





COVID-19 can converge with the pro-inflammatory immunoregulatory mechanisms of chronic lung diseases. Given the disorders inherent to lung transplantation and the inexistence of other definitive therapeutic alternatives, Adipose tissue-derived Stem Cells (ASCs) presented themselves as a therapeutic hope. The purpose of this review is to assess the basis for the potential use of ASCs in lung diseases unresponsive to conventional therapy, relating to their possible use in COVID-19 ARDS. 35 studies comprised this review, 14 being narrative reviews, 19 preclinical trials and two proofs of concept. COVID-19 can converge with the pro-inflammatory immunoregulatory mechanisms of chronic lung diseases. In view of the disorders inherent to lung transplantation and the inexistence of definitive therapeutic alternatives, Adipose tissue-derived Stem Cells (ASCs) presented themselves as a therapeutic hope. Its detailed reading indicated the absence of serious adverse effects and toxicity to the administration of ASCs and suggested possible effectiveness in reducing lung damage, in addition to promoting the recovery of leukocytes and lymphocytes with its immunomodulatory and anti-apoptotic effects. The revised clinical data suggests optimism in the applicability of ASCs in other immunoinflammatory diseases and in severe COVID-19 ARDS. However, further studies are needed to develop a consensus on the methods of collection of ASCs, the ideal dosage schedule, the most effective time and route of administration, as well as on the definition of indications for the administration of ASCs in cases of COVID-19 for conducting clinical trials in near future.
The end of 2019 was marked by the growing number of cases of severe respiratory illnesses of unknown origin in Wuhan, China; in January 2020, its etiologic agent, the contagious Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) was identified [1]. Two months later, in March 2020, the World Health Organization (WHO) elevated a category of the 2019 Coronavirus Disease (COVID-19) from epidemic to the first pandemic caused by coronavirus, which on March 2, 2021 already illustrated a scenario with 2.6 million new confirmed and an increase of 63,000 deaths in the last week [2].
SARS-CoV-2 is one of three coronaviruses that evolve with Acute Respiratory Distress Syndrome (ARDS) [3]. Despite the genomic similarity of 79% to the Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) and 50% to the Middle East Respiratory Syndrome coronavirus (MERS-CoV), SARS-CoV-2 does not stand out for its relatively low 6.76% mortality, compared to 9.6% for SARS-CoV and 35.5% for MERS-CoV, but rather due to its high infectivity, which underscores the superiority of absolute numbers over percentage data [4].
Despite different etiologies, the pathophysiology of COVID-19 may converge to the same pro-inflammatory immunoregulators of chronic lung diseases:[3] abnormal repair processes with concomitant destruction of airway epithelium[5] and vascular endothelium [6]. However, regardless of the steady growth in the prevalence of asthma and Chronic Obstructive Pulmonary Disease (COPD) in recent years as well as COPD ranking third among the causes of chronic disease mortality worldwide, lung transplantation is still the only curative therapy for chronic lung disorders [1].
Due to the lack of other definitive therapeutic alternatives for chronic lung diseases and the disorders inherent to lung transplantation ‒ high donor incompatibility, lifelong need for immunosuppressive therapy, and high mortality rate after the procedure (50% in 5 years)[1] ‒ Preclinical and clinical studies of Mesenchymal Stem Cells (MSCs), with their paracrine immunomodulatory mechanisms that reduce pulmonary inflammation and promote tissue repair, have raised expectations about this possibility of treatment for chronic lung disease [1,7].
Even though, since their first description in 1968 [8], the number of clinical trials using MSCs in the management of lung diseases was somewhat unimpressive until this year, when the SARS-CoV-2 pandemic led to the pursuit of possible effective treatments, as of March 9, 2021, of the 110 studies registered in the National Institutes of Health (NIH) Clinical Trial Database on the use of cell therapy in lung diseases, 72 are specifically for COVID-19, with new studies being registered daily [9,10].
Adipose Tissue (TA) MSCs have received increasing attention over the years, both for their practical collection using local anesthesia [11], and for the greater quantity and easy isolation of target stem cells compared to those originating from Bone Marrow (BM) [11]. As one of the cellular components of the stromal Vascular Fraction (FVE), the portion of subcutaneous fat, it can be easily isolated by enzymatic degradation of adipocytes and cell expansion [11].
