


Endometriosis is a chronic inflammatory disease affecting about 10% of women of reproductive age. Endometrioma is the most common presentation of endometriosis in ovaries.
ObjectivesHerein, the authors study the effect of the ultrasound-guided ethanol retention technique for endometrioma sclerotherapy and its effect on the plasma levels of pro-inflammatory cytokines.
Materials and methodsEach endometrioma was aspirated and washed with 0.9% saline until clearance and then 2/3 of the cyst volume was filled with ethanol 98%. Patients were followed for 3 months. After that, changes in their cyst diameter, dyspareunia, dysmenorrhea, and antral follicular count were assessed. Also, the sera levels of Interleukin 1β (IL-β), IL-6, and IL-8 were assayed before and after the treatment. The primary sera levels were also compared with a control group.
ResultsIn the treatment and control groups, 23 and 25 individuals (respectively) with a matched mean age (p-value = 0.680) were enrolled in the study. Among the laboratory variables, IL-1β (p-value = 0.035), as well as AMH (p-value = 0.002), were lower, and IL-6 (p-value = 0.011) was higher in the endometriosis group compared to the controls. Following the treatment, dysmenorrhea, dyspareunia, and the mean diameter of all cysts were significantly (p-values < 0.001) decreased in the treatment group. Also, right (p-value = 0.022) and left (p-value = 0.002) ovaries' antral follicular counts were increased following the treatment. No significant change was found among any of the investigated laboratory levels (p-value > 0.05).
ConclusionEthanol retention method is proven to be safe and could improve the clinical status of patients with endometrioma. Although further studies are necessary.
The presence of endometrial-like tissue in any organ/space other than the uterus has been defined as endometriosis [1]. This disease with a prevalence of up to 18% [2] (average 10%) [3] among women of fertility age is a common gynecologic issue. Also, the prevalence increases up to 42% and 31% in women with chronic pelvic pain and infertility, respectively [2]. The symptoms vary from asymptomatic to severe pelvic pain and infertility. According to the 2008 United States health care costs for diseases report, endometriosis and a chronic disease such as diabetes place an economically same burden as each other with an average of 4000$ [1]. The pathogenesis of endometriosis involves a combination of different pathways occurring within the immune system (inflammation), angiogenesis, and endocrine system. The endometrial tissue could present itself anywhere besides the uterus, activate the immune system, and, therefore, induce an inflammatory response via chemokines, prostaglandins, and cytokines [4]. Studies have shown that the serum/abdominal fluid levels of pro-inflammatory cytokines and chemokines such as Interleukin 1β (IL-1β), IL-6, IL-8, and Tumor Necrosis Factor α (TNF-α) are higher in patients with endometriosis [4–7].
The presence of endometriosis in ovaries might cause a cyst named endometrioma, also known as a chocolate cyst [1]. Despite endometriosis being small lesions for which laparoscopic visualization is the golden standard of diagnosis [8], endometrioma could only be diagnosed via vaginal ultrasound or Magnetic Resonance Imaging (MRI) [9]. It has been shown that excision of endometrioma could negatively influence the ovarian follicular reserve represented by decreased Anti-Müllerian Hormone (AMH) [10].
Accordingly, this study aims to investigate the efficacy of an alternate treatment option, the ultrasound-guided ethanol retention technique for endometrioma sclerotherapy, and its effect on the pro-inflammatory cytokine levels in a setting of a prospective investigation with a 3-month follow-up.
Materials and methodsStudy setting and ethicsThis clinical trial was conducted in a tertiary obstetrics/gynecology hospital in Tabriz, Iran between January 2022 and August 2022. The inclusion criteria were considered as any women aged 18‒49 with the approved diagnosis of endometrioma and a cyst diameter greater than 3 centimeters. The exclusion criteria were active cancer, abnormal CA-125 levels, pregnancy, history of any biological medications such as monoclonal antibodies in the past three months, consumption of any corticosteroids and/or Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) in the past seven days, and cysts bigger than 150 mL. The patients were asked to voluntarily sign a consent form after being explained the aims and methods of the study according to their level of knowledge. This study has been approved by the Medical Ethics Committee of Tabriz University of Medical Sciences (IR.TBZMED.REC.1400.598) and registered in the Iranian Registry of Clinical Trials (IRCT) with approval number IRCT20130115012146N9.
