



Allergic respiratory diseases such as asthma and allergic rhinitis have increased considerably in the last decades.
ObjectiveThe present study estimates prevalence trends of asthma, allergic rhinitis and pollinosis in the population of a city of Southern Brazil, without restriction of age, from 2011 to 2018, using the ISAAC standardized questionnaire.
MethodsData was collected from March to June of 2011 and during the same months in 2018, in order to verify trends in the prevalence of these allergic conditions. The total sample consisted of 3132 individuals of both sexes living in the municipality of Santo Ângelo, in the state of Rio Grande do Sul, Brazil.
ResultsNo differences were observed in the prevalence of asthma diagnosis (15.1% in 2011 and 13.8% in 2018), however the prevalence of current wheeze was significantly reduced from 24.7% in 2011 to 21.2% in 2018 (p<0.05). Regarding allergic conditions in 2011 and in 2018, a significant reduction was observed (p<0.001) in reported current rhinitis (63.3% vs. 50.5%), rhinoconjunctivitis (48.9% vs. 38.8%), hay fever (52.0% vs. 43.3%), and pollinosis (29.0% vs 17.0%). Moreover, we observed an inverse relation between age and rhinoconjunctivitis and hay fever, and all symptoms were more frequent in females. Rhinoconjunctivitis and hay fever, as well as current rhinitis and pollinosis were highly prevalent among 30–39 years-old individuals, whereas current wheeze affected mainly the age group 10–19 years-old.
ConclusionWhile the prevalence of asthma remained similar after seven years, allergic rhinitis and pollinosis declined between 2011 and 2018.
Allergic respiratory diseases such as allergic rhinitis and asthma are among the most frequent diseases worldwide,1 and co-occurrence of these conditions is often observed in patients.2 Asthma affects approximately 339 million people and is in the top 20 causes of years of life lived with disability.3 In most parts of the world more people are diagnosed with asthma every year, and several contributing factors have been associated to such an increasing trend in the prevalence of asthma.4 For example, a Westernized lifestyle and fast urbanization lead to changes in the environment, changes in diet, greater permanence in closed places, exposure to environmental aeroallergens, and other conditions that have an impact on health conditions such as allergic diseases.1
Although allergies are still attributed mainly to children and adolescents, many adults suffer from allergic disease, however the studies assessing such diseases in adults are rare.4 The appropriate method to estimate trends in prevalence of specific health conditions is to repeatedly survey large random samples in the same area, within the same age-span and with the same validated methods.1,4
Previous studies have described a high prevalence of allergic rhinitis and pollinosis in specific populations in Southern Brazil, whereas the prevalence of asthma seems to be within the national and international average; these studies were conducted with college students,5 army soldiers,6 adolescents aged 13 and 14 years,7 children 6 and 7 years8 and children and adolescents aged 0–15 years in more vulnerable areas and public health coverage.9 In order to gather more information about respiratory allergic conditions, the present study describes the prevalence of asthma, allergic rhinitis and pollinosis in individuals from the municipality of Santo Ângelo, in Southern Brazil, without age restriction, based on the ISAAC questionnaire. Comparing data obtained in 2011 and 2018, the study attempts to show the trends in the prevalence of these conditions in the region.
Materials and methodsStudy design and selection criteriaThe work represents two cross-sectional studies performed in the same location and using the same survey, at two different moments (2011 and 2018). The population was composed of residents of the city of Santo Ângelo, state of Rio Grande do Sul (RS), Southern Brazil. The municipality of Santo Ângelo is located in the Northwestern part of RS, 28°17′56″S, 54°15′46″W, at an altitude of 285m. According to the most recent census of the Brazilian Institute of Geography and Statistics (IBGE), the population was estimated at 76,275 inhabitants.10
Data collection was based on interviews carried out with passers-by in a delimited area of downtown of the city. The sample size was not proportional to the size of the population of the municipality; selection of cases was done without restriction of sex nor age. As an inclusion criterion, the individual should have been a resident of Santo Ângelo for more than two years. The interviews occurred between March and June in the year 2011, and seven years later, during the same months of 2018. At least 1500 individuals were interviewed in each year. Of note, the interviews were undertaken during fall to avoid possible seasonal influences, such as very cold days in the winter or more pollen during spring.
Questionnaire and definitionsData were collected using the standardized ISAAC (International Study of Asthma and Allergies in Childhood) epidemiological questionnaire, developed by Asher et al.11 with the asthma content validated for the Portuguese language by Solé et al.,12 and the allergic rhinitis and pollinosis by Esteves et al.,13 also adapted for application in adults.