Although the analysis of experimental studies by Wecht and Rojas 12] has suggested both efficacy – reducing inflammation, preventing the progression of fibrosis, and accelerating tissue repair – and safety in the use of MSCs in chronic lung diseases, the effects of ASCs are underreported. Therefore, the objective of this study is to evaluate, through a systematic review of the literature, the therapeutic rationale of ASCs in chronic or acute pulmonary diseases that are unresponsive to conventional therapy, relating to their possible use in ARDS by COVID-19.
MethodGeneral informationThe present study is a systematized review of the literature. Systematized review is a classification described in the literature that attempts to include elements from the systematic review process to the narrative review while maintaining greater freedom in the quality assessment and comprehensive searching, all of which are shown in their limitations of methodology. To this end, the present article used an adaptation of the PRISMA guidelines suitable for systematized reviews.
The following databases were searched:
- •
CENTRAL (Cochrane Library) - https://www.cochranelibrary.com/
- •
CLINICAL TRIALS - https://clinicaltrials.gov
- •
LILACS (BIREME) - http://brasil.bvs.br/
- •
MEDLINE (PubMed) - https://www.ncbi.nlm.nih.gov/pubmed/
- •
SCOPUS - https://www.scopus.com
- •
WEB OF SCIENCE - https://www.webofscience.com
The descriptors (DeCS/MeSH) selected, in Portuguese and English, were: mesenchymal stem cells (células tronco mesenquimais), pneumonia (broncopneumonia) and pulmonary fibrosis (fibrose pulmonar).
Search strategies1 - ((pulmonary fibrosis[MeSH Terms]) OR (fibrose pulmonar [DeCS Terms]) OR (pneumonia[MeSH Terms]) OR (broncopneumonia[DeCS Terms])) AND ((mesenchymal stem cells[MeSH Terms]) OR (células tronco mesenquimais [DeCS Terms))
2 - Articles referenced by the works filtered from the search strategy that covered the eligibility criteria were also added.
Selection process according to the inclusion and exclusion criteriaPublications were selected using the search strategy previously described, without date or language limitation. Duplicates and titles not related to the topic were excluded before the screening.
The inclusion criteria choice was based on the PICO strategy. The study population included lung diseases, the intervention analyzed was the infusion of mesenchymal stem cells derived from adipose tissue, which was compared to conventional treatment or placebo saline infusion and analyzed for efficacy and safety.
In the first selection process abstracts were reviewed for the following inclusion criteria: (a) Administration of Intravenous (IV) ASCs, which (b) Were not used as a concurrent vehicle for other therapeutic agents, as (c) Treatment for acute or chronic lung diseases.
The second selection process excluded: a) Editorials, comments, and letters to the editor, in addition to articles that b) Discussed exclusively non-adipose stem cells and derivatives, or that c) Did not involve the intravenous administration of ASCs in d) Pulmonary immunoinflammatory diseases.
EndpointsThe evaluated outcomes can be divided according to two main approaches: efficacy and safety. The primary endpoint of the efficacy assessment was clinical parameters, while the primary endpoints of the safety assessment were descriptions of serious adverse events and death correlated to the intravenous administration of ASCs. Secondary outcomes included: a) For efficacy ‒ analysis of the homing capacity of ASCs, serial imaging tests, histopathology, cytology, biochemistry, TUNEL method, PCRs, and immunohistochemistry, in addition to taking into account the study design, its participants, the origin of ASCs and dosage administered for comparative purposes; as well as b) Safety ‒ mild adverse effects (transient fever, diarrhea, bronchitis and common colds) secondary to the IV infusion of ASCs.
