



The studies that have evaluated the effectiveness of bilateral cochlear implantation in children suggest an improvement in hearing about sound localisation and speech discrimination. In this paper we show the differences in audio-linguistic achievements with early bilateral cochlear implantation versus unilateral, and differences between simultaneous and sequential bilateral implantation.
Material and methodsWe present 88 children with bilateral profound sensorineural hearing loss, treated with bilateral cochlear implantation in 32 cases and unilateral in 56 cases, during the first 12 months (27 children) of life and between 12 and 24 months (61 children). We conducted a statistical comparison of both groups in the audiometry, IT-Mais, Nottingham, LittlEars scales and verbal tests.
ResultsNo significant differences in hearing thresholds and questionnaires between unilateral and bilateral implantation were detected in either the first or second year. Verbal tests do show statistically significant differences: children with bilateral cochlear implant obtain 100% recognition of disyllabic and phrases within 2–3 years after implantation whilst children with one implant do not obtain those results at 5 years after surgery. No differences between simultaneous and sequential bilateral implantation were detected.
ConclusionWe emphasise the importance of ensuring good early audiological screening, to carry out an early and bilateral cochlear implantation with the consequent development of audio-language skills similar to normal hearing children.
Los estudios que han evaluado la efectividad de los implantes cocleares bilaterales en niños sugieren una mejoría de la capacidad auditiva en cuanto a la localización del sonido y la discriminación del lenguaje. En este trabajo mostramos las diferencias en los logros audio-lingüísticos con la implantación coclear bilateral precoz frente a la unilateral, así como las diferencias entre la implantación bilateral secuencial y simultánea.
Material y métodosPresentamos 88 niños diagnosticados de hipoacusia neurosensorial profunda bilateral tratados mediante implantación coclear bilateral en 32 casos, y unilateral en 56 casos, durante los primeros 12 meses (27 niños) y entre los 12 y 24 meses (61 niños). Se compararon los resultados en la audiometría tonal, en las escalas IT-Mais, Nottingham y LittlEars, así como en las pruebas logoaudiométricas.
ResultadosNo se detectan diferencias significativas en los umbrales auditivos y en los cuestionarios IT-Mais, Nottingham y LittlEars entre los niños implantados bilateral y unilateralmente, tanto en el primer como en el segundo año. Las pruebas verbales sí que muestran diferencias estadísticamente significativas, ya que los niños con un implante coclear bilateral alcanzan antes el 100% en el reconocimiento de bisílabos y frases, sin que los niños con un solo implante lleguen a igualar dichos resultados a los 5 años de la cirugía. No existen diferencias entre implantación bilateral simultánea y secuencial.
ConclusiónCon este estudio remarcamos la importancia de asegurar un buen cribado audiológico precoz, para poder llevar a cabo una implantación coclear temprana, a ser posible bilateral, logrando así un desarrollo de las habilidades audio-lingüísticas equiparable al de los normooyentes.
Prelingual type hearing impairment is when the hearing impairment occurs prior to the acquisition of language, i.e. before 2 years of age. Should this impairment be severe or profound, it will lead to serious repercussions in language development, which takes place up to the age of 5. Language is such a powerful tool that its dysfunction may negatively affect total cognitive economy. Restrictions predominantly occur in the development of oral communication. Without a good oral language base learning to read is profoundly hindered and without powerful language and reading ability thoughts cannot be expressed. The outcome will be inequality in social circumstances, in education, at work and also social isolation. Those affected by a prelingual type hearing impairment who undergo surgery, in this case with a cochlear implantation, are able to benefit from a wide range of benefits, outreaching mere hearing perception.
Overall evaluation of the long term outcome of cochlear implantation in a sample of children up to and including 6 years of age, reveals that most children are able to recognise the spoken word in an open context without the visual support of lip reading or gestures.1–5 Results also suggest that children who were given implantations earlier, before the age of 3, have greater possibilities of dominating these skills and a better development of the spoken language.6–8 However, as implantation age goes beyond the critical period when the auditory pathway is able to develop its greatest potential of flexibility and learning – usually approximately the first 5 or 6 years of age – results may suffer serious individual variations derived from medical factors and from the educational and physiotherapeutic attention the child receives following implantation.