MethodologyAfter meeting the inclusion and exclusion criteria, patients were enrolled in the study. Before the intervention, 5 mL of peripheral blood from the cubital vein was harvested from each patient. Then, they underwent vaginal ultrasound evaluation, and the volume of their cyst(s) was recorded. The fluid was aspirated consequently, and the cyst was washed with 0.9% saline solution until clearance. Finally, ethanol 98% was injected into the cyst(s) equal to 2/3 of its volume and retained there. The patients were followed for three months, after which they underwent another ultrasound investigation and blood sampling. A time interval of three months was set for the follow-up evaluation according to a similar study [11]. Also, before and three months after the intervention patients were asked to declare their dyspareunia and dysmenorrhea on a scale of 1‒10 (10 severe pain, 5 moderate pain, and 1 lowest possible pain). This study also included a control group. This group donated 5 mL of blood and expressed their dyspareunia and dysmenorrhea score. Moreover, their antral follicular counts were investigated using ultrasound.
Healthy control groupIn this study, in order to have a better understanding of the disease effect on the mentioned baseline characteristics, a healthy comparison group, as a control group at baseline was also evaluated. These individuals were assessed for levels of IL-1β, IL-6, IL-8, and AMH. Also, their dyspareunia and dysmenorrhea scores as well as antral follicular counts were investigated and reported.
Enzyme-linked immunosorbent assay (ELISA)The harvested blood samples were centrifuged at 1500 × g for 10 minutes at 4°C and the supernatant (sera) was harvested and stored at -70°C. The levels of IL-1β, IL-6, IL-8, AMH, and CA-125 were assayed by the ELISA method according to each kit manufacturer's instruction.
Statistical analysisAll the demobiographic data were recorded in a Microsoft Excel file by two different individuals and in case of any mismatch, a third person re-checked the issue. The categorical and continuous variables are shown as n (%) and mean ± Standard Deviation (SD), respectively. The Kolmogorov-Smirnov test was used to check the normality assumption. Between-group