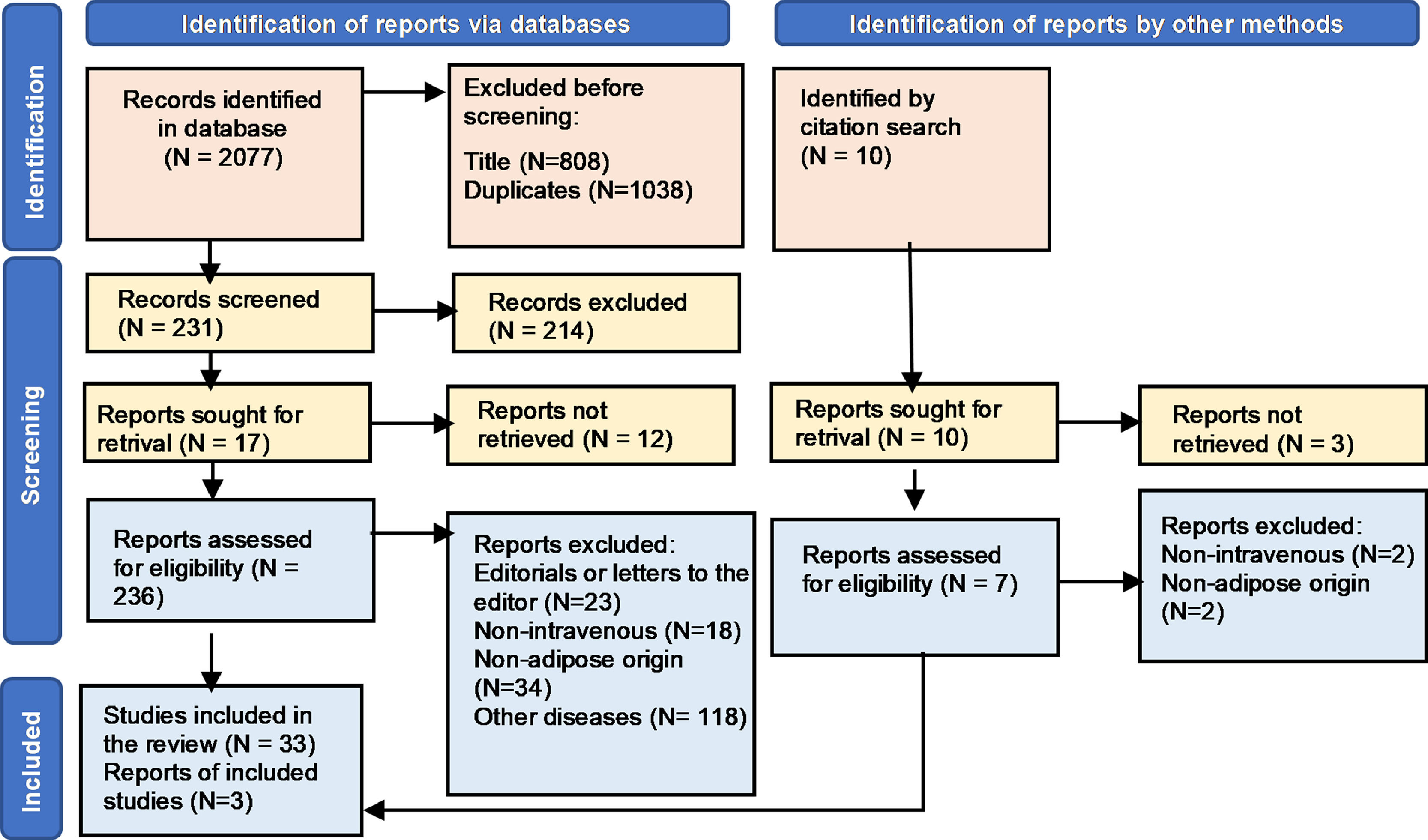
ResultsAfter inserting the search strategy in databases, 2077 results were obtained, among which 1046 studies were initially excluded, then, based on the reading of titles and abstracts before the screening, only 231 articles were pre-selected (Fig. 1). After evaluating the full text according to the eligibility criteria already described, 36 studies composed this review, being: 14 narrative reviews, 19 preclinical trials and three clinical trials. The clinical characteristics of these studies are summarized in Tables 1, 2 and 3.
.")
Flowchart of the selection process for researched articles. Legend: After inserting the search strategy in the databases, 2077 results were obtained, among which 1846 studies were initially excluded and only 231 articles were pre-selected, based on the reading of titles and abstracts. After evaluating the full text according to the eligibility criteria already described, 36 studies composed this review, being: 14 narrative reviews, 19 preclinical trials and three proofs of concept (N, Number).
Narrative reviews on the administration of ASCs in chronic or acute lung diseases.
