



Air and surfaces in the hospital environment are a potential source of exposure to filamentous fungi (FF) that could cause invasive fungal diseases (IFD) in severely immunocompromised patients. The prevalent FF in IFD are species from the genera Aspergillus, Fusarium, Scedosporium, and those within the order Mucorales. We have compiled regulations and described the procedures used in the clinical mycology laboratory to assess the presence of FF in areas at risk for the development of IFD. The infection control committees of each establishment implement hospital policies to regulate and control processes aimed at preventing infections. Fungal load monitoring is an important step in this process to validate air quality in order to ensure a clean and protected environment for severely immunocompromised patients.
El aire y las superficies en el ambiente hospitalario son una fuente potencial de exposición a hongos filamentosos (HF) que pueden causar enfermedades fúngicas invasivas (EFI) en pacientes con inmunocompromiso grave. Los HF prevalentes en EFI son especies que pertenecen a los géneros Aspergillus, Fusarium, Scedosporium y los del orden Mucorales. Recopilamos regulaciones y describimos procedimientos que se utilizan en el laboratorio de micología clínica para evaluar la presencia de HF en el ambiente de áreas de riesgo para el desarrollo de EFI. El comité de control de infecciones de cada establecimiento implementa políticas hospitalarias destinadas a regular y controlar procesos para prevenir infecciones. La monitorización de la carga fúngica es un eslabón en esta cadena y está dirigida a validar la calidad del aire, con el fin de asegurar un entorno limpio y protegido para el paciente.
Air and surfaces of the hospital environment are a potential source of exposure to filamentous fungi (FF) that can cause invasive fungal disease (IFD) in severely immunocompromised patients. In recent years, the frequency of IFD caused by FF has increased as a result of advances in medicine, the use of more aggressive treatments, hematopoietic progenitor cell or solid organ transplantation, chemotherapeutic treatments, and the use of immunomodulatory agents. The prevalent FF species associated with IFD belong to the genera Aspergillus, Fusarium, Scedosporium and those of the order Mucorales2,15.
These fungal infections may be acquired during prolonged hospital stays due to the increase of fungal spores in the environment, which is attributable to multiple causes, such as construction works in the area of the facilities or its surroundings1,10,11,13. The role of the clinical mycology laboratory in monitoring environmental fungi involves a complex and laborious practice that requires interdisciplinary work, sample collection planning, processing strategies, and interpretation of results.
In this report, we describe the procedures used to assess the presence of FF in the environment of hospital areas considered to be at risk for the development of IFD.
The areas in the health centers are standardized into categories based on their clean air requirements, which vary depending on the clinical characteristics of the patients and the activities performed. These areas are designed based on an appropriate building structure, specific equipment, and ventilation systems that maintain controlled environmental parameters to achieve low levels of contamination. The filtered air that flows into the environment should circulate from the clean areas (higher safety areas for the patients) to the unclean areas (lower safety areas)14.