The questionnaire included eight questions about asthma and nine questions about allergic rhinitis. Specific definitions used in this study were: current wheeze, which is universally used to identify individuals with active asthma, was evaluated based on the percentage of positive responses to the question “Have you presented wheezing in the past 12 months?”. Asthma diagnosis, which was assessed indirectly by a physician based on the answer to the question “Have you ever had or have asthma?”; and the severity of asthma was considered as intense wheezing in the previous 12 months that could limit speech, as reported by the subject.
Probable asthmatic individuals were those who did not report having or having ever had asthma, but who presented, in the past 12 months: four or more wheezing episodes; or interrupted sleep and with one to three wheezing episodes; or with one to three wheezing episodes without interrupted sleep but with nocturnal cough; or wheezing during exercises, according to previously established criteria.14,15
The prevalence of diagnosed or referred rhinitis was estimated based on positive answers to the question “Have you ever had or have hay fever?”; the question “Have you ever had sneezing and runny nose in the past 12 months?” identified who currently had current rhinitis. Rhinoconjunctivitis was assessed based on the response to “In the past 12 months, has your nose problem been accompanied by itchy-watery eyes?”. In addition, the person who answered “No” to the question “Have you ever had or have allergic rhinitis?”, but also reported sneezing and a runny nose in the past 12 months, accompanied by symptoms of itchy and watery eyes, was classified as a person with probable allergic rhinitis, according to established criteria.14
Pollinosis was evaluated based on individual's answers about pollen allergy during spring. In this sense, individuals who reported pollen allergy associated with nasal and optic allergic symptoms specifically during Spring months (October and November) were considered as having pollinosis.5
All interviewed subjects were invited to participate in the project and to sign the free and informed consent form, and had their questions clarified. If the subject was underage, a parent or guardian signed the informed consent form. All questionnaires correctly completed and with the consent of the individual or parents were included in the study. We excluded the questionnaires that were not adequately filled out, following the same criteria adopted in the research. This study was approved by the research ethics committee of URI (Universidade Regional Integrada) and by the National Ethics Committee (CAAE 66223817.9.0000.5354).
Statistical analysisPrevalence was calculated by dividing the positive responses to a given question by the total validated and completed questionnaires. The chi-squared or Fisher test was used for the categorical data.