COVID-19, 2019 Coronavirus Disease; ARDS, Acute Respiratory Distress Syndrome; COPD, Chronic Obstructive Pulmonary Disease; IPF, Idiopathic Pulmonary Fibrosis; PAH, Pulmonary Arterial Hypertension; PF, Pulmonary Fibrosis; BLM, Bleomycin; LP, Lung Lesion; NR, Does Not Refer; ASCs, Adipose tissue-derived Stem Cells; TGF-b, Transforming Growth Factor beta; TNF-α, Tumor Necrosis Factors Alpha; IFN-γ, Interferon-gamma; IL, Interleukin; MMP, Metalloproteinases; IV, Intravenous; IT, Intratracheal; EB, Endobronchial; DU, Single Dose; kg, Kilogram; MSC, Mesenchymal Stem Cells; CD, Differentiation Cluster; cell., Cells.
Preclinical trials on the administration of ASCs in chronic or acute lung diseases.
PF, Pulmonary Fibrosis; BLM, Bleomycin; MTX, Methotrexate; ALI, Acute Lung Injury; LP, Lung Injury; COPD, Chronic Obstructive Pulmonary Disease; RCT, Randomized Trial with a Control group; αSMA, α Smooth Muscle Actin; IL, Interleukin; TGF-β, Transforming Growth Factor Beta; TNF-α, Tumor Necrosis Factors Alpha; bFGF, Basic Fibroblast Growth Factor; CTGF, Connective Tissue Growth Factor; Col., Collagen; MMP, Metalloproteinases; VEGF, Endothelial Growth Factor; Nrf2, Factor 2 Related to Nuclear erythroid Factor 2; ROS, Reactive Oxygen Species; IGF, Insulin-Like Growth Factor; MDA, Malondialdehyde, GSH, Reduced Glutathione; SOD, Superoxide Dismutase; HGF, Hepatocyte Growth Factor; PG, Prostaglandin; MIP, Macrophage Inflammatory Protein, MPO, Myeloperoxidase; VCAM, Vascular Cell Adhesion Molecule; MCP, Monocyte Chemotactic Protein; PDGF, Platelet-Derived Growth Factor; NOS, Nitric Oxide Synthase; NO, Nitric Oxide; KGF, Keratinocyte Growth Factor; Ang-1, Angiotensin 1; PGDH, Hydroxyprostaglandin Dehydrogenase; IFN-γ, Interferon-Gamma; Ig, Immunoglobulin; IDO, Indoleamine 2,3 Dioxygenase; BALF, Bronchoalveolar Lavage; IV, Intravenous; IT, Intratracheal; GAPDH, Glyceraldehyde-3-Phosphate Dehydrogenase; MSC, Mesenchymal Stem Cells; ASC-MC, Conditioned Medium from in vitro Adipose Cell Culture; DU, Single Dose; cell., Cells; mL, Milliliter; µL, Microliter; CD, Differentiation Cluster; ASCs, Adipose issue-derived Stem Cells; kg, Kilogram; PE, Phycoerythrin; FITC, Fluorescein Isothiocyanate; APC, Antigen Presenting Cell; HLA, Human Leukocyte Antigen System; mAb, Monoclonal Antibodies; NR, Does Not Refer; yASCs, ASCs taken from young animals; oASCs, ASCs taken from elderly animals; BM-MSCs, Bone Marrow-derived Stem Cells; LPS, Lipopolysaccharide; NETs, Extracellular Neutrophil Traps; NR, Does Not Refer.
