



The purpose was to advance research and clinical methodology for assessing psychopathology by testing the international generalizability of an 8-syndrome model derived from collateral ratings of adult behavioral, emotional, social, and thought problems. Collateral informants rated 8,582 18-59-year-old residents of 18 societies on the Adult Behavior Checklist (ABCL). Confirmatory factor analyses tested the fit of the 8-syndrome model to ratings from each society. The primary model fit index (Root Mean Square Error of Approximation) showed good model fit for all societies, while secondary indices (Tucker Lewis Index, Comparative Fit Index) showed acceptable to good fit for 17 societies. Factor loadings were robust across societies and items. Of the 5,007 estimated parameters, 4 (0.08%) were outside the admissible parameter space, but 95% confidence intervals included the admissible space, indicating that the 4 deviant parameters could be due to sampling fluctuations. The findings are consistent with previous evidence for the generalizability of the 8-syndrome model in self-ratings from 29 societies, and support the 8-syndrome model for operationalizing phenotypes of adult psychopathology from multi-informant ratings in diverse societies.
El propósito fue avanzar en la metodología clínica y de investigación de la evaluación psicopatológica mediante el examen de la generalización internacional de un modelo de 8 síndromes derivados de evaluaciones de personas allegadas a adultos, en sus problemas emocionales, sociales y de pensamiento. Informantes allegados a los adultos calificaron a 8.582 residentes de 18 países entre 18 y 59 años de edad con el Adult Behavior Checklist (ABCL). Un análisis factorial confirmatorio examinó el ajuste del modelo de 8 síndromes a las puntuaciones provenientes de cada país. El índice primario de ajuste del modelo (RMSEA) mostró un buen ajuste del modelo para todas las sociedades, mientras que índices secundarios (TLI, CFI) mostraron un ajuste de aceptable a bueno para 17 países. Las cargas factoriales fueron robustas a través de los países e ítems. Los hallazgos son consistentes con evidencia previa existente para la generalización del modelo de 8 síndromes en autoinformes de 29 sociedades. Además, los resultados respaldan el modelo de 8 síndromes para operacionalizar fenotipos de psicopatología del adulto provenientes de evaluaciones de múltiples informantes en diversas sociedades.
Globalization is a theme of our times. World communities are becoming increasingly diverse as traditional boundaries between societies are changing. Mental health professionals increasingly need clinical constructs and methods for operationalizing such constructs that can be used with people of many different backgrounds.
One approach is to define constructs on the basis of experts’ knowledge and judgments, as exemplified by the American Psychiatric Association's (2013)Diagnostic and Statistical Manual (DSM) and the World Health Organization's (2010)International Classification of Disease (ICD). A second approach derives constructs from statistical analyses of problems reported for samples of individuals. This approach can be applied to various kinds of data, including experts’ judgments of individuals’ problems. An early example is Wittenborn's (1951) factor analysis of psychiatrists’ and nurses’ ratings of U.S. inpatients on 55 symptoms, which yielded nine syndromes resembling diagnostic constructs of that era.
The statistical approach can also be applied to self-reported problems. As an example, Goekoop et al. (1992) derived five factors from exploratory factor analysis (EFA) of 192 Dutch outpatients’ interview reports regarding 65 items of the Comprehensive Psychopathological Rating Scale (Asberg, Montgomery, Perris, Schalling, & Sedvall, 1978). In a study of 91 UK Tourette syndrome patients, EFA of 11 self-rated personality and psychopathology measures yielded obsessionality and anxiety/depression factors (Eapen, Fox-Hiley, Banerjee, & Robertson, 2004).
The statistical approach has been used to derive syndrome constructs from a broad spectrum of problems assessed by the Adult Self-Report (ASR), which is designed for clinical, research, and epidemiological assessment of 18-59-year-olds (Achenbach & Rescorla, 2003). Literate respondents can rate its 120 problem items in about 15minutes, or it can be administered by lay interviewers. The items describe particular kinds of behavioral, emotional, social, and thought problems, which are rated 0=not true, 1=somewhat or sometimes true, or 2=very true or often true, based on the preceding 6 months. Every item had to meet at least one of the following criteria: (a) it discriminated significantly between individuals referred for mental health or substance use services versus demographically similar individuals not referred for services; (b) it was identified by international experts as being very consistent with > 1 DSM diagnostic category; (c) it loaded significantly on at least one of eight syndromes derived by EFAs and confirmatory factor analyses (CFAs) of self-ratings by 2,968 U.S. referred and nonreferred 18-59-year-olds (Achenbach & Rescorla, 2003). The syndromes are designated as Anxious/Depressed, Withdrawn, Somatic Complaints, Thought Problems, Attention Problems, Aggressive Behavior, Rule-Breaking Behavior, and Intrusive. The first three syndromes aggregate into a broad-band Internalizing scale, while the last three aggregate into an Externalizing scale, based on second-order factor analyses.