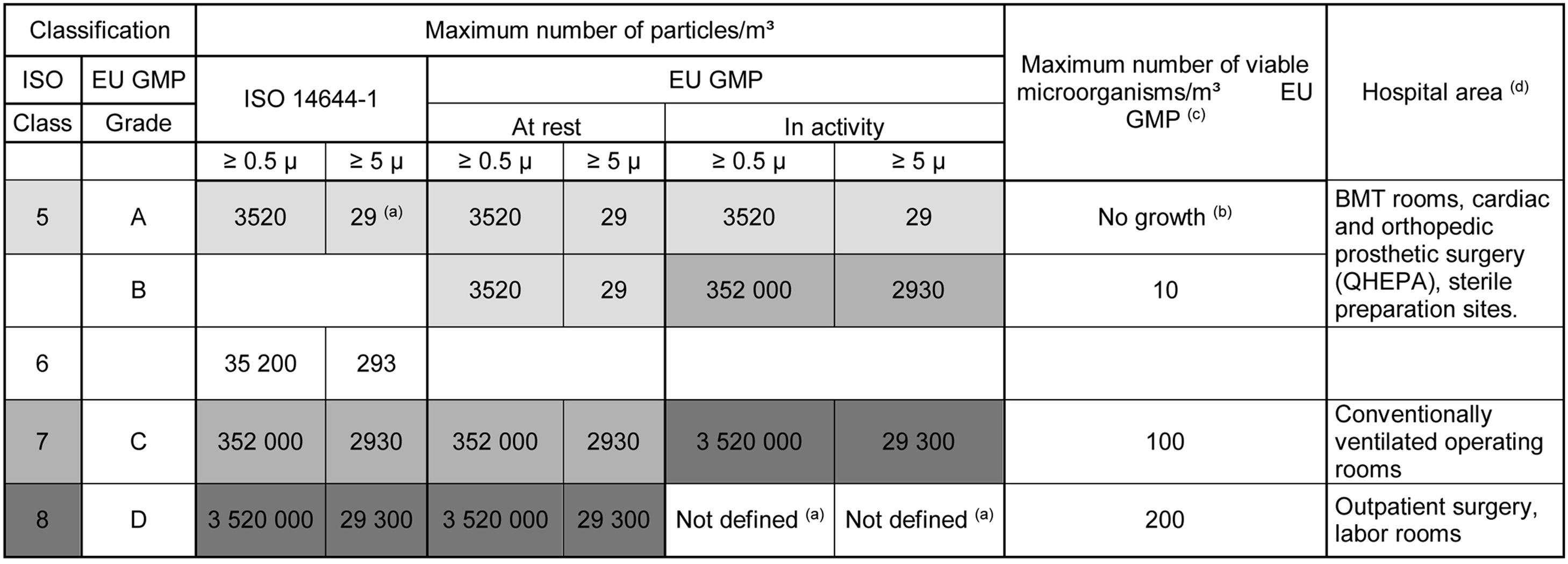
To validate these rooms, it is necessary to monitor the quality of the air circulating within them. There are international standards that classify air quality; however, it is important to note that acceptable levels of airborne microorganisms may vary based on guidelines and regulations established by health authorities. The International Organization for Standardization (ISO) standard validates the operability of clean rooms based on the count of airborne particles by their size in μ/m3 of air, known as ISO 14644-1, which includes classes ranging from ISO 1 (aseptic area) to ISO 9 (less clean air)8. The European Union regulations detailed in the Guide to Good Manufacturing Practice (EU GMP) classify clean rooms into grades A, B, C and D3, depending on the level and size of particles/m3 of air, viable microorganisms/m3 of air and the activity in the area.
Table 1 shows a comparison of the classification of clean areas according to both international standards. The concordance between them is observed not only in terms of the maximum count of particles allowed but also in its relationship with the number of viable microorganisms/m3 and the corresponding hospital area5. The maximum accepted level for particles and microorganisms is established for each type of room. When these values are reached, a follow-up alert is generated; however, if they are exceeded, prompt corrective measures must be implemented3.