analysis was performed through independent Student's t-test or Mann-Whitney test as a parametric and non-parametric test, respectively. For before and after analysis, paired t-test or Wilcoxon signed-rank test was used. Also, for the categorical variables, the authors benefited from Chi-Square/Fisher's exact tests. Any p-value less than 0.05 was considered statistically significant.
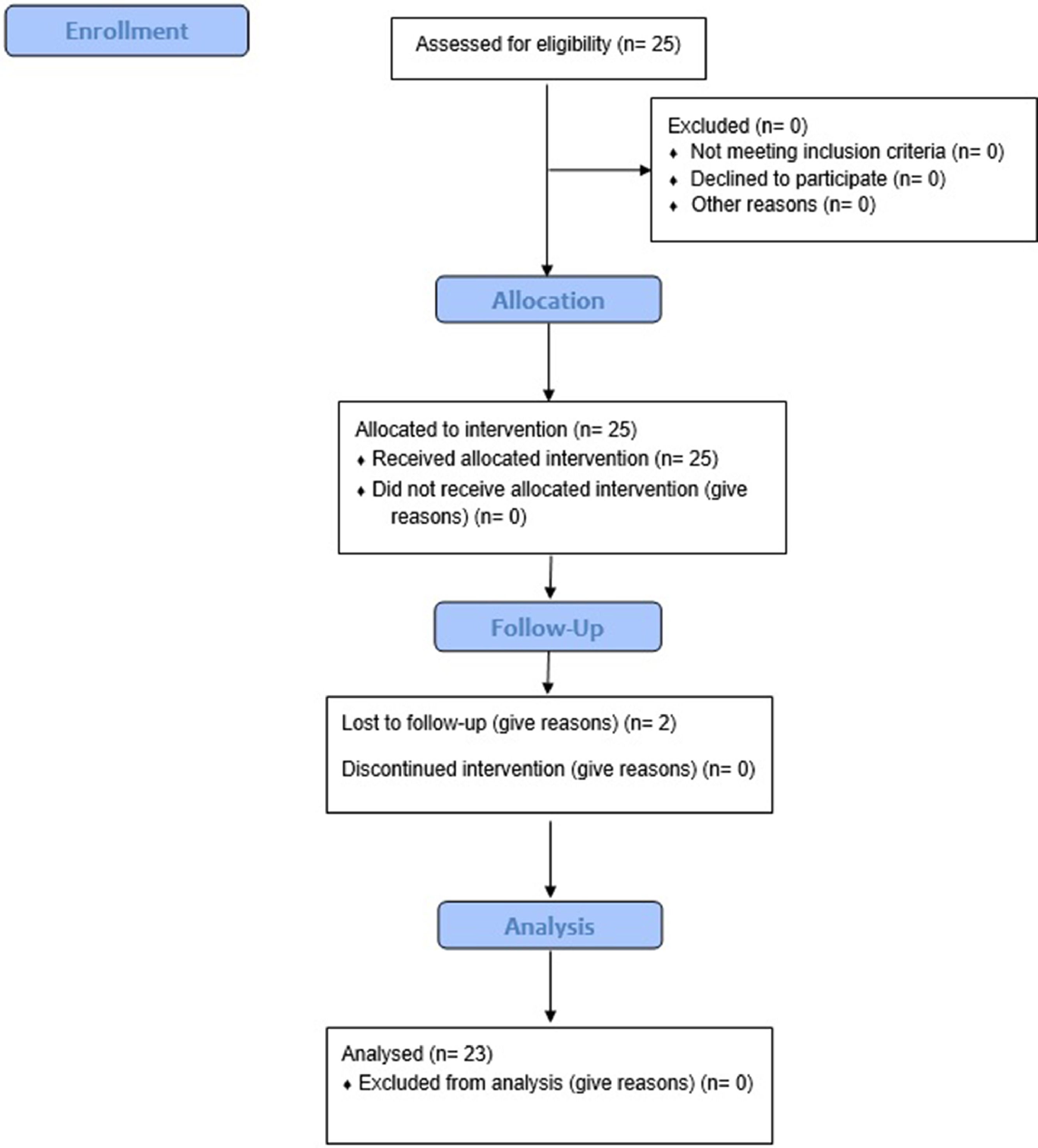
ResultsAfter meeting the exclusion criteria, 23 out of 25 patients (mean age of 35.87 ± 5.11 years) were enrolled in the study (Fig. 1) with a mean infertility duration of 3.70 ± 4.30 years. After vaginal ultrasound evaluation, a total of 37 cysts with a mean volume of 65.45 ± 56.91 mL (mean diameter of 43.24 ± 13.11 mm) were demonstrated in the patient group. The pathology report for all aspirated fluid was compatible with endometriosis accompanied by the finding of “hemorrhagic black ground and hemosiderin-laden macrophages and neutrophils”. The mean age of 25 healthy individuals enrolled in the study was 35.24 ± 5.36 years (other details demonstrated in Table 1). No endometrioma was found in the control group. The scores for dyspareunia and dysmenorrhea in both groups are provided in Table 1.

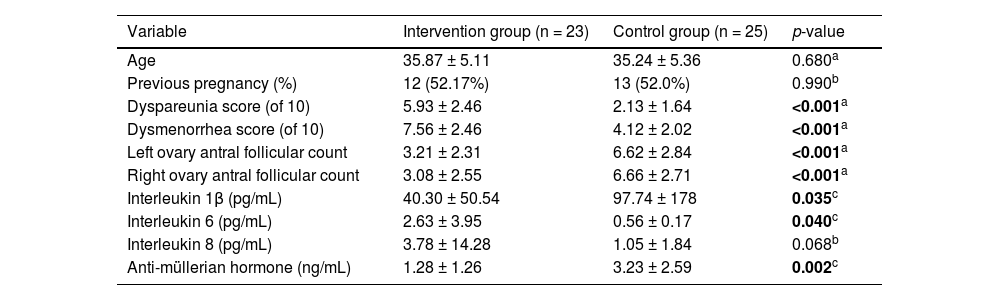
Baseline characteristics between control and intervention groups.
Control group is a healthy compare group, p-value a is calculated based on the independent t-test, p-value b is calculated based on the Chi-Square test, p-value c is calculated based on the Mann Whitney test.
According to the analyses, age and previous pregnancy history were found to not differ significantly between the groups (p-values > 0.05). Considering the clinical symptoms, dysmenorrhea and dyspareunia scores were significantly lower in the control group in comparison to the endometriosis group (p-values < 0.001). Regarding the ultrasound variables, the control group had a significantly higher number of right and left antral follicular counts (p-value < 0.001). Among the laboratory variables, IL-1β (p-value = 0.035), IL-6 (p-value = 0.011), and AMH (p-value = 0.002) were significantly different in the endometriosis group compared to the controls (details have been shown in Table 1).