The syndrome scales scored from the ASR have been found to correlate significantly with scales of the Symptom Checklist-90-Revised (Derogatis, 1994) in a U.S. clinical sample. Most of the syndrome scales have also been found to correlate significantly with MMPI scales in a Turkish nonclinical sample (Achenbach & Rescorla, 2003). Over 100 published studies have reported use of the ASR (Bérubé & Achenbach, 2014).
Beyond self-reportsAssessment of adult psychopathology tends to rely on data obtained mainly from the person being assessed. However, reports by other informants may not agree with self-reports. For example, Meyer et al. (2001) found a mean kappa of only .18 between diagnoses based solely on adults’ self-reports versus diagnoses based on collateral reports. Meyer et al. also found that 70% of personality disorder diagnoses based on clinical interviews with adult patients were wrong when compared with diagnoses made from multiple sources of data. Furthermore, meta-analyses have yielded mean correlations between adult self- and informant-ratings of only .43 for internalizing problems (e.g., anxiety, depression) and .44 for externalizing problems (e.g., aggression, lying) (Achenbach, Krukowski, Dumenci, & Ivanova, 2005).
One method intended to overcome the limitations of self-report instruments is to use validity scales to correct for misleading self-reports. However, several reviews have concluded that validity scales do not improve the validity of results (e.g., Archer, Fontaine, & McCrae, 1998; Barthlow, Graham, Ben-Porath, Tellegen, & McNulty, 2002; McGrath, Mitchell, Kim, & Hough, 2010). In a cross-cultural study that found validity scales to reduce validity, the authors concluded that multimethod approaches are superior to validity scales, because “The best evidence on protocol validity, and the best alternative to the use of validity scales, comes from the comparison of self-report scores with independent assessments,” i.e., reports by informants who know the people being assessed (Piedmont, McCrae, Riemann, & Angleitner, 2000, p. 590). Although standardized multi-informant methods are often used for assessing child psychopathology (De Los Reyes, Thomas, Goodman, & Kundey, 2013), such methods may also improve assessment of adult psychopathology (De Los Reyes, Bunnell, & Beidel, 2013).
One way to advance standardized multi-informant assessment of adult psychopathology is to develop instruments for obtaining collateral reports that parallel self-report instruments. Accordingly, the Adult Behavior Checklist (ABCL) was developed for completion by collaterals to assess many of the same problems that are assessed by the ASR. The ABCL has counterparts of 115 of the 120 ASR problem items but omits items not likely to be ratable by informants (e.g., “heart pounding”). The ABCL also has three items that are not likely to be self-reported (e.g., “stares blankly”). Like the ASR items, ABCL items are rated 0-1-2, based on the preceding 6 months. EFAs and CFAs of ABCL ratings by collaterals of 1,660 U.S. referred and nonreferred 18-59-year-olds yielded counterparts of the eight syndromes found in ASR self-ratings (Achenbach & Rescorla, 2003). The collaterals included spouses/partners, family members, and friends. Correlations between ASR and ABCL scores were .43 for internalizing problems and .44 for externalizing problems, the same as the mean cross-informant correlations found in the meta-analyses of many instruments in many studies (Achenbach et al., 2005).
Testing syndromes in other societiesThere are multiple reasons why we cannot assume that assessment instruments developed in one society would be applicable in other societies. As an example, genetic factors affecting behavioral covariation may differ across societies (Way & Lieberman, 2010). Additionally, different behaviors may be encouraged or discouraged in different societies, leading to different groupings of behaviors across societies (Weisz, Weiss, Suwanlert & Chaiyasit, 2006).
To evaluate the applicability of assessment instruments to societies other than where they were developed, they must be used to assess large samples from those societies. To test the degree to which ratings of problems in other societies fit particular syndrome models, CFAs should be applied to the ratings obtained in each society. CFAs of ASR self-ratings by 17,152 18-59-year-olds from 29 diverse societies have supported the eight-syndrome model in each society (Ivanova et al., in press). However, to our knowledge, no published studies report multi-society tests of syndromes of adult psychopathology derived statistically from collateral ratings.
Although focused on personality dimensions rather than psychopathology, EFAs of ratings of the NEO-PI-R (Costa & McCrae, 1992) by collaterals in multiple societies may be instructive. The NEO-PI-R is a 240-item questionnaire for assessing personality dimensions designated as Neuroticism, Extraversion, Openness-to-Experience, Agreeableness, and Conscientiousness. McCrae Terracciano and 78 Members of the Personality Profiles of Cultures Project (2005) performed EFAs on NEO-PI-R collateral ratings for 11,985 18- to 59-year-olds. Data were collected in 50 societies representing a wide range of world regions. Results supported the five NEO-PI-R personality factors in all tested societies, although support was weaker for the five African societies.