Following this initial analysis, a binary logistic regression model was fitted to identify the determinants of the allergic conditions studied, using symptoms and related diagnosis as dependent variables, and year, sex and age as the primary independent variables. The odds ratio (OR) at a 95% confidence interval (CI) was calculated. A p value <0.05 was considered statistically significant for all tests. The SSPSS software version 17.0 for Windows (SPSS, Inc., Chicago, IL, USA) was used for statistical analyses.
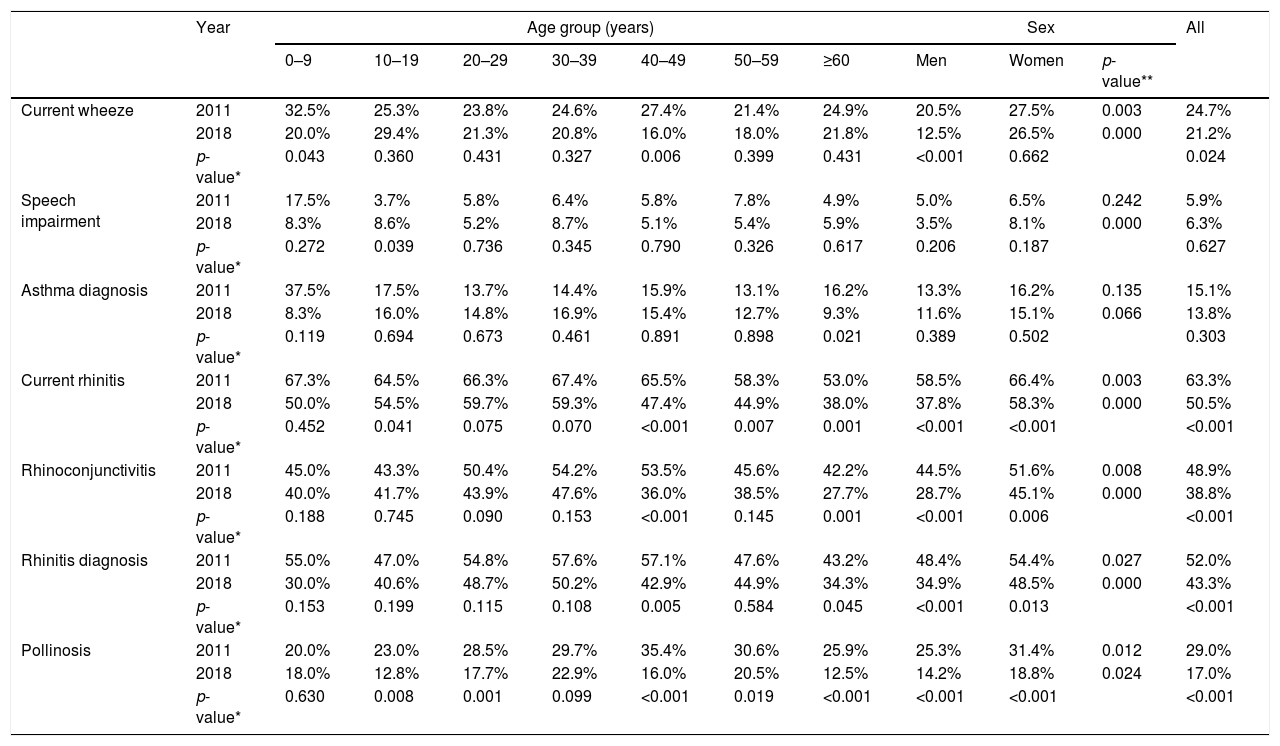
ResultsA total of 3132 individuals were interviewed, and 2882 (92.0%) interviews were validated according to the inclusion criteria, being 1443 in 2011, and 1439 in 2018. Females accounted for 881 (61.1%) and 889 (61.8%) of the validated interviews in 2011 and 2018, respectively. Table 1 presents the distribution of asthma and allergic rhinitis based on affirmative responses to the specific questions contained in the questionnaire.
Prevalence of current wheeze, asthma diagnosis, current rhinitis, rhinoconjunctivitis, rhinitis diagnosis and pollinosis by age groups and sex among all subjects in 2011 (n=1443) and 2018 (n=1439).
| Year | Age group (years) | Sex | All | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0–9 | 10–19 | 20–29 | 30–39 | 40–49 | 50–59 | ≥60 | Men | Women | p-value** | |||
| Current wheeze | 2011 | 32.5% | 25.3% | 23.8% | 24.6% | 27.4% | 21.4% | 24.9% | 20.5% | 27.5% | 0.003 | 24.7% |
| 2018 | 20.0% | 29.4% | 21.3% | 20.8% | 16.0% | 18.0% | 21.8% | 12.5% | 26.5% | 0.000 | 21.2% | |
| p-value* | 0.043 | 0.360 | 0.431 | 0.327 | 0.006 | 0.399 | 0.431 | <0.001 | 0.662 | 0.024 | ||
| Speech impairment | 2011 | 17.5% | 3.7% | 5.8% | 6.4% | 5.8% | 7.8% | 4.9% | 5.0% | 6.5% | 0.242 | 5.9% |
| 2018 | 8.3% | 8.6% | 5.2% | 8.7% | 5.1% | 5.4% | 5.9% | 3.5% | 8.1% | 0.000 | 6.3% | |
| p-value* | 0.272 | 0.039 | 0.736 | 0.345 | 0.790 | 0.326 | 0.617 | 0.206 | 0.187 | 0.627 | ||
| Asthma diagnosis | 2011 | 37.5% | 17.5% | 13.7% | 14.4% | 15.9% | 13.1% | 16.2% | 13.3% | 16.2% | 0.135 | 15.1% |
| 2018 | 8.3% | 16.0% | 14.8% | 16.9% | 15.4% | 12.7% | 9.3% | 11.6% | 15.1% | 0.066 | 13.8% | |
| p-value* | 0.119 | 0.694 | 0.673 | 0.461 | 0.891 | 0.898 | 0.021 | 0.389 | 0.502 | 0.303 | ||
| Current rhinitis | 2011 | 67.3% | 64.5% | 66.3% | 67.4% | 65.5% | 58.3% | 53.0% | 58.5% | 66.4% | 0.003 | 63.3% |
| 2018 | 50.0% | 54.5% | 59.7% | 59.3% | 47.4% | 44.9% | 38.0% | 37.8% | 58.3% | 0.000 | 50.5% | |
| p-value* | 0.452 | 0.041 | 0.075 | 0.070 | <0.001 | 0.007 | 0.001 | <0.001 | <0.001 | <0.001 | ||
| Rhinoconjunctivitis | 2011 | 45.0% | 43.3% | 50.4% | 54.2% | 53.5% | 45.6% | 42.2% | 44.5% | 51.6% | 0.008 | 48.9% |
| 2018 | 40.0% | 41.7% | 43.9% | 47.6% | 36.0% | 38.5% | 27.7% | 28.7% | 45.1% | 0.000 | 38.8% | |