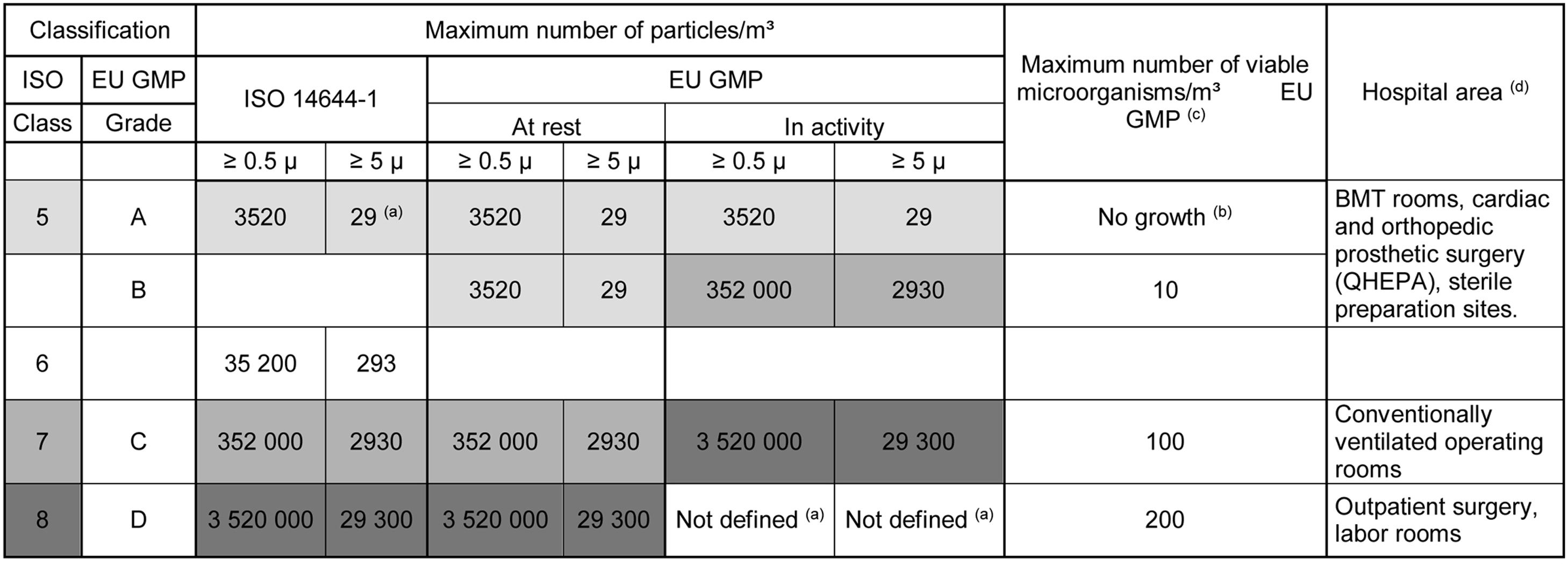
BMT: bone marrow transplantation; ISO: International Organization for Standardization; EU GMP: European Union Guide to Good Manufacturing Practice.
The concordances between the two standards are indicated by the same color. At rest: monitoring is carried out with the room empty after cleaning. In activity: the monitoring is carried out with the usual personnel in the area. The values indicate accepted limits of particles or microorganisms. When counts are higher than indicated, appropriate corrective action must be taken according to standard operating procedures.
(a) At grade D, the operational limits are not predetermined. Criteria are set by each institution based on risk assessment and routine data.
(b) Any growth indicates the need for an evaluation of the monitored area to implement corrective measures.
(c) The maximum number of viable microorganisms/m3 is specified only by the EU GMP standard for Recommended Microbial Contamination Limits.
(d) The last and fourth column indicates the specific hospital area classified depending on the clean air requirement based on its activity according to the standards.
In Argentina, the National Single Central Institute for Ablation and Implant Coordination (INCUCAI, as per its acronym in Spanish)6,7 is the organism that regulates the processes that ensure the quality of good hospital practices and specifies the necessary infrastructure requirements for rooms used for cell and/or tissue bank processing, as well as rooms for patients undergoing autologous and allogeneic hematopoietic progenitor cell transplantation. In addition, INCUCAI outlines environmental microbiological control measures and their frequency in response to specific situations7.
Areas for monitoring include:
- (a)
Rooms for immunocompromised patients undergoing bone marrow transplantation (BMT) with neutropenia (≤100cells/mm3) and an expected duration of ≥1 week. These rooms are equipped with HEPA filters (99.97% efficiency for particles of 0.3μm) with recirculation, positive air pressure (>2.5Pa, ideally >8Pa), >12air changes/hour, and airflow direction from clean to unclean areas14. In these rooms only FF is assessed. Several air intakes are performed, including below the laminar flow that filters air with high efficiency (grade A/ISO class 5), at the patient's bedside headboard/feet, in corners adjacent to the laminar flow (empty grade B/ISO class 5) at the air entrance and exit areas of the room. In the bathroom (grade C/ISO class 7) air intake procedures should be conducted both before and after using the shower, leaving it open for at least 5min. The search for airborne FF is complemented with swabs of wet surfaces, such as shower heads, faucet spouts, bathtub, sink and bidet drains1,12.
