








We present our experience in the reconstruction of cerebrospinal fluid (CSF) leaks according to their size and location.
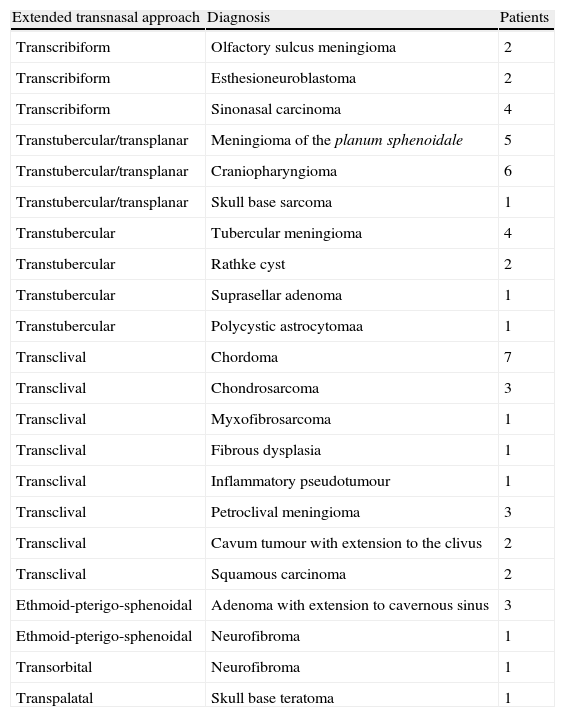
Materials and methodsFifty-four patients who underwent advanced skull base surgery (large defects) and 62 patients with CSF leaks of different origin (small and medium-sized defects) were included. Large defects were reconstructed with a nasoseptal pedicled flap positioned on fat and fascia lata and lumbar drainage was used. In small and medium-sized leaks of other origin, intrathecal fluorescein 5% was applied previously to identify the defect. Fascia lata in an underlay position was used for reconstruction, which was then covered with mucoperiosteum from the turbinate. Perioperative antibiotics were administered for 5–7 days. Nasal packing was removed after 24–48h.
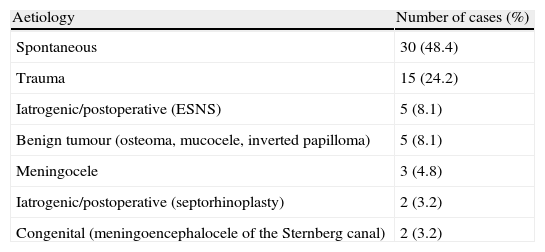
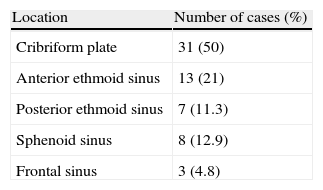
ResultsThe most frequent aetiology for small and medium-sized defects was spontaneous (48.4%), followed by trauma (24.2%), iatrogenic (5%) and then others. The success rate was of 91% after the first surgery and 98% in large skull base defects and small/medium-sized respectively. After rescue surgery, the rate of closure achieved was 100%. The follow-up was 15.6±12.4 months for large defects and 75.3±51.3 months for small/medium-sized defects without recurrence.
ConclusionsEndoscopic surgery for closure of any type of skull base defect is the gold standard approach. Defect size does not play a significant role in the success rate. Fascia lata and mucoperiosteum allow a reconstruction of small/medium-sized defects. For larger skull base defects, a combination of fat, fascia lata and nasoseptal pedicled flaps provides a successful reconstruction.
Presentamos nuestra experiencia en el cierre de fístulas de líquido cefalorraquídeo según su tamaño y localización.
Material y métodoSe incluyeron 54 pacientes con tumores de base de cráneo intervenidos mediante cirugía endoscópica (defectos grandes) y 62 pacientes con fístulas de otra causa (defectos pequeños y medianos). Los defectos grandes fueron reparados con un colgajo nasoseptal previa colocación de grasa y fascia lata y drenaje lumbar. En las fístulas de otra causa se aplicó fluoresceína al 5% intratecalmente para identificar la fístula. Para su reconstrucción utilizamos la fascia lata en posición underlay recubierta por un injerto mucoperióstico del cornete. Se retiró el taponamiento a las 24-48h y se administró ceftriaxona durante 5-7 días.
ResultadosLa etiología más frecuente fue la espontánea (48,4%), seguida de la traumática (24,2%), la iatrogénica (5%) y otras. La tasa de éxito en la primera cirugía fue del 91% en los defectos grandes y del 98% en los pequeños. Con la cirugía de rescate la tasa asciende al 100%. El seguimiento a largo plazo fue de 15,6±12,4 meses para los defectos grandes y de 75,3±51,3 meses para los pequeños, sin evidencia de recurrencias.
ConclusiónLa cirugía endoscópica es segura y eficaz en el cierre de los defectos de base de cráneo con o sin fístula activa. El tamaño del defecto juega un papel menor en el resultado. La fascia lata y el mucoperiostio del cornete son suficientes para la reparación de las fístulas pequeñas y medianas, mientras que se prefieren los colgajos nasoseptales para los defectos grandes.