Purpose of the present studyVarious studies indicate that reports by collaterals provide important information about adult psychopathology beyond what self-reports provide. The ABCL was developed to obtain informants’ ratings of most of the problems that are self-rated on the ASR. Factor analyses of the ABCL and ASR for U.S. samples have yielded eight similar syndromes that enable researchers and clinicians to rigorously compare collateral versus self-reports. CFAs of ASR ratings from 29 societies have supported the eight-syndrome model in self-ratings but the multi-society generalizability of the syndromes scored from the ABCL needs to be tested. The purpose of this study was to test whether the ABCL eight-syndrome model would be supported in collateral ratings of adults in societies that differed in many ways from the U.S. The multi-society CFA findings for ASR self-ratings suggest that ABCL collateral ratings would also support the eight-syndrome model.
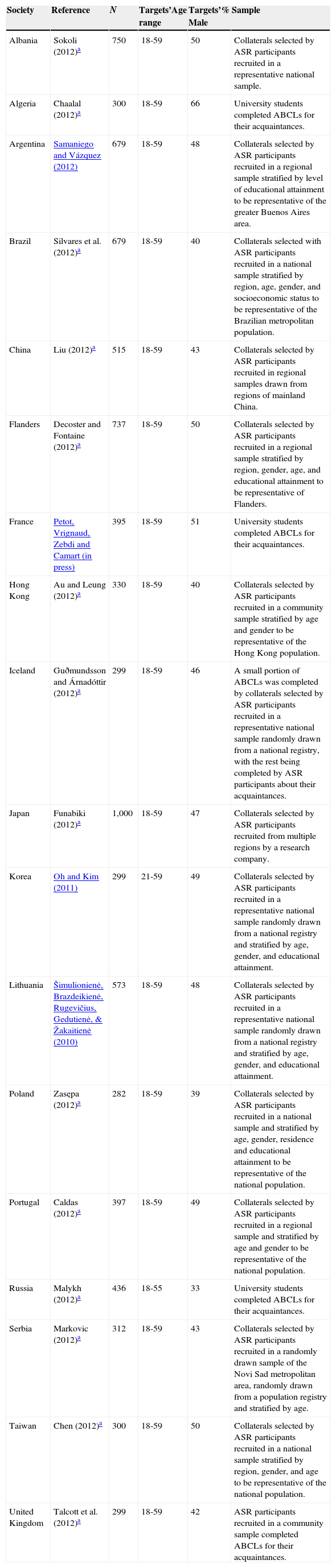
MethodSamplesThe ABCL was completed by 8,582 informants from the 18 samples described in Table 1. Informants were instructed to complete the ABCL about an 18- to 59-year-old they knew well. The ABCLs were completed for 8,582 different adults, i.e., no adult was rated by > 1 informant. Each sample was collected by indigenous researchers, who followed procedures for protection of research participants in their respective institutions. Samples ranged from 282 (Poland) to 1,000 (Japan), with a mean of 477. The gender of assessment targets averaged 46% male. Following scoring conventions for the ABCL (Achenbach & Rescorla, 2003), forms with ≥8 missing items were excluded from analyses. Excluded forms comprised .0081 of the total sample of ABCLs (0% for Albania, Algeria, Argentina, Flanders, France, Japan, Korea, Lithuania, Portugal, Serbia, and Taiwan to 8.8% for Iceland).
Samples used for CFA.