| p-value* | 0.188 | 0.745 | 0.090 | 0.153 | <0.001 | 0.145 | 0.001 | <0.001 | 0.006 | <0.001 | ||
| Rhinitis diagnosis | 2011 | 55.0% | 47.0% | 54.8% | 57.6% | 57.1% | 47.6% | 43.2% | 48.4% | 54.4% | 0.027 | 52.0% |
| 2018 | 30.0% | 40.6% | 48.7% | 50.2% | 42.9% | 44.9% | 34.3% | 34.9% | 48.5% | 0.000 | 43.3% | |
| p-value* | 0.153 | 0.199 | 0.115 | 0.108 | 0.005 | 0.584 | 0.045 | <0.001 | 0.013 | <0.001 | ||
| Pollinosis | 2011 | 20.0% | 23.0% | 28.5% | 29.7% | 35.4% | 30.6% | 25.9% | 25.3% | 31.4% | 0.012 | 29.0% |
| 2018 | 18.0% | 12.8% | 17.7% | 22.9% | 16.0% | 20.5% | 12.5% | 14.2% | 18.8% | 0.024 | 17.0% | |
| p-value* | 0.630 | 0.008 | 0.001 | 0.099 | <0.001 | 0.019 | <0.001 | <0.001 | <0.001 | <0.001 | ||
No significant changes were observed for asthma diagnosis in the years studied (15.1% in 2011 vs. 13.8% in 2018), nor for speech impairment (5.9% in 2011 vs. 6.3% in 2018) (Table 1). On the other hand, the prevalence of current wheeze was higher in 2011 than in 2018 (24.7% vs. 21.2%, p=0.024), indicating a slight decrease of current wheeze in the population. It was noteworthy that current wheeze was more common among people in the age groups 0–9 and 10–19 years old.
Rhinitis, rhinoconjunctivitis and pollinosis also decreased significantly in the population in the period. Nasal symptoms indicative of current rhinitis were reported by 63.3% of the individuals in 2011, and 50.5% in 2018 (p<0.001); it should be highlighted that rhinitis was more common among young adults, affecting 67.4% of the individuals in the age group 30–39 years old in 2011, and 59.7% of the individuals in the age group 20–29 years old in 2018. Regarding allergic rhinitis (ever in life), 52.0% and 43.3% of the individuals were diagnosed with that condition in 2011 and 2018, respectively (p<0.001); and it was also more frequent among 30–39 years old people. The prevalence of rhinoconjunctivitis (sneezing, runny nose accompanied by eye itching and watery eyes) was also higher in 2011 than in 2018 (p<0.001), being more frequent among people 30–39 years old. Pollinosis was reported by 29.0% of the individuals interviewed in 2011, and by 17.0% in 2018 (p<0.001), with higher frequency in the age groups 40–49 years in 2011 (35.4%), and 30–39 years in 2018 (22.9%).
The prevalence values were higher in females than in males for most of the variables analyzed, except for speech impairment and asthma diagnosis in 2011, in which no significant differences were found despite more women answering positively for these parameters.
When analyzing the distribution of nasal and ocular symptoms during the months of the year (Fig. 1), a significant reduction of symptoms is observed from 2011 to 2018, mainly during the spring months (September with 47.6% vs. 30.9%, and October 38.9% vs. 24.3%, November 23.4% and 10.4%; p<0.001).
.")