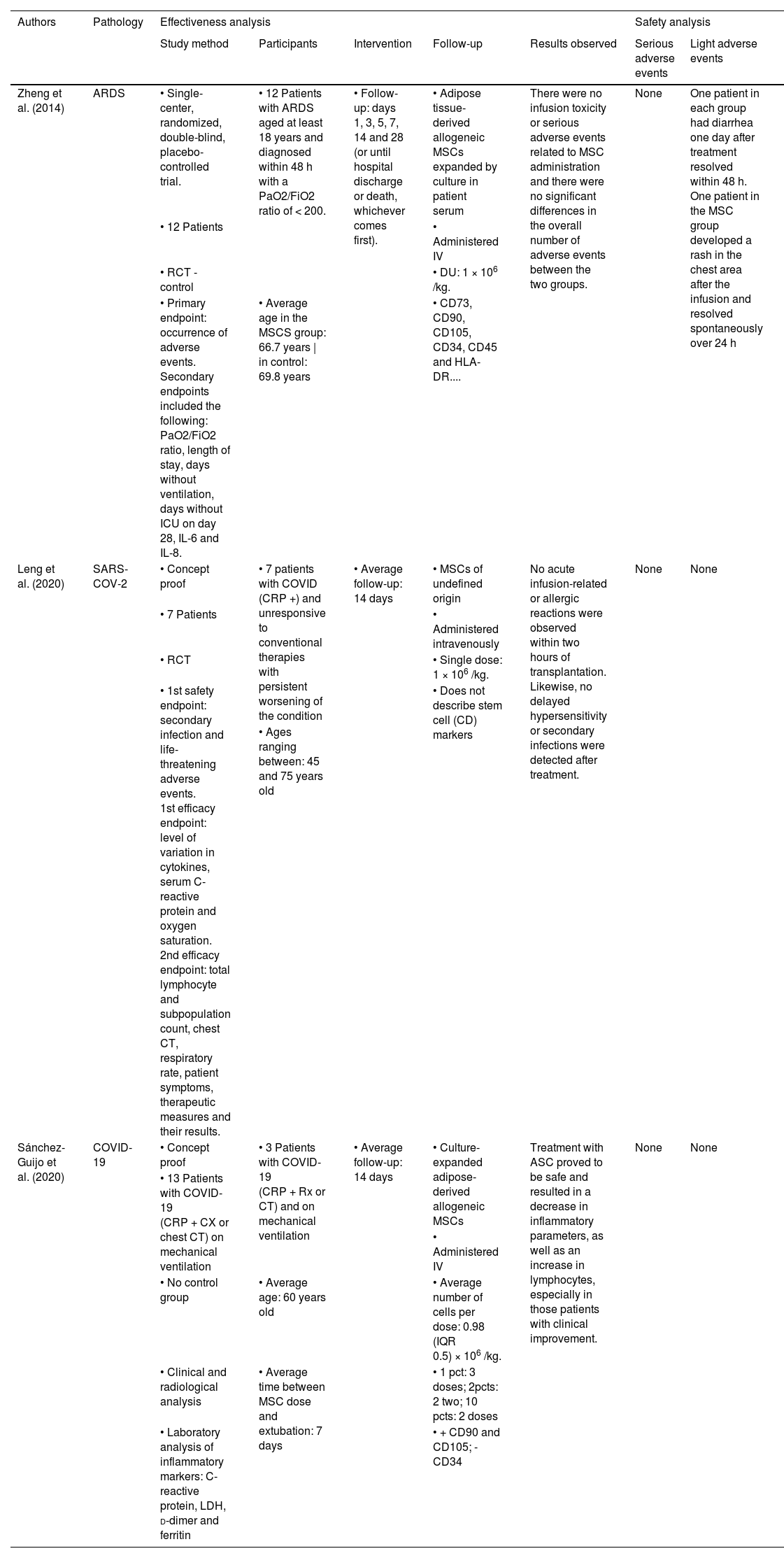
Published clinical trials on the administration of ASCs in chronic or acute lung diseases.
COVID-19, 2019 Coronavirus Disease; ARDS, Acute Respiratory Distress Syndrome; PCR, Reverse Transcription followed by Polymerase Chain Reaction; X-Ray, Radiography; CT, Computed Tomography; RCT, Randomized Trial; LDH, Lactate Dehydrogenase; FiO2, Inspired Oxygen Fraction; PaO2, Arterial Oxygen Pressure; ICU, Intensive Care Units; IL, Interleukin; MSC, Mesenchymal Stem Cells; IV, Intravenously; kg., Kilogram; pct(s), Patient(s); CD, Differentiation Cluster; HLA, Human Leukocyte Antigen system; DU, Single Dose; IQR, Interquartile Range; ASCs, Adipose tissue-derived Stem Cell; sCABP, Severe Community-Acquired Bacterial Pneumonia; IMV, Invasive Mechanical Ventilation.