- (b)
Tissue and cell banks (TCB) where materials are manipulated in accordance with air quality and cleanliness standards.
- (c)
Operating rooms equipped with high-efficiency HEPA air filter cabinets (QHEPA) where orthopedic or cardiovascular prosthetic implant surgeries are performed, and material for the bone bank is fractionated9.
- (d)
Hospital pharmacy sectors (HOP) where sterile solutions for high-risk medications (dangerous drugs) are prepared.
In the cases of TCB, QHEPA, HOP, the air within the high-efficiency cabinets in operation (grade A/ISO class 5) and in the work area around the cabinets are evaluated, considering the air flow circulation (grade B empty/ISO class 5).
- (e)
Critical care units, burn units and conventional operating rooms will be monitored in specific situations, such as outbreak studies to identify an environmental source, suspicion of surgical site infections, modification of cleaning protocols, building constructions, remodeling and/or repairs, cleaning of ventilation ducts, and before enabling operating theaters9.
In addition to FF, mesophilic bacteria are assessed in TCB, QHEPA, HOP, and conventional operating rooms.
If during monitoring something out of the cleaning standard is observed, the surfaces will be evaluated.
The procedures include:
- (1)
Environmental sampling planning. The following must be considered to design and establish the sampling sites: the ventilation flow (air inlet and outlet direction), the area where the patients are or will be located, and the activity and circulation of staff. A thorough and careful examination of the entire room must be conducted, including walls, windows, inside closets, and vertical surfaces hidden behind furniture, in search of moisture stains or reservoirs that could harbor fungi.
- (2)
Measurement of non-viable particles is an important component of preventive maintenance as it is a measure of the degree of contamination of the site and is considered “real time” data. This service is provided by companies specialized in environmental biosafety and is supervised by the hospital bioengineering sector. A laser counter is used to indicate the total number of particles classified by size from 0.3 to 10μ/m3 of air. If the measurement exceeds the site's particulate standard, immediate action must be taken to correct the deviation3,9.
- (3)
Measurement of viable particles. The transmission of airborne conidia depends on the dispersal characteristics of the fungus. In the case of Eurotiales conidia, such as Aspergillus, which have hydrophobic behavior, they are easily released, dispersed and maintained by flotation in the air11. Hypocreales conidia (e.g. Fusarium spp.), as they are viscous, remain suspended in the air for less time and are distributed in the environment by adhering to objects or drops of humidity; therefore, their search must be complemented with surface swabs from humid places1.