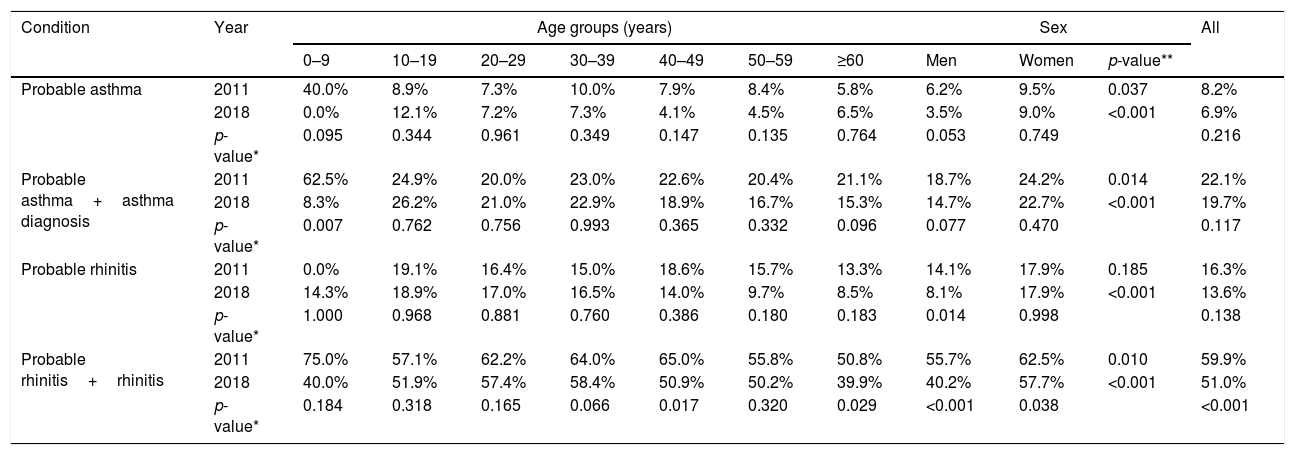
The prevalence of affirmative answers to questions that indicate probable asthma and probable rhinitis is shown in Table 2. No significant changes were observed throughout the period for probable asthma (8.2% in 2011 vs. 6.9% 2018; p=0.216), probable asthma combined with asthma diagnosis (22.1% in 2011 vs. 19.7% in 2018; p=0.117), or probable allergic rhinitis (16.3% in 2011 vs. 13.6% in 2018; p=0.138). However, a significant decrease was observed from 2011 to 2018 when probable allergic rhinitis was considered together with rhinitis diagnosis (59.9% in 2011 vs. 51% in 2018; p<0.001).
Prevalence of probable asthma and allergic rhinitis by age groups and sex among all subjects in 2011 (n=1443) and 2018 (n=1439).
| Condition | Year | Age groups (years) | Sex | All | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0–9 | 10–19 | 20–29 | 30–39 | 40–49 | 50–59 | ≥60 | Men | Women | p-value** | |||
| Probable asthma | 2011 | 40.0% | 8.9% | 7.3% | 10.0% | 7.9% | 8.4% | 5.8% | 6.2% | 9.5% | 0.037 | 8.2% |
| 2018 | 0.0% | 12.1% | 7.2% | 7.3% | 4.1% | 4.5% | 6.5% | 3.5% | 9.0% | <0.001 | 6.9% | |
| p-value* | 0.095 | 0.344 | 0.961 | 0.349 | 0.147 | 0.135 | 0.764 | 0.053 | 0.749 | 0.216 | ||
| Probable asthma+asthma diagnosis | 2011 | 62.5% | 24.9% | 20.0% | 23.0% | 22.6% | 20.4% | 21.1% | 18.7% | 24.2% | 0.014 | 22.1% |
| 2018 | 8.3% | 26.2% | 21.0% | 22.9% | 18.9% | 16.7% | 15.3% | 14.7% | 22.7% | <0.001 | 19.7% | |
| p-value* | 0.007 | 0.762 | 0.756 | 0.993 | 0.365 | 0.332 | 0.096 | 0.077 | 0.470 | 0.117 | ||
| Probable rhinitis | 2011 | 0.0% | 19.1% | 16.4% | 15.0% | 18.6% | 15.7% | 13.3% | 14.1% | 17.9% | 0.185 | 16.3% |
| 2018 | 14.3% | 18.9% | 17.0% | 16.5% | 14.0% | 9.7% | 8.5% | 8.1% | 17.9% | <0.001 | 13.6% | |
| p-value* | 1.000 | 0.968 | 0.881 | 0.760 | 0.386 | 0.180 | 0.183 | 0.014 | 0.998 | 0.138 | ||
| Probable rhinitis+rhinitis | 2011 | 75.0% | 57.1% | 62.2% | 64.0% | 65.0% | 55.8% | 50.8% | 55.7% | 62.5% | 0.010 | 59.9% |
| 2018 | 40.0% | 51.9% | 57.4% | 58.4% | 50.9% | 50.2% | 39.9% | 40.2% | 57.7% | <0.001 | 51.0% | |
| p-value* | 0.184 | 0.318 | 0.165 | 0.066 | 0.017 | 0.320 | 0.029 | <0.001 | 0.038 | <0.001 | ||
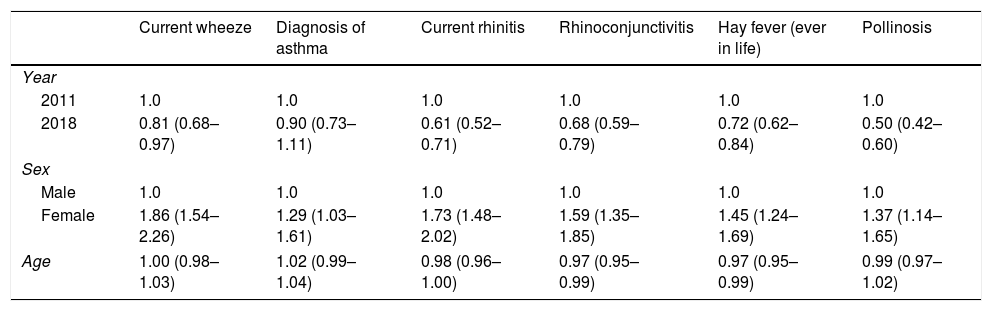
After completing an adjusted analysis, the results were consistent with binary logistic regression. As seen in Table 3, there was a decreased risk of current wheeze, current rhinitis, rhinoconjunctivitis, hay fever and pollinosis from 2011 to 2018, while there was non-significant association between diagnosis of asthma and the year of analysis. For all parameters analyzed, prevalence values were higher for females compared to males. With regards to age, a decreased relation was observed for rhinoconjunctivitis and hay fever.
Binary logistic regression between calendar year, sex, and age with self-reported current wheeze, diagnosis of asthma, current rhinitis, rhinoconjunctivitis, hay fever (ever in life) and pollinosis.
| Current wheeze | Diagnosis of asthma | Current rhinitis | Rhinoconjunctivitis | Hay fever (ever in life) | Pollinosis | |
|---|---|---|---|---|---|---|
| Year | ||||||
| 2011 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| 2018 | 0.81 (0.68–0.97) | 0.90 (0.73–1.11) | 0.61 (0.52–0.71) | 0.68 (0.59–0.79) | 0.72 (0.62–0.84) | 0.50 (0.42–0.60) |
| Sex | ||||||
| Male | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| Female | 1.86 (1.54–2.26) | 1.29 (1.03–1.61) | 1.73 (1.48–2.02) | 1.59 (1.35–1.85) | 1.45 (1.24–1.69) | 1.37 (1.14–1.65) |
| Age | 1.00 (0.98–1.03) | 1.02 (0.99–1.04) | 0.98 (0.96–1.00) | 0.97 (0.95–0.99) | 0.97 (0.95–0.99) | 0.99 (0.97–1.02) |