The search in the clinical trials database resulted in 29 studies of adipose-derived stem cells in lung diseases, their official status being: one no longer available, five unknown, five withdrawn, one enrolling by invitation, four recruiting, four not yet recruiting, one suspended, two terminated, six completed. No study has published its results in academic journals in the literature to date. The population, intervention, comparator and outcome of these studies are summarized in Table 4.
Unpublished clinical trials on the administration of ASCs in chronic or acute lung diseases.
SVF, Stromal Vascular Fraction; PRP, Platelet Rich Plasma; BMMC, Bone Marrow Mononuclear Cells; ASCs, Adipose-derived Stem Cell; COPD, Chronic Obstructive Pulmonary Disease; CRP, C-Reactive Protein; Pro-BNP, Pro-type B Natriuretic peptide; BI, Bilirubin; Cr, Creatinine; AEs, Adverse Effects; SAEs, Severe Adverse Effects; SOFA, Sequential Organ Failure Assessment; IV, Intravenously; CCO, Corticosteroids; ARDS, Acute Espiratory Distress Syndrome; 6MWD, 6-Minute Walk Distance; AP, Alkaline Phosphatase; ALT,. Alanine Aminotransferase; AST, Aspartate Aminotransferase; K, Potassium; Hb, Hemoglobin; Ht, Hematocrit; MCV, Mean Corpuscular Volume; MCHb, Mean Corpuscular Hemoglobin; Eos, Eosinophils; Neutro, Neutrophils; Lymphs, Lymphocytes; Mono, Monocytes; Baso, Basophils; Ca, Calcium; Na, Sodium; Cl, Chloride; PTT, Prothrombin Time; SF-36, Short-Form 36 Health Survey.
Searching the gray literature did not present results contemplated by the subject of the study.
DiscussionAlthough the mechanisms by which ASCs reduce lung inflammation and promote tissue repair are not fully elucidated [3], the use of mesenchymal stem cells in acute lung diseases had previously been reviewed by current literature showing promising results [13]. Since the initial analysis of the new disease caused by SARS-CoV-2 demonstrated main pathologic features similar to ALI/ARDS [14], the hypothesis of transposing these benefits in the context of a new pandemic without known therapeutic options were naturally investigated [1,3,14]. However, upon closer analysis, peculiarities were found in the pathophysiology of COVID-19 that benefited from autologous or allogeneic IV ASCs in a different way than those initially imagined [3].
In this context the present study proposed to analyze the benefits of cell therapy in COVID-19, exposing the possible common path among chronic and acute lung diseases that allow COVID-19 to manifest itself like chronic lung diseases [1,6], with fibrosis and pulmonary consolidation, but with an acute and fulminant evolution [6], owing to inflammatory exudation, pulmonary edema, and inflammatory cytokine storm.
Thus, the effectiveness evidenced by Liu et al. [3], Siu et al. [15]. and other studies is here revised as being due to immune dysregulation and fibrosis being common components of the pathophysiology of chronic and acute lung diseases, being closely related to their morbidity and mortality despite the different etiologies [7,13]. This convergence differs from a physiological immune response by inflammation resulting from both the activation of native pulmonary macrophages, molecular patterns associated with pathogens or associated damage, and the overproduction of alarmins that attract circulating immune cells to the lungs, initiating inflammation secondary to trauma and hypersensitivity [16,17].
Regarding clinical parameters, the present review is in line with similar studies by showing that IV administration of ASCs: has pulmonary homing, rescued the suppressive effects of cigarette smoke on bone marrow hematopoietic progenitor cell function [18], restored sustained weight loss [8,18,19], reduced PF score [8,19], increased survival in animal models improved the PF Ashcroft score [8,19], attenuated pulmonary edema [18,20], preserved pulmonary architecture [8,19,21,22,23], reduced allergic symptoms and mucus production [20,22], in addition to exerting protective effects on ALI secondary to pulmonary infection by P. aeruginosa [24,25,26].
In opposition to the study by Feizpour et al. [27], the histopathological endpoints showed that ASC IV, not only reduced inflammatory infiltration [28–31], decreased lung cell death [19,31–34] and increased air space [35,36], but also attenuated the increase in inflammatory cells [28–31] and presented tissue regenerative potential [31–33].