| Society | Reference | N | Targets’Age range | Targets’% Male | Sample |
|---|---|---|---|---|---|
| Albania | Sokoli (2012)a | 750 | 18-59 | 50 | Collaterals selected by ASR participants recruited in a representative national sample. |
| Algeria | Chaalal (2012)a | 300 | 18-59 | 66 | University students completed ABCLs for their acquaintances. |
| Argentina | Samaniego and Vázquez (2012) | 679 | 18-59 | 48 | Collaterals selected by ASR participants recruited in a regional sample stratified by level of educational attainment to be representative of the greater Buenos Aires area. |
| Brazil | Silvares et al. (2012)a | 679 | 18-59 | 40 | Collaterals selected with ASR participants recruited in a national sample stratified by region, age, gender, and socioeconomic status to be representative of the Brazilian metropolitan population. |
| China | Liu (2012)a | 515 | 18-59 | 43 | Collaterals selected by ASR participants recruited in regional samples drawn from regions of mainland China. |
| Flanders | Decoster and Fontaine (2012)a | 737 | 18-59 | 50 | Collaterals selected by ASR participants recruited in a regional sample stratified by region, gender, age, and educational attainment to be representative of Flanders. |
| France | Petot, Vrignaud, Zebdi and Camart (in press) | 395 | 18-59 | 51 | University students completed ABCLs for their acquaintances. |
| Hong Kong | Au and Leung (2012)a | 330 | 18-59 | 40 | Collaterals selected by ASR participants recruited in a community sample stratified by age and gender to be representative of the Hong Kong population. |
| Iceland | Guðmundsson and Árnadóttir (2012)a | 299 | 18-59 | 46 | A small portion of ABCLs was completed by collaterals selected by ASR participants recruited in a representative national sample randomly drawn from a national registry, with the rest being completed by ASR participants about their acquaintances. |
| Japan | Funabiki (2012)a | 1,000 | 18-59 | 47 | Collaterals selected by ASR participants recruited from multiple regions by a research company. |
| Korea | Oh and Kim (2011) | 299 | 21-59 | 49 | Collaterals selected by ASR participants recruited in a representative national sample randomly drawn from a national registry and stratified by age, gender, and educational attainment. |
| Lithuania | Šimulionienė, Brazdeikienė, Rugevičius, Gedutienė, & Žakaitienė (2010) | 573 | 18-59 | 48 | Collaterals selected by ASR participants recruited in a representative national sample randomly drawn from a national registry and stratified by age, gender, and educational attainment. |
| Poland | Zasępa (2012)a | 282 | 18-59 | 39 | Collaterals selected by ASR participants recruited in a national sample and stratified by age, gender, residence and educational attainment to be representative of the national population. |
| Portugal | Caldas (2012)a | 397 | 18-59 | 49 | Collaterals selected by ASR participants recruited in a regional sample and stratified by age and gender to be representative of the national population. |
| Russia | Malykh (2012)a | 436 | 18-55 | 33 | University students completed ABCLs for their acquaintances. |
| Serbia | Markovic (2012)a | 312 | 18-59 | 43 | Collaterals selected by ASR participants recruited in a randomly drawn sample of the Novi Sad metropolitan area, randomly drawn from a population registry and stratified by age. |
| Taiwan | Chen (2012)a | 300 | 18-59 | 50 | Collaterals selected by ASR participants recruited in a national sample stratified by region, gender, and age to be representative of the national population. |
| United Kingdom | Talcott et al. (2012)a | 299 | 18-59 | 42 | ASR participants recruited in a community sample completed ABCLs for their acquaintances. |
Each of the 93 items with significant factor loadings was assigned to only one factor. For each factor, the first item was specified as the metric item (i.e., the scale of the latent factor is set to the scale of that item). All latent factors were modeled as correlated first-order factors, and no hierarchical relations between factors were specified. Item 37. Gets in many fights was omitted for Taiwan, because it was not endorsed by any participant. Because endorsements would have required the investigator to report respondents to the police, four items assessing illegal behavior were not used in Japan (6. Uses drugs (other than alcohol or nicotine) for nonmedical purposes; 57. Physically attacks people; 82. Steals; and 92. Does things that may cause trouble with the law).
Data analysesThe correlated eight-factor model was tested separately in each society, following the factor analytic procedures reported by Achenbach and Rescorla (2003). All 0-1-2 item ratings were transformed to 0 versus 1 or 2, and tetrachoric correlations were computed on these ratings. To account for the nonnormal distribution of the ratings, we used the robust WLSMV estimator (Muthén & Muthén, 1998-2012). It involves computing weighted least square parameter estimates using a diagonal weight matrix with standard errors and mean- and variance-adjusted chi-square test statistic.
We selected the Root Mean Square Error of Approximation (RMSEA) as the primary model fit index because it was identified as the best performing index for the WLSMV (Yu & Muthén, 2002). Yu and Muthén (2002) found that RMSEA values of<.05-.06 indicated good model fit for ordered categorical variables in a simulation study. We also computed the Comparative Fit Index (CFI; Bentler, 1990) and Tucker Lewis Index (TLI; Tucker & Lewis, 1973), but considered their results to be secondary to the RMSEA. We did not use other model fit indices generated by Mplus for CFAs with the WLSMV (e.g., SRMR, WRMR), because Yu and Muthén (2002) found that they did not perform as reliably as the RMSEA, CFI, and TLI with binary or ordered categorical variables. Based on the results of their simulation study with three five-item factors, Hu and Bentler (1999) proposed that CFI and TLI values greater than .95 should be interpreted to indicate good model fit. However, Marsh, Hau, and Wen (2004) argued that Hu and Bentler's threshold was too stringent for complex models. Because our model was much more complex than Hu and Bentler's, we adopted the less stringent criteria of .80 to .90 to indicate acceptable model fit, and ≥.90 to indicate good model fit.