In the present study, the ISAAC questionnaire was adapted to assess symptoms indicative of asthma, rhinitis and pollinosis in people of all ages living in a city in Southern Brazil. Notably, when comparing answers obtained in 2011 and in 2018, we observed a reduction of cases of current rhinitis, diagnosis of allergic rhinitis and pollinosis after a seven-year period, whereas the diagnosis of asthma maintained its prevalence, despite a decrease in reports of current wheeze. In a similar study conducted in Chile with young adults from a semi-rural area, after a 10-year follow-up period the number of cases of asthma remained stable, and current wheeze decreased; however, different from our study, an increase in rhinitis and rhinoconjunctivitis was observed.16 Another study carried out in Sweden with 20–69 years old adults, reported an increase in asthma between 1996, 2006, and 2016 (8.4%, 9.9%, 10.9%, respectively), and an increase in allergic asthma.1 Interestingly, a gradual increase in reports of asthma was observed between the 1960s and 1990s worldwide, reaching stable incidences especially in Western countries such as Australia and some European countries. In contrast, in countries where urbanization and industrialization increased considerably in the beginning of the 21st century, such as China and middle- and low-level income countries, the prevalence of asthma continues to raise.1,4
In Latin America, the prevalence of current wheeze increases were higher: 0.32% per year for adolescents and 0.07% per year for children aged from 6 to 7 years.17 Differences in the prevalence of asthma between different regions in Brazil may occur depending on environmental and social factors. Therefore, while in some Brazilian regions increases in the number of cases of asthma and allergic rhinitis can be observed, in others, as shown in our study, stabilize or even decrease. Accordingly, based on the ISAAC protocol, a decrease in current wheeze was observed in adolescents 13–14 years old in Brazil from 2003 to 2012 (18.5% vs. 17.5%); on the other hand, the prevalence of severe asthma and asthma diagnosis increased (14.3% vs. 17.6%), as well as the prevalence of rhinitis, rhinoconjunctivitis and atopic dermatitis.18
In a previous study with the adult population (20–69 years) in Southern Brazil, the prevalence of asthma diagnosis was 14.3%,19 results similar to those obtained in the present study with individuals of all age groups (15.1% in 2011 and 13.8% in 2018), as well as to the national average of 13%, according to the WHS.20 With regard to current wheeze, Brazil occupies the fourth place with a prevalence of 22.6%, which is similar to our findings (24.7% in 2011 and 21.2% in 2018).20 Of note, the global average of asthma diagnosis is 4.3%, while for current wheeze the prevalence is 8.6%.20
Another finding of this study that corroborates other studies with adults is that cases of current wheeze,19,21 allergic rhinitis and asthma diagnosis are mainly associated with the female sex.1,16,22,23 With regard to age, the highest prevalence of asthma was observed in the age group 10–19 years, as opposed to a study in five Middle Eastern countries in which a higher prevalence was observed among individuals older than 50 years.21 For rhinoconjunctivitis, we found the highest prevalence among individuals 30–39 years old; a study in Sweden found a higher prevalence of asthma and allergic rhinoconjunctivitis in the age group 20–29 years.1 It is noteworthy that we observed an inverse correlation between age and rhinoconjunctivitis and hay fever.