These findings are most likely due to the remodeling capacity of the microenvironment exhibited by ASCs IV [31,37,38] through antioxidant and anti-apoptotic properties by inhibiting IL-4, IL-5, and IL-13 from the Th2 pathway concomitant with the increase in Th1 cytokines [11,12,31,37,38]. Furthermore, ASCS decreased levels of TGF-β, collagen I fibers, apoptotic cells, plasma fibrinogen, PDGF, Von Willebrand factor, NOS-2, FGF7, CC16, CK19, myeloperoxidase, MIP-2 and proteins totals in BALF [13,18–22,39] as well as inhibited: total immune cells, NET formation, fibroblast activation, collagen deposition, epithelial-mesenchymal transition, bacterial loads, iNOS, NFкB and Caspase-3 expression; in addition to significantly increasing the Bcl-2/Bax ratio [24-28,30,35,40-42].
Unlike similar studies that did not review the dosing regimen used, nor its effect on the studied endpoints, the present systematic review suggests that the fastest dose-dependent effect was exerted by cells cryopreserved at the primary site of infection [27] and the high dose showed not only a greater decrease in these parameters but also a low expression of αSMA and reversal of induced histopathological changes [26,43,44].
Therefore, and in accordance with other similar studies, this review suggests: the safety of IV ASCs [39,43–45][31,39,43–45], based on the absence of serious adverse effects or toxicity to their administration, and the applicability of ASCs in ALIs of different pathophysiological mechanisms [5,6,14,20,23,28,29,31,37–39], including severe COVID-19 [1,6,26,40,43]. The physiological rationale reviewed suggests that therapy with ASCs can reduce lung damage in a patient with ARDS from SARS-CoV-2 infection, in addition to promoting leukocyte and lymphocyte recovery with its immunomodulatory and anti-apoptotic effects [12,17,26,40,43].
This study has among its limitations the selection bias, inherent to any non-systematic review; the limitation of most studies to interventions in the early inflammatory phase, offering better support for acute exacerbations to the detriment of its real applicability in the chronic fibrotic phase of the disease; the non-standardization of treatment time and dosage; as well as the lack of methodological rigor of some evidence included by not describing: their MSC surface markers, the parameters used in the analysis of the studies, nor the presence or absence of adverse effects.
Databases used in the present article are the main ones used in similar studies and allow contact with the vast amount of available literature on the subject. However, EMBASE database could not be included since CAPES periodicals does not provide its access through CAFe space. In addition, as it is a topic of recent emergence in the literature and, consequently, has an insufficient amount of clinical evidence for analysis, this study includes narrative reviews and preclinical studies to provide a summary of the currently available evidence on the topic, however, these study types have low-level certainty and high-level biases.
Finally, although the revised clinical data suggests optimism in the applicability of ASCs in other immunoinflammatory diseases [5,6,14–17,20–23,28–31,37–43] the little clinical evidence available about the effectiveness of this treatment lacks standardization, making it difficult to extrapolate its results. Therefore, further studies are needed to be focused on the elaboration of a consensus on the methods of collection of ASCs, the ideal dosage schedule, the most effective time and route of administration, as well as on the definition of indications for the administration of ASCs in cases of COVID-19 for conducting clinical trials soon.
ConclusionThe revised clinical data suggests optimism in the applicability of ASCs in other immunoinflammatory diseases and in severe COVID-19 ARDS. However, further studies are needed to develop a consensus on the methods of collection of ASCs, the ideal dosage schedule, the most effective time and route of administration, as well as on the definition of indications for the administration of ASCs in cases of COVID-19 for conducting clinical trials in near future.
Authors’ contributionsBruna Benigna Sales Armstrong: Collected the data, performed the analysis and wrote the paper.
Juan Carlos Montano Pedroso: Supervised the project, revised it critically for important intellectual content and made a substantial contribution to the interpretation of data.
José da Conceição Carvalho Jr.: Supervised the project, revised it critically for important intellectual content and made a substantial contribution to the interpretation of data.
Lydia Masako Ferreira: Conceived and designed the review, supervised the project, revised it critically for important intellectual content, and gave the final approval of the version to be published. All authors reviewed the results and approved the final version of the manuscript
Financial support and sponsorshipNone.
None.