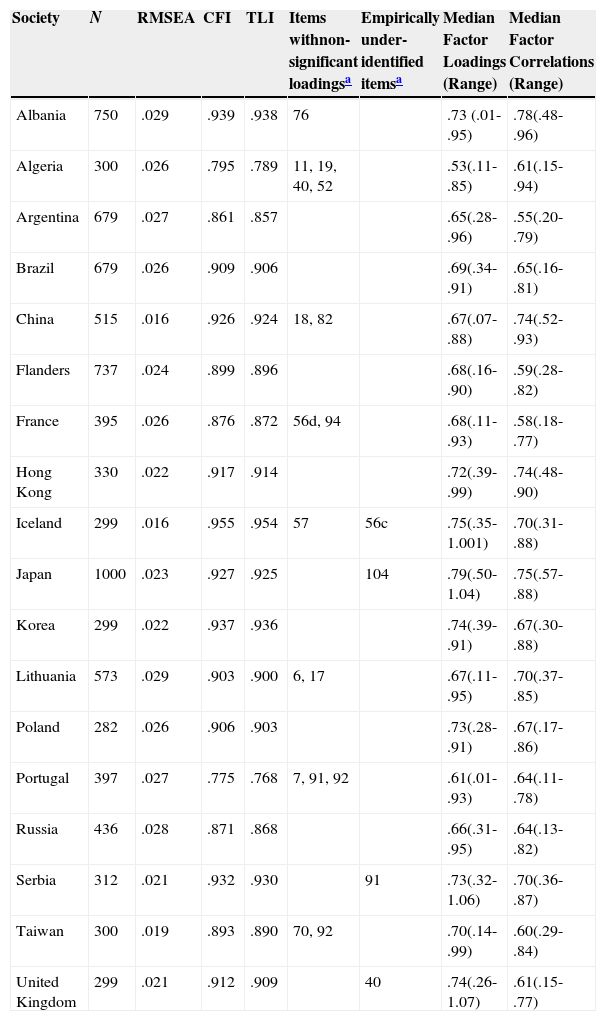
ResultsThe correlated eight-factor model converged for all samples. RMSEAs ranged from .016 (China and Iceland) to .029 (Albania and Lithuania), indicating good fit for all societies (Table 2). The RMSEAs equaled .021, .025, and .027 at the 25th, 50th, and 75th percentiles, respectively. CFIs ranged from .775 for Portugal to .955 for Iceland. TLI values were similar to CFI values within societies, ranging from .768 for Portugal to .954 for Iceland. CFIs and TLIs indicated acceptable to good model fit for all societies, except Portugal and Algeria.
CFA results.
| Society | N | RMSEA | CFI | TLI | Items withnon-significant loadingsa | Empirically under-identified itemsa | Median Factor Loadings (Range) | Median Factor Correlations (Range) |
|---|---|---|---|---|---|---|---|---|
| Albania | 750 | .029 | .939 | .938 | 76 | .73 (.01-.95) | .78(.48-.96) | |
| Algeria | 300 | .026 | .795 | .789 | 11, 19, 40, 52 | .53(.11-.85) | .61(.15-.94) | |
| Argentina | 679 | .027 | .861 | .857 | .65(.28-.96) | .55(.20-.79) | ||
| Brazil | 679 | .026 | .909 | .906 | .69(.34-.91) | .65(.16-.81) | ||
| China | 515 | .016 | .926 | .924 | 18, 82 | .67(.07-.88) | .74(.52-.93) | |
| Flanders | 737 | .024 | .899 | .896 | .68(.16-.90) | .59(.28-.82) | ||
| France | 395 | .026 | .876 | .872 | 56d, 94 | .68(.11-.93) | .58(.18-.77) | |
| Hong Kong | 330 | .022 | .917 | .914 | .72(.39-.99) | .74(.48-.90) | ||
| Iceland | 299 | .016 | .955 | .954 | 57 | 56c | .75(.35-1.001) | .70(.31-.88) |
| Japan | 1000 | .023 | .927 | .925 | 104 | .79(.50-1.04) | .75(.57-.88) | |
| Korea | 299 | .022 | .937 | .936 | .74(.39-.91) | .67(.30-.88) | ||
| Lithuania | 573 | .029 | .903 | .900 | 6, 17 | .67(.11-.95) | .70(.37-.85) | |
| Poland | 282 | .026 | .906 | .903 | .73(.28-.91) | .67(.17-.86) | ||
| Portugal | 397 | .027 | .775 | .768 | 7, 91, 92 | .61(.01-.93) | .64(.11-.78) | |
| Russia | 436 | .028 | .871 | .868 | .66(.31-.95) | .64(.13-.82) | ||
| Serbia | 312 | .021 | .932 | .930 | 91 | .73(.32-1.06) | .70(.36-.87) | |
| Taiwan | 300 | .019 | .893 | .890 | 70, 92 | .70(.14-.99) | .60(.29-.84) | |
| United Kingdom | 299 | .021 | .912 | .909 | 40 | .74(.26-1.07) | .61(.15-.77) |
Note. RMSEA=Root Mean Square Error of Approximation, CFI=Comparative Fit Index, TLI=Tucker-Lewis Index.