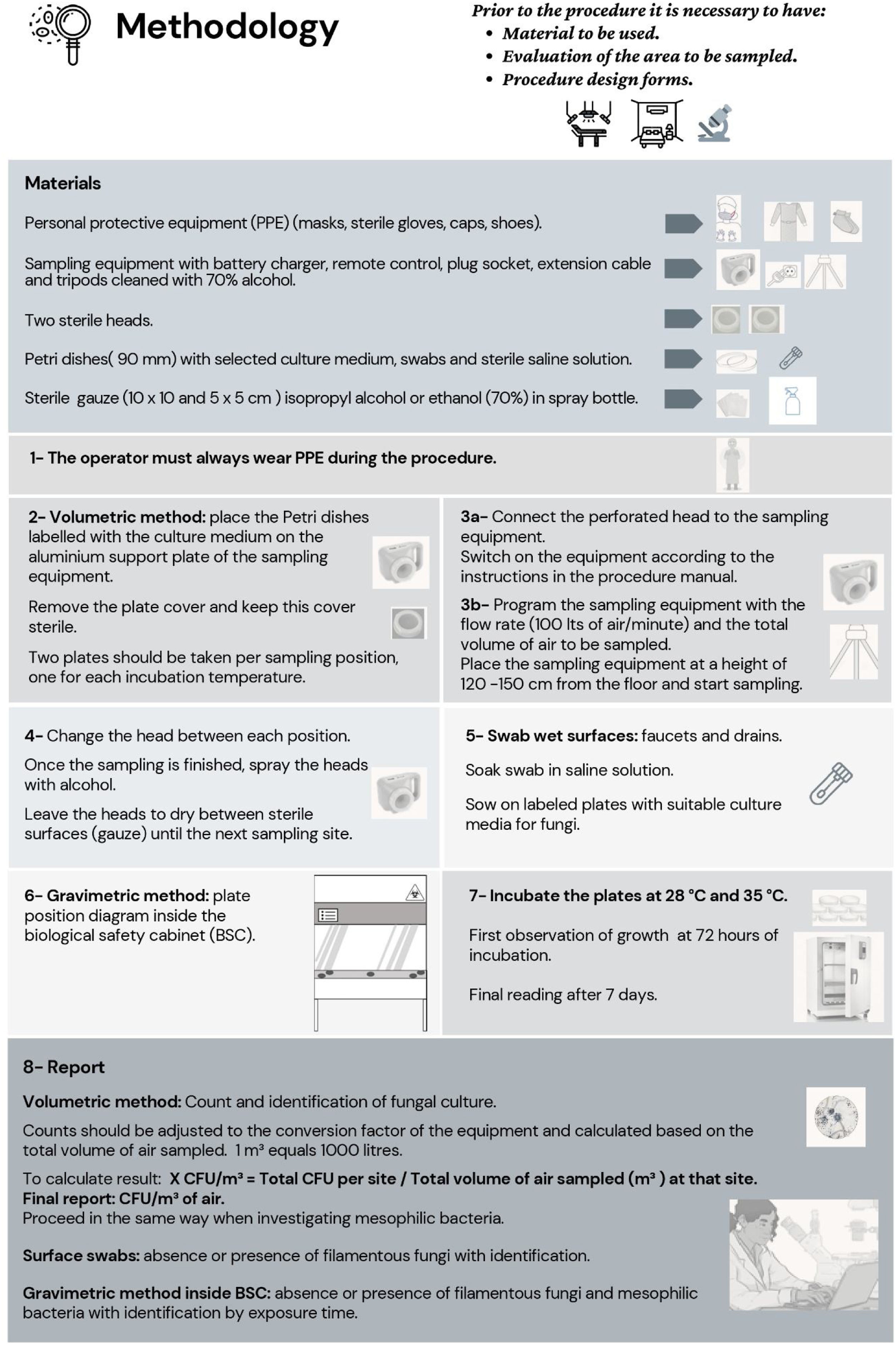
The measurement of viable particles can be done by either the sedimentation or gravimetric method (passive) or volumetric method (active).
- (3a)
Gravimetric method: bioaerosols deposit by gravity, depending on the size of the spores according to the Lewis–Stokes equation14. Suspended particles in the air ≥5μ are deposited, while those ≤5μ float due to their aerodynamic behavior. For example, conidia of Aspergillus section Fumigati have a small diameter, ranging from 2 to 3μ. In addition to their hydrophobic characteristic, they are rough on the external surface, which increases their floating time and allow them to remain suspended in the air for prolonged periods.
- -
It is useful for monitoring inside a biological safety cabinet where filtered air is blown in a vertical laminar fashion at a constant velocity (grade A/ISO class 5). In these cabinets, uncovered 90mm Petri dishes with appropriate culture media for the development of FF and mesophilic bacteria are used; these are placed in 5 or 6 positions (Fig. 1) for a time ranging from 1h to no more than 4h5.
- -
This method is not recommended in larger sites such as rooms and operating theater suites (grades B/C/D) because it does not represent the real environmental fungal load14.
