) has been recognized as an important cause of cirrhosis and has increased in frequency recently.32,33 However, neither ECDB-2008 nor GBD 2010 specifically estimate cirrhosis from NASH, which is probably included in the category “other causes of cirrhosis” in these studies. Methodological strategies to estimate cirrhosis from NASH should be developed.
This study has some limitations that need to be discussed. The paucity of populational based studies on the epidemiology of liver diseases in Brazil is an important limitation to estimate the burden of these diseases in the country. Some diseases could not be included, as was mentioned above. Furthermore, prevalence estimates of hepatitis B and C were based on a national survey performed in capital cities of Brazil between 2005 and 2009.16 There are at least three reasons why this strategy could have compromised accuracy of data. First of all, the pool of liver disease at a certain time reflects viral infection in the past.34 In this context, data from a cross-sectional study on viral hepatitis such as this survey might not directly reflect the current prevalence of liver disease, since there is a significant interval between onset of infection and advanced liver disease.34 Furthermore, eventual differences in prevalence estimates between rural and urban areas could not be assessed since the survey was performed only in capital cities. Urban areas seem to have a higher prevalence rate of hepatitis C, for instance.35Additionally, general population surveys underestimate the true prevalence of hepatitis C, since groups with a higher risk of infection are not included in these studies.36 Therefore, the methodological approach applied in this study might have underestimated the true burden of liver disease in the country. However, the strategy used was conservative and is still representative of the epidemiology of liver disease in Brazil.
In conclusion, the present study shows that hepatitis B, hepatitis C and non-viral cirrhosis are responsible for a significant proportion of DALY in Brazil, affecting individuals still in their productive years, specially men. Non-viral causes of cirrhosis, which have a major contribution of alcohol, accounted for the greatest proportion of burden of liver disease in the country. Results could guide policies towards earlier diagnosis and effective treatment of these diseases. Furthermore, this study will allow future comparative analysis of the burden of liver disease in Brazil, showing trends over time and also the impact of interventions such as new treatment for hepatitis C.
Abbreviations- •
anti-HCV: antibody to hepatitis C virus.
- •
DALY: disability adjusted life years.
- •
ECDB-2008: Estudo de Carga de Doença no Brasil – 2008 (Brazilian Burden of Disease Study for the year 2008).
- •
GBD: global burden of disease.
- •
HBsAg: hepatitis B surface antigen.
- •
ICD-10: tenth version of the International Classification of Diseases.
- •
NASH: non-alcoholic steatohepatitis.
- •
SIM: Sistema de Informação de Mortalidade (Brazilian Mortality Information System).
- •
YLD: Years Lived with Disability.
- •
YLL: Years of Life Lost.
We would like to thank Angelo Alves de Mattos, Francisco José Dutra Souto, Henrique Sérgio Moraes Coelho e Jorge André de Segadas-Soares for participating in the consensus meeting organized for this project. We would also like to acknowledge Leila Maria Beltrão Pereira for providing detailed information on the viral hepatitis survey.
Financial SupportECDB-2008 was funded by Science and Technology Department of Brazilian Ministry of Health.
DISCLOSURE
Authors do not have any disclosure to report.