For 10 societies, all 93 tested items had statistically significant loadings on their respective factors. As shown in Table 2, 17 item loadings were not statistically significant (one for Albania and Iceland, two for China, France, Lithuania, and Taiwan, three for Portugal, and four for Algeria). The 17 nonsignificant loadings comprised 1.01% of the 1,669 loadings we tested (92 for Taiwan and 89 for Japan, plus 93 for the remaining 16 societies).
Table 2 presents medians and ranges of factor loadings for each society. The median factor loading ranged from .53 (Algeria) to .79 (Japan), with an overall median of .70. Table 2 also presents medians and ranges for correlations between latent factors across the 18 societies. Median latent factor correlations ranged from .55 in the Argentine sample to .78 in the Albanian sample, with an overall median of .66.
Table 3 presents the means, medians, standard deviations, and ranges of the loadings for each item and for the items comprising each syndrome across the 18 societies. For each item, the median factor loading across societies ranged from .49 (121. Late for appointments) to .87 (54. Feels tired without good reason), with an overall median of .71. For the items comprising each syndrome, median loadings ranged from .65 (Attention Problems) to .74 (Thought Problems).
Descriptive statistics for factor loadings across 18 societies by syndrome.
| Syndromes and items | Mean | Median | ||
|---|---|---|---|---|
| loading | loading | SD | Range | |
| Anxious/Depressed | .69 | .72 | .09 | .57-.85 |
| 12. Lonely | .64 | .66 | .10 | .39-.77 |
| 14. Cries a lot | .56 | .59 | .11 | .29-.73 |
| 31. Fears doing bad | .57 | .58 | .16 | .25-.86 |
| 33. Feels unloved | .77 | .79 | .08 | .60-.88 |
| 34. Others out to get her | .77 | .77 | .08 | .60-.95 |
| 35. Feels worthless | .77 | .77 | .08 | .50-.87 |
| 45. Nervous, tense | .73 | .76 | .07 | .61-.80 |
| 47. Lacks self-confidence | .70 | .71 | .07 | .54-.80 |
| 50. Fearful, anxious | .69 | .72 | .12 | .32-.87 |
| 52. Feels too guilty | .61 | .65 | .17 | .11-.81 |
| 71. Self-conscious | .56 | .57 | .14 | .31-.85 |
| 103. Unhappy, sad | .84 | .85 | .05 | .73-.92 |
| 107. Can’t succeed | .71 | .72 | .10 | .52-.82 |
| 112. Worries | .57 | .57 | .14 | .29-.76 |
| Withdrawn | .69 | .73 | .10 | .52-.77 |
| 25. Doesn’t get along | .78 | .77 | .07 | .66-.89 |
| 30. Poor relations with | ||||
| opposite sex | .66 | .68 | .10 | .40-.81 |
| 42. Rather be alone | .52 | .52 | .07 | .39-.61 |
| 48. Not liked | .74 | .76 | .14 | .36-.95 |
| 60. Enjoys little | .74 | .75 | .12 | .44-.91 |
| 65. Refuses to talk | .72 | .73 | .10 | .52-.91 |
| 67. Trouble making friends | .76 | .76 | .06 | .64-.89 |
| 69. Secretive | .50 | .53 | .17 | .25-.74 |
| 111. Withdrawn | .68 | .73 | .15 | .28-.85 |
| Somatic Complaints | .68 | .70 | .13 | .50-.87 |
| 51. Feels dizzy | .77 | .76 | .10 | .56-.92 |
| 54. Tired without reason | .84 | .87 | .08 | .66-.97 |
| 56a. Aches, pains | .67 | .70 | .13 | .32-.80 |
| 56b. Headaches | .59 | .57 | .09 | .39-.77 |
| 56c. Nausea, feels sick | .74 | .76 | .13 | .41-1.001a |
| 56d. Eye problems | .49 | .50 | .17 | .11-.79 |
| 56e. Skin problems | .50 | .53 | .13 | .16-.69 |
| 56f. Stomachaches | .62 | .64 | .12 | .30-.86 |
| 56g. Vomiting | .76 | .77 | .19 | .26-1.00 |
| Thought Problems | .73 | .74 | .07 | .60-.84 |
| 9. Can’t get mind off thoughts | .58 | .60 | .14 | .32-.81 |