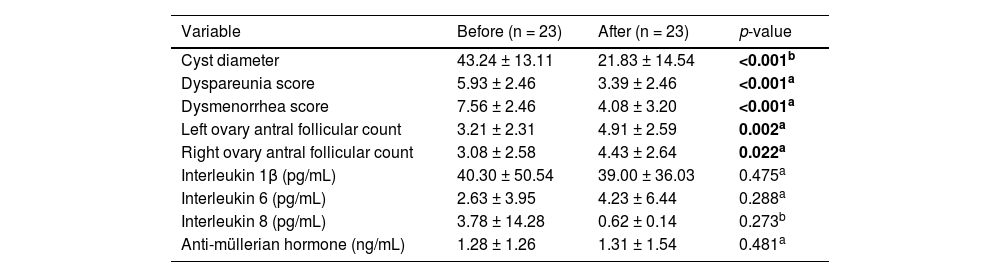
No significant side effect was reported by patients during the follow-up period. Following the ultrasound-guided ethanol retention technique for endometrioma sclerotherapy, the already mentioned variables were investigated in the intervention group. The mean diameter of all cysts was significantly reduced from 43.24 ± 13.11 to 21.83 ± 14.54 mm (p-value < 0.001). Accordingly, the treatment significantly reduced the scores of both dysmenorrhea and dyspareunia (p-values < 0.001). In the ultrasound investigation, it was shown that the right (p-value = 0.022) and left (p-value = 0.002) ovaries' antral follicular counts were increased following the treatment. No significant change was found among the laboratory levels (details have been provided in Table 2).
Statistical comparisons of variables between before and after the intervention (n = 23).
p-value a is calculated based on the paired t-test, p-value b is calculated based on the Wilcoxon signed-rank test.
The current study aimed to investigate the change in the pro-inflammatory profile of patients with endometrioma following receiving ethanol retention sclerotherapy. The levels of IL-1β and IL-6 were detected to be higher in the patients with endometrioma compared to a control group. Also, the treatment didn't change the pro-inflammatory profile in patients. However, statistically significant changes in the cyst diameter, dyspareunia, dysmenorrhea, and ovary antral follicular count were found following the intervention.
In a study on 40 individuals with endometriosis, the serum, and peritoneal levels of IL-1β, IL-6, IL-10, and IL-37 were investigated and compared with 32 healthy controls. According to their analyses, it was shown that the serum and peritoneal levels of IL-1β and IL-10 were not significantly different between controls and patients with endometriosis. On the other hand, the serum and peritoneal levels of IL-6 and IL-37 were significantly higher in the endometriosis group compared to the controls [12]. These findings somehow (except for IL-1β) were compatible with our findings. Another study investigated the serum concentrations of IL-6 and IL-8 in patients with endometrioma and deep infiltrating endometriosis as well as a healthy control group. According to their results, the levels of IL-6 in the sera of patients with endometrioma were significantly higher [13], similar to the results from our study.
To our knowledge, no study has evaluated the differences in sera levels of IL-1β, IL-6, and IL-8 before and after the alcohol retention model. However, in a study comparing the efficacy of ethanol retention and aspiration models, authors have reported reduced pain and increased antral follicular count following the retention technique [14]. Although this study could be considered as a leading research in many aspects, there are still limitations to it among which the most important is the small sample size. Also, not investigating the peritoneal fluid along with serum is considered another limitation. Although the authors studied the most important pro-inflammatory factors associated with endometriosis, more factors could be analyzed which authors suggest for further studies.
ConclusionHerein, it was demonstrated that the ultrasound-guided ethanol retention technique for endometrioma sclerotherapy seems to be a safe method due to no side effects reported by the patients. Although no significant changes were observed in the pro-inflammatory profile of the patients following the treatment, this method was able to reduce cyst diameter, dysmenorrhea, and dyspareunia as well as anincrease in the antral follicular count. The authors suggest further detailed clinical trials on a greater population sample size.
Authors’ contributionsConceptualization: RAA and LF. Investigation: RAA, AG, KH, NN, PH, and LF. Methodology: RAA, LF. Project administration: RAA and LF. Validation: RAA. Supervision: LF. Software: RAA. Writing – original draft: RAA, AG, KH, NN, PH, and LF. Writing – review & editing: RAA, AG, KH, NN, PH, and LF.
Trail registration numberIRCT20130115012146N9.
Medical Ethics Committee approval numberIR.TBZMED.REC.1400.598.
This study was not funded.