We should also perform bilateral cochlear implantation on these prelingual hearing impairments, whether simultaneously or sequentially. The reasons for considering a second cochlear implantation include: the possibility of using the ear with better hearing, improving the localisation of sounds, avoiding head shade effect and improving word perception in noise, in addition to capturing a bilateral stimulation of the pathways and auditory centres during the period of the greatest neuroplasticity. One should recall that the auditory system is anatomically and functionally prepared to receive stimuli from outside from both ears under normal conditions. For this reason, intervention of the pathways and centres which comprise this system confer the binaural auditory perception with a series of advantages against monaural hearing.9
The aim of this paper is to evaluate the auditory and linguistic outcome obtained in children diagnosed with congenital hearing impairment and treated with a cochlear implant between the ages of one and two years, and to make a comparison of said outcome between those children who received bilateral implants and those who received unilateral implants.
Material and MethodsA longitudinal observational and retrospective study which included a total of 88 children from the screening programme, from 1999 until 2014, presenting with a diagnosis of cognitive hearing impairment and who were divided into 2 groups according to implantation age: children who received implantations between the ages of 12 and 24 months, a total of 61 patients and the group of 27 children who received implantations before they reached the age of 12 months. They were also divided into another 2 groups depending on whether implantation was unilateral or bilateral: 32 children had bilateral implantations compared with 56 who had unilateral implantations. All the children were assessed during the first 6 months and subsequently at yearly intervals for 5 years after implant activation.
Inclusion criteria were as follows: all children were diagnosed with profound bilateral hearing impairment with thresholds over 90dB, with or without the minimum benefit of audiphones (with thresholds to conversational frequencies over 50dB in behavioural hearing tests or from visual reinforcement). Furthermore, a psychological and neurological assessment was made prior to this to confirm the benefit which the implantation afforded, and imaging studies using computerised tomography and MRI to demonstrate the existence of a sufficiently developed cochlear for holding the electrode and the presence of the cochlear nerve.
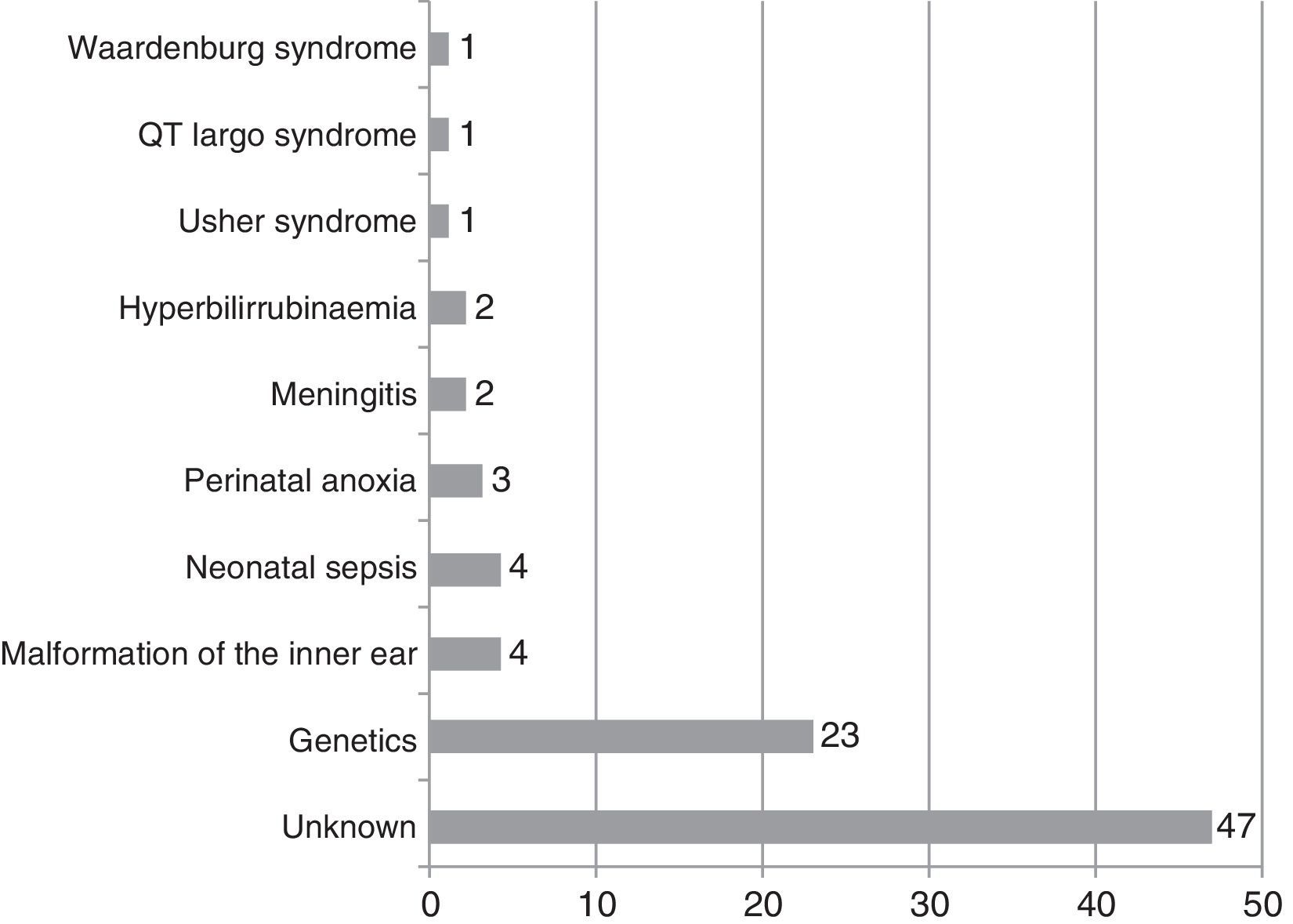