| 18. Harms self | .72 | .78 | .23 | .10-.95 |
| 40. Hears sounds, voices | .69 | .74 | .24 | .21-1.07a |
| 66. Repeats acts | .64 | .67 | .15 | .34-.96 |
| 70. Sees things | .66 | .75 | .21 | .23-.94 |
| 80. Stares blankly | .69 | .70 | .12 | .38-.99 |
| 84. Strange behavior | .78 | .76 | .12 | .50-.96 |
| 85. Strange ideas | .68 | .71 | .13 | .43-.88 |
| 91. Suicidal thoughts | .79 | .84 | .19 | .32-1.06a |
| Attention Problems | .65 | .65 | .09 | .49-.76 |
| 1. Forgetful | .50 | .51 | .05 | .39-.57 |
| 8. Can’t concentrate | .64 | .64 | .09 | .40-.80 |
| 11. Too dependent | .63 | .65 | .13 | .15-.73 |
| 13. Confused | .75 | .76 | .07 | .56-.87 |
| 17. Daydreams | .52 | .56 | .16 | .11-.77 |
| 53. Trouble planning | .69 | .71 | .07 | .59-.83 |
| 59. Fails to finish | .73 | .74 | .08 | .56-.87 |
| 61. Poor work performance | .75 | .75 | .09 | .53-.92 |
| 64. Trouble setting priorities | .73 | .75 | .07 | .58-.83 |
| 78. Trouble making | ||||
| decisions | .71 | .72 | .06 | .62-.79 |
| 96. Lacks initiative | .65 | .64 | .07 | .51-.79 |
| 101. Skips job | .63 | .61 | .15 | .42-.94 |
| 102. Lacks energy | .68 | .67 | .10 | .53-.87 |
| 105. Disorganized | .70 | .71 | .09 | .57-.84 |
| 108. Loses things | .57 | .57 | .08 | .41-.71 |
| 119. Not good at details | .58 | .57 | .11 | .38-.79 |
| 121. Late for appointments | .48 | .49 | .09 | .28-.62 |
| Aggressive Behavior | .70 | .70 | .06 | .61-.80 |
| 3. Argues | .61 | .61 | .09 | .40-.78 |
| 5. Blames others | .68 | .66 | .09 | .47-.82 |
| 16. Mean to others | .67 | .69 | .15 | .48-.90 |
| 28. Gets along badly with family | .65 | .66 | .09 | .44-.80 |
| 37. Gets in fights | .65 | .61 | .18 | .22-1.00 |
| 55. Mood swings between | ||||
| elation and depression | .77 | .75 | .09 | .64-.93 |
| 57. Attacks people | .67 | .67 | .12 | .42-.88 |
| 68. Screams a lot | .66 | .66 | .09 | .44-.80 |
| 81. Changeable behavior | .79 | .80 | .06 | .62-.90 |
| 86. Stubborn, sullen, irritable | .72 | .72 | .09 | .51-.82 |
| 87. Mood changes | .80 | .79 | .05 | .69-.90 |
| 95. Hot temper | .71 | .72 | .08 | .60-.88 |
| 97. Threatens people | .69 | .71 | .15 | .46-.95 |
| 113. Sulks | .74 | .75 | .08 | .49-.84 |
| 116. Easily upset | .76 | .77 | .11 | .42-.91 |
| 118. Impatient | .68 | .68 | .11 | .53-.91 |
| Rule-Breaking Behavior | .68 | .71 | .09 | .51-.86 |
| 6. Uses drugs | .48 | .51 | .13 | .23-.65 |
| 23. Breaks rules | .66 | .65 | .10 | .48-.84 |
| 26. Lacks guilt | .60 | .63 | .13 | .35-.83 |
| 39. Bad friends | .66 | .71 | .16 | .31-.93 |
| 41. Impulsive | .72 | .72 | .10 | .47-.85 |
| 43. Lying, cheating | .71 | .72 | .09 | .58-.83 |
| 76. Irresponsible | .79 | .86 | .21 | .01-.93 |
| 82. Steals | .68 | .72 | .20 | .07-.93 |
| 90. Gets drunk | .49 | .52 | .11 | .26-.63 |
| 92. Trouble with the law | .64 | .72 | .24 | .01-.85 |
| 114. Fails to pay debts | .69 | .73 | .17 | .25-.93 |
| 117. Trouble managing money | .67 | .68 | .09 | .47-.81 |
| 122. Trouble keeping jobs | .72 | .71 | .12 | .54-.96 |
| Intrusive | .68 | .69 | .06 | .59-.76 |
| 7. Brags | .63 | .67 | .21 | .06-.93 |
| 19. Demands attention | .69 | .70 | .18 | .11-.89 |
| 74. Showing off, clowning | .65 | .70 | .17 | .30-.89 |
| 93. Talks too much | .59 | .59 | .10 | .41-.75 |
| 94. Teases a lot | .67 | .68 | .19 | .12-.93 |
| 104. Loud | .75 | .76 | .12 | .53-1.04a |
Note. Values in italics are descriptive statistics for median item loadings comprising the syndromes.