- -

Accompanied by surface sampling, either with swabs or touch plates, the gravimetric method could be a transitional alternative in institutions that do not have access to the volumetric method. However, we emphasize that their results do not provide a real assessment of the aerial fungal biota.
- (3b)
The volumetric method is performed using an air sampling equipment that works with a reverse ventilator that sucks and impels a specified air flow. The most used flow rate is 100l/min (Fig. 1).
Devices vary depending on the way the air impacts; this impact can be perpendicular or tangential. The most commonly used devices are those with perpendicular (orthogonal) impact. In these systems, the aspirated air passes through a perforated head with multiple holes that impact the surface of a plate containing a culture medium.
There are several types of equipment, each with different efficiency levels, some equipped with a tripod and remote control. When acquiring or renting this equipment, it is important to consider that the head is adapted to contain 90mm plates, which is the standard size for Petri dishes. If the equipment has two independent heads, this will speed up the sampling process. The heads are sterilized in an autoclave (wet steam).
These devices require annual calibration (preventive maintenance) to certify the volume of air aspirated per minute. The sampling height for the equipment should be between 1.2 and 1.5m from the floor.
The air volume to be sampled at each position ranges between 250, 500, and 1000l, depending on the estimated degree of contamination in the area to be sampled. In all cases the planning should include a prior control sampling to assess the quality of the air and better define the sampling design in terms of the volume of air to be sampled.
In clean environments (rooms grade C/D, ISO class 7/8), 250–500l should be aspirated per position, while in very clean or ultra clean environments (rooms grade A/B, ISO class 5), 500–1000l should be aspirated per position. It is not advisable to sample a larger volume per plate because it will dehydrate the culture medium used. The total volume sampled per site should be representative of the total volume of that environment. On average, this would correspond to an average of 4000–6000l (40–50% of the air in the site)14.
- (4)
Surface sampling is performed using a swab moistened in sterile saline solution. This practice always applies when the sampling is carried out in BMT rooms for humid surfaces and/or when irregular situations of cleanliness or humidity stains are observed in any of the abovementioned rooms. The swabs are transported in properly labeled sterile tubes. If cultivation for FF is not done immediately, these tubes should be kept refrigerated until processed.
Culture media and temperature conditions: selective culture media such as Sabouraud agar or malt agar with added antibiotics are used. In the latter, colonies develop with a reduced diameter and adequate fructification, allowing better visualization for counting and microscopic observation.
The optimum incubation temperature for the growth of most environmental FF is 28–30°C.
To investigate the presence of thermotolerant species such as Aspergillus section Fumigati, Scedosporium spp. or Fusarium spp. it is advisable to incubate at 35–37°C; therefore, 2 intakes (plates) per position should be collected, one for each temperature4.
Outcome record: a preliminary report is conducted after 72h of incubation, and the final incubation time is 7 days. The final report is prepared based on the methodology available for the identification of the isolates. The results are expressed in colony forming units (CFU) (Fig. 1). In the gravimetric method, the CFU count per plate exposure time is reported. In the volumetric method, the count is expressed in CFU/m3 of air. For surface sampling swabs indicate the absence or presence of FF with its identification.
When the colony count is performed, this number must be adjusted with a correction factor, which varies depending on the efficiency of the sampler. Each equipment has the corresponding conversion table in the instruction manual.
After 72h of incubation, colony development should be carefully evaluated to prevent the spread of conidia. If Aspergillus spp., Fusarium spp., Scedosporium spp. and/or Mucorales are suspected, a preliminary identification should be conducted, and the count reported immediately. This information will allow prompt corrective decisions, such as the verification of the state of the ventilation system, infrastructure, cleanliness, area activity, among others. After 7 days of incubation, the final count is performed. Reports should include the area of origin, the time of sampling, and important considerations such as whether the sampling was taken when the area was empty or occupied, whether the activity was normal or not, whether it was done before or after daily cleaning.