With regard to the hearing impairment aetiology, this was unknown in the majority of cases and of genetic origin in 23 patients, of whom 13 demonstrated a mutation in the gene coding connexin 26 gene and otoferlin. The other causes are shown in Fig. 1.

Pure tone liminar audiometry was included in all post-operative assessments at 6 months, although these children needed some play time first for a sufficiently reliable result. These audiometries were carried out in a soundproof booth, in open spaces, and one metre distance from the source of the sound, with sound modulation and no background noise. The following diverse tests were also included in this assessment: the IT-Mais scale, which measures the behaviour of the child to sound in everyday life situations and which assesses 10 items graded from 0 to 4; the Nottingham auditory performance scale, which assesses 8 categories, the first of which corresponds to a complete inability to perceive environmental sounds, despite appropriate prosthesis fitting, and the last of which corresponds to the child's ability to maintain a telephone conversation with an unknown interlocutor and on an unfamiliar subject; and the LittlEars questionnaire, which is filled in by the parents and which assesses audiocommunicative improvements with the cochlear implantation using 35 items. Finally, the individual hearing level tests (two syllables and sentences); these were carried out without the help of lip reading and in an open context, at one metre's distance and an intensity of 65dB with no background noise. The two syllable test consisted of 8 lists of 20 words forming part of a child's vocabulary. The sentence test comprised 3 lists of 6 sentences each, with 4 key words, and required certain short term auditory memory skill. In order to carry out these tests, it is necessary for the child to have a certain level of oral language development. In the majority of cases these tests therefore had to be conducted after the implantation had been activated for 2 years.
The Student's t-test was systematically applied to observe the differences between performance between the 2 age groups and the 2 groups divided according to number of implantations. Samples were previously standardised and statistical significance was established as P<.05.
ResultsThe minimum age of implantation was 9 months. The mean age of implantation was 11.9 (±0.8) months in those operated on when they were one and 18 (±2.6) months on those operated on when they were two.
Regarding bilateral implantation, 14 of the 27 patients formed part of the group of those under one year who received cochlear implants in both ears, simultaneously in 6 cases and sequentially in the remaining 8. Of the 61 patients who received implants in the first 2 years of life, 18 were bilateral and of those 7 were simultaneous and 11 sequential.