For four societies, one item had a negative residual, indicating that it was misspecified (item 56c. Nausea, feels sick for Iceland; item 104. Is unusually loud for Japan; item 91. Talks about killing self for Serbia; and item 40. Hears sounds or voices that aren’t there (describe) for the UK). Because the 95% confidence intervals for all four parameters included the admissible parameter space, sampling fluctuations may explain their misspecification (Chen, Bollen, Paxton, Curran, & Kirby, 2001). These four out-of-range parameters comprised only 0.08% of the 5,007 parameters that we estimated (93 thresholds, item loadings, and residuals for 16 societies, 92 thresholds, item loadings, and residuals for Taiwan, and 89 thresholds, item loadings, and residuals for Japan).
Discussion/conclusionsThe ABCL was developed to meet needs for multi-informant assessment of adult psychopathology by obtaining informant ratings of the same clinical constructs as rated by the people being assessed. Because findings in the society where an instrument originated cannot be assumed to generalize to other societies without empirical evidence, instruments and constructs should be empirically tested in multiple societies. The more diverse the societies in which an instrument's constructs are supported, the more confidence their generalizability warrants. We used CFAs to test the ABCL's eight-syndrome model in 18 societies from such very different regions as Africa, Asia, South America, and Eastern, Northern, and Western Europe.
We found that the eight-syndrome model scored from ABCL ratings by collaterals was supported by RMSEAs ranging from .016 for China and Iceland to .029 for Albania and Lithuania. The small size of the RMSEAs indicated very good fit for the eight-syndrome model in all 18 societies in which collaterals completed ABCLs. The secondary fit indices indicated acceptable to good fit in all societies except Algeria and Portugal. Of the 1,669 loadings that were tested, the median loading was .71, and only 17 (1.01%) were not significant. Of the 5,007 parameters that were estimated, 4 (0.08%) were out of range, but 95% confidence intervals included the admissible range for all 4. Our findings thus supported the same eight-syndrome model for collateral ratings as was previously supported for self-report ratings (Ivanova et al., in press).
Our findings indicate that the eight-syndrome model was supported for operationalizing phenotypes of mutually associated problems rated by collaterals in 18 societies that differed in ethnicity, language, religion, geographical region, and economic, mental health, and political systems. Combined with similar findings for the eight-syndrome model in ASR self-ratings from 17 of these societies (Ivanova et al., in press), our findings support the applicability of the syndromes scored from the parallel collateral- and self-rating instruments for 18-59-year-olds in many parts of the world. Additional items, instruments, and models are likely to be useful. However, the ASR and ABCL items and the eight syndromes scored from them provide a core data language for describing and quantifying psychopathology that can be widely used for research and clinical purposes in conjunction with whatever additional items, instruments, and/or models may be warranted in particular contexts and societies.
ImplicationsThe findings support use of the ABCL to assess 18-59-year-olds in terms of the eight-syndrome model scored from collateral ratings in many societies. When the people being assessed rate themselves on the ASR, the parallel items and scales of the two instruments enable clinicians and researchers to identify specific similarities and differences between collateral- and self-reports. To evaluate the degree of deviance indicated by particular scores on each syndrome, research is needed to test differences between scores for different societies, males versus females in different age groups, and collateral- versus self-ratings, as is now being done (Rescorla, 2014;Rescorla et al., 2014). The findings provide a basis for constructing norms that take account of differences in distributions of scores for different societies, each gender/age group, and collateral- versus self-ratings. Computer software will then enable users to display syndrome scale scores in relation to norms appropriate for each society and gender/age group for collateral- and self-ratings.
LimitationsThe present study tested the configural invariance of the ABCL syndrome structure in data from 18 societies. Configural invariance, which is the most fundamental component of measurement invariance, means that an assessment instrument measures the same construct(s) across different populations (e.g., Vandenberg & Lance, 2000). Because our tested model was complex and the WLSMV estimator (which we used to account for the ordered categorical nature of our data) is very computationally intensive, we were unable to successfully execute tests of other components of measurement invariance (i.e., metric, scalar, item residual, and factor), which all require multi-sample modelling.
Although the study reported here extends evidence-based collateral assessment of psychopathology across diverse societies, it is limited to what Pike (1967) called etic research, which applies the same standardized assessments to people in different societies. We did not hypothesize that the ABCL syndrome structure is universal nor that every ABCL item is equally applicable in all societies. Instead, the study's purpose was to test the degree to which the ABCL syndrome structure fit ratings of the ABCL items in 18 specific societies.
Detailed comparisons of scores in different societies (Rescorla, 2014; Rescorla et al., 2014) may reveal societal differences that warrant what Pike (1967) called emic research, which is customized for particular societies to explore society-specific phenomena. Emic research may also be used to test the validity of the ABCL items and syndromes according to society-specific criteria. The findings may argue for use of other items and syndrome models in particular societies.
Available online 29 August 2014