When the search for mesophilic bacteria is required, it is advisable to use nutrient agar and the count will be carried out after 48h, indicating the number of CFU/m3 of air and the identification of the colonies.
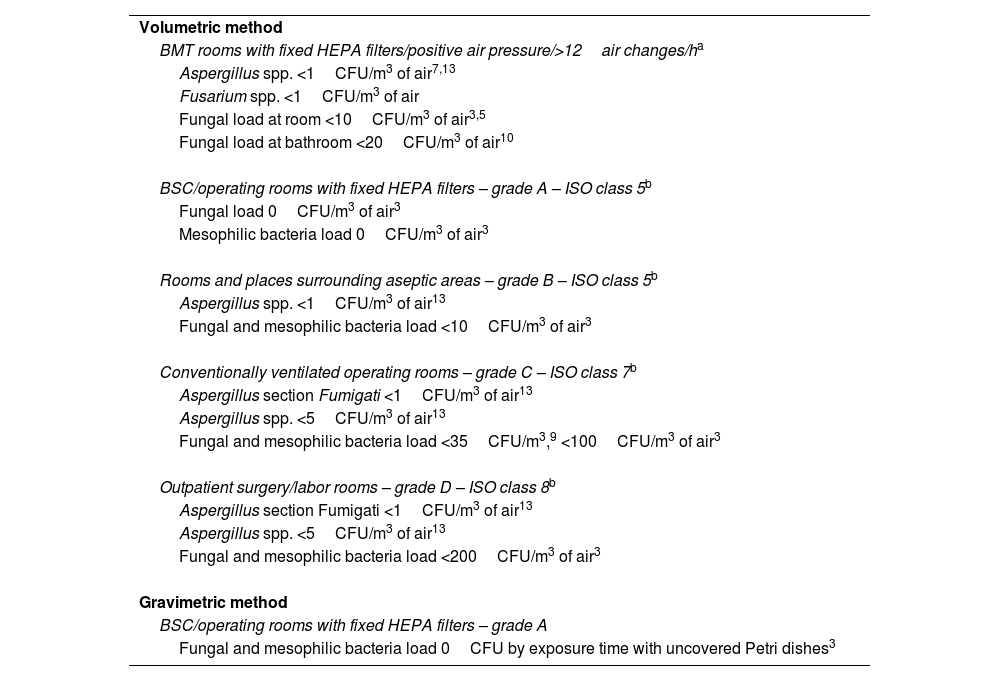
Table 2 shows criteria for the evaluation of results for their interpretation according to the air quality requirements of the site, based on the EU GMP3,5, on guidelines9,13, and on published works from different experiences10.
Recommended values for the interpretation of air monitoring results.
| Volumetric method |
| BMT rooms with fixed HEPA filters/positive air pressure/>12air changes/ha |
| Aspergillus spp. <1CFU/m3 of air7,13 |
| Fusarium spp. <1CFU/m3 of air |
| Fungal load at room <10CFU/m3 of air3,5 |
| Fungal load at bathroom <20CFU/m3 of air10 |
| BSC/operating rooms with fixed HEPA filters – grade A – ISO class 5b |
| Fungal load 0CFU/m3 of air3 |
| Mesophilic bacteria load 0CFU/m3 of air3 |
| Rooms and places surrounding aseptic areas – grade B – ISO class 5b |
| Aspergillus spp. <1CFU/m3 of air13 |
| Fungal and mesophilic bacteria load <10CFU/m3 of air3 |
| Conventionally ventilated operating rooms – grade C – ISO class 7b |
| Aspergillus section Fumigati <1CFU/m3 of air13 |
| Aspergillus spp. <5CFU/m3 of air13 |
| Fungal and mesophilic bacteria load <35CFU/m3,9 <100CFU/m3 of air3 |
| Outpatient surgery/labor rooms – grade D – ISO class 8b |
| Aspergillus section Fumigati <1CFU/m3 of air13 |
| Aspergillus spp. <5CFU/m3 of air13 |
| Fungal and mesophilic bacteria load <200CFU/m3 of air3 |
| Gravimetric method |
| BSC/operating rooms with fixed HEPA filters – grade A |
| Fungal and mesophilic bacteria load 0CFU by exposure time with uncovered Petri dishes3 |
BMT rooms: bone marrow transplant units; BSC: biological safety cabinet.
The fungal load and the isolation of other FF such as Penicillium spp., Cladosporium spp. and others, should be reported to the infection control team. Although they may not have a high impact on the development of IFD, their presence indirectly indicates a malfunction of the ventilation system, lack of building maintenance or deficiency in the performance of internal protocols.
In our personal experience, when the patient, family member or healthcare personnel are present during environmental monitoring, it may be likely that yeast fungi, such as Candida spp. and Rhodotorula spp. can be recovered.
The frequency of performing measurements of non-viable particles suggests the need to requalify areas with grades A/B within a maximum of 6 months, and in areas with grades C/D within a maximum of 12 months3,9.
The frequency of measuring airborne fungi and/or mesophilic bacteria will depend on the action policies of the infection control committee of each health center, or on the situation that requires monitoring.
In bone marrow transplant units (BMTs) grade A/ISO class 5, mycological control is recommended every 6 months3, and/or after any corrective action, or when construction work is carried out in the sector or adjacent to the ward or hospital3,7.
In operating theater suites, the monitoring frequency will depend on the grade according to the described classification.
Grade A/ISO class 5, QHEPA, TCB, HOP: each health facility will assess the monitoring frequency according to the risks, which will be at least every 6 months9.
In conventional ventilated operating rooms grade B/C/D: it is not advisable to perform systematic controls9.
Final conclusions or recommendations: we consider that the monitoring of FF spores in hospital environments is an important step in a series of actions aimed at controlling and validating processes to prevent IFD. Health centers present different degrees of complexity, infrastructure, human resources, and quality assurance systems, among others. Due to this diverse reality, we provide general recommendations for FF monitoring. It is likely that there are situations that have not been covered in this manuscript. Each institution will assess the need for environmental spores monitoring at relevant sites that pose a high risk of acquiring an IFD to the severely immunocompromised patient.
Hospital air quality control combines the monitoring of physical parameters (temperature, relative humidity, acoustic level, air movement, velocity, and pressure), the counting of airborne (non-viable) particles ≤0.5μ to ≥5μ, and a mycological study of the air to assess the environmental fungal microbiota.
Except for BMT, the hospital areas already mentioned above, which include TCB, QHEPA, HOP, are jointly monitored for FF and mesophilic bacteria3,9. Intensive care areas, burn units and conventional operating rooms lack a universally accepted standard for endpoints and interpretation of FF results; probably because these wards house patients with lower risks of IFD.
It is important to consider that the presence of any type of FF in high counts is an indicator of lack of building maintenance or deficiencies in the performance of internal protocols, thus representing a potential risk.
Since these samplings are affected by a multifactorial and complex dynamics, the criteria for the interpretation of results present variability among the standards that regulate air quality (Table 2). The procedures described are based on current regulations, international guidelines, and published works. The infection control committee of each institution, in permanent operation, oversees the actions aimed at regulating and controlling processes to prevent infections.
The monitoring of the fungal load in the hospital environment performed by the clinical mycology laboratory aims to validate hospital indoor air quality to ensure a controlled environment for immunocompromised patients to prevent fungal infections.
FundingNone declared.
Conflict of interestNone declared.
Dr. Gustavo Giusiano, Department de Micología, Consejo Nacional de Investigaciones Científicasy Tecnológicas (CONICET) --- Instituto de Medicina Regional, Universidad Nacional del Nordeste, Resistencia (Chaco) ---Argentina, for his contributions and critical review of the Manuscript.
Membersof Subcomisión de Micología Clínica, Asociación Argentina de Microbiología.