Allergic rhinitis is closely linked to various comorbidities, especially asthma.24,25 In the United States, the National Health and Nutrition Examination Survey (NHANES) estimates that the prevalence of allergic rhinitis in the population is 23.5%, reaching 31.3% among 40–49 years old individuals.23 Reports by the ECRHS have shown variable prevalence of nasal allergy depending on the geographical region, ranging from 11.8% in Oviedo, Spain, to 46% in Melbourne, Australia.26 It is important to take into account the fact that the number of cases of allergic rhinitis has increased significantly in countries with a previous low prevalence.2
In our study, despite the fact that we found numbers of cases of asthma within the national average,19,20 the high prevalence of allergic rhinitis diagnosis (52% in 2011 and 43.3% in 2018) represents a risk for asthma. Previous studies in the region have found high rates of allergic rhinitis in children of six and seven years,8 adolescents of 13 and 14 years7 and college students.5 It has been estimated that one in two cases of rhinitis can present symptoms of asthma, depending on the severity of the allergic rhinitis24; in addition, nasal symptoms are exhibited by up to 85% of the patients that have asthma.2
Pollinosis is an allergic condition that deserves attention in a local context because of the high index found in our region, representing a health burden.5,6,9 With increased exposure to antigens during life, pollinosis occurs mainly in the young adult,6 therefore, it was considered necessary to apply the ISAAC questionnaire to the population in all age groups, to estimate the real prevalence not only of asthma and allergic rhinitis, but including pollinosis. For the analysis of pollinosis in this study, the residence time in the city was restricted to two or more years. This was necessary since, in order to be sensitized, previous contact with pollen antigens is assumed, and the symptoms will be characterized within the researched environment. The question to individuals about pollen allergy in the spring has no diagnostic value, especially in regions where people do not have symptoms during the months of pollen dispersal.5 To determine the prevalence of pollinosis in the present study the question was asked “have or had allergy to spring pollen”, this issue was analyzed in conjunction with the positive response for the spring months (October and November) and rhinoconjunctivitis in the past 12 months.
The prevalence of pollinosis differs according to the geographic position, vegetation, climate and age of the groups surveyed. In a survey carried out with militaries from two different regions in RS, namely Pampa and Missões, the index of pollinosis was 3.2% and 21.6%, respectively.6 In the present study, conducted in Santo Angelo, a city in the Missões region, the pollinosis index in the general population was 29.0% in 2011 and 17.0% in 2018.
The increase of the population density and the life styles in different regions are aspects used to explain the occurrence of the variability of the prevalence of current wheeze and allergic rhinitis between different studies.4,27,28 Some factors may contribute to the protection against asthma and allergic rhinitis, such as: reduction of early exposure to infections (avoidance due to non-cohabitation of children in day-care centers), growing up on a farm with livestock, reduced exposure to aeroallergens.29 In contrast, individuals (adults and children) moving to urban areas29 or close to a major road28 may have an increased risk of current wheeze, atopy and mainly of pollinosis.
Another fact that may justify the high occurrence of allergic rhinitis, especially pollinosis, would be annual ryegrass (Lolium multiflorum). In Southern Brazil, L. multiflorum, known as annual ryegrass, is used as pasture and forage, constituting one of the main pollinating grasses.30L. multiflorum is desiccated during its final development cycle with the use of herbicide, serving as a soil cover basis for summer crops such as soybean and corn. Ryegrass remains in the soil annually and has a natural semination, its pollen is anemophilous and highly allergenic5; hence, the introduction of L. multiflorum in extensive agricultural areas, close to the population of many cities of our region, may pose an as yet unassessed and unmeasured environmental and health impact.6
The increase in pollinosis prevalence during spring is accompanied by an increase in nasal and ocular symptoms, which are important characteristics of pollinosis; accordingly, in the present these symptoms were observed mainly in September, a month of high pollination, reaching a prevalence index of 48.7% in 2011 and 30.7% in 2018. A previous study performed in 2004 assessed pollinosis in university students living in two different municipalities in RS: Caxias do Sul, a city of high urbanization and industrial activity, and Santo Ângelo, which is a smaller town with an economy based mostly on agriculture; the results were similar, with peaks in pollinosis prevalence during the spring and index values of 40.3% and 41.6% in Caxias do Sul and Santo Ângelo, respectively.5 Another study, which analyzed pollinosis in soldiers in RS also demonstrated a high increase of the symptoms in the month of September, with a decline in the following months6; accordingly, our results show a marked decline in pollinosis symptoms in December and January. The decrease in pollinosis coincides with the decrease in pollen concentration of grasses; possibly as early as October there is the extensive drying of L. multiflorum for planting soybean in the region.6
Validity and limitations of the studyThis study analyzed data from individuals of all ages, including adults over 60 years. It is important to consider chronic obstructive pulmonary disease (COPD) as a possible confounder in the elderly, and because COPD is commonly under-diagnosed, it can be easily misclassified as asthma.1,4,20 Notwithstanding, our study addresses the complaint of allergic respiratory symptoms in our community in different age groups,5–8 as high prevalence was found for conditions such as asthma, allergic rhinitis, and mainly pollinosis.
Another limitation of this study was the lack of information about certain life-style factors, such as smoking. In Brazil, the use of tobacco in an active and passive way has presented a reduction in recent years: in 2011, the percentage of the male and the female population considered active smokers in Brazilian was 16.5% and 10.7%, respectively, whereas in 2017 the frequency was 13.2% for males and 7.5% for females.31
Other risk factors that may influence outcomes are obesity and environmental pollution. In this sense, the study that evaluated pollinosis in students living in Caxias do Sul and Santo Ângelo also assessed allergic rhinitis; surprisingly, the number of cases for both conditions was greater in Santo Ângelo,5 reflecting the importance of other variables in the development of allergic conditions. In addition, recent studies have shown a relationship between obesity and asthma, but it is not related to cases of allergic rhinitis and atopy.32
We also have to take into account that the present study did not differentiate atopic from non-atopic rhinitis due to the lack of atopy tests such as the Skin Prick Test; nonetheless, the questionnaire on rhinitis has been validated to assess the presence of atopy.26 Moreover, we used a standardized questionnaire to identify individuals with asthma, allergic rhinitis and pollinosis in a fast, effective and low-cost way. Though the global prevalence of asthma and allergic rhinitis might be overestimated when assessed through a questionnaire about respiratory symptoms, the clinical definition can underestimate these diseases mainly in low-income countries where access to health care conditions are difficult or limited.20
Our results showed that the prevalence of asthma was maintained over seven years (2011–2018), and current wheeze was shown to be declining. It should be noted that allergic rhinitis and pollinosis, which are public health problems with high prevalence mainly in middle-aged adults, presented a decline from 2011 to 2018. Other epidemiological studies should be carried out to clarify other factors such as the relationship between pollen diseases and ryegrass and changes in agricultural practices.
This study has served as a model for other analyses that can be performed in other geographical regions, especially where conditions are similar to our region and regional and multidisciplinary studies are required to offer a contribution to the community and a better quality of life to the carriers of allergic diseases and asthma.
Funding and contributorsThis work was supported by the research support program of Fundação Regional Integrada (FuRI) from Universidade Regional Integrada (URI).
Conflict of interestThere is no conflict of interest in submission of this manuscript.
To each person who gave five minutes of their time to participate in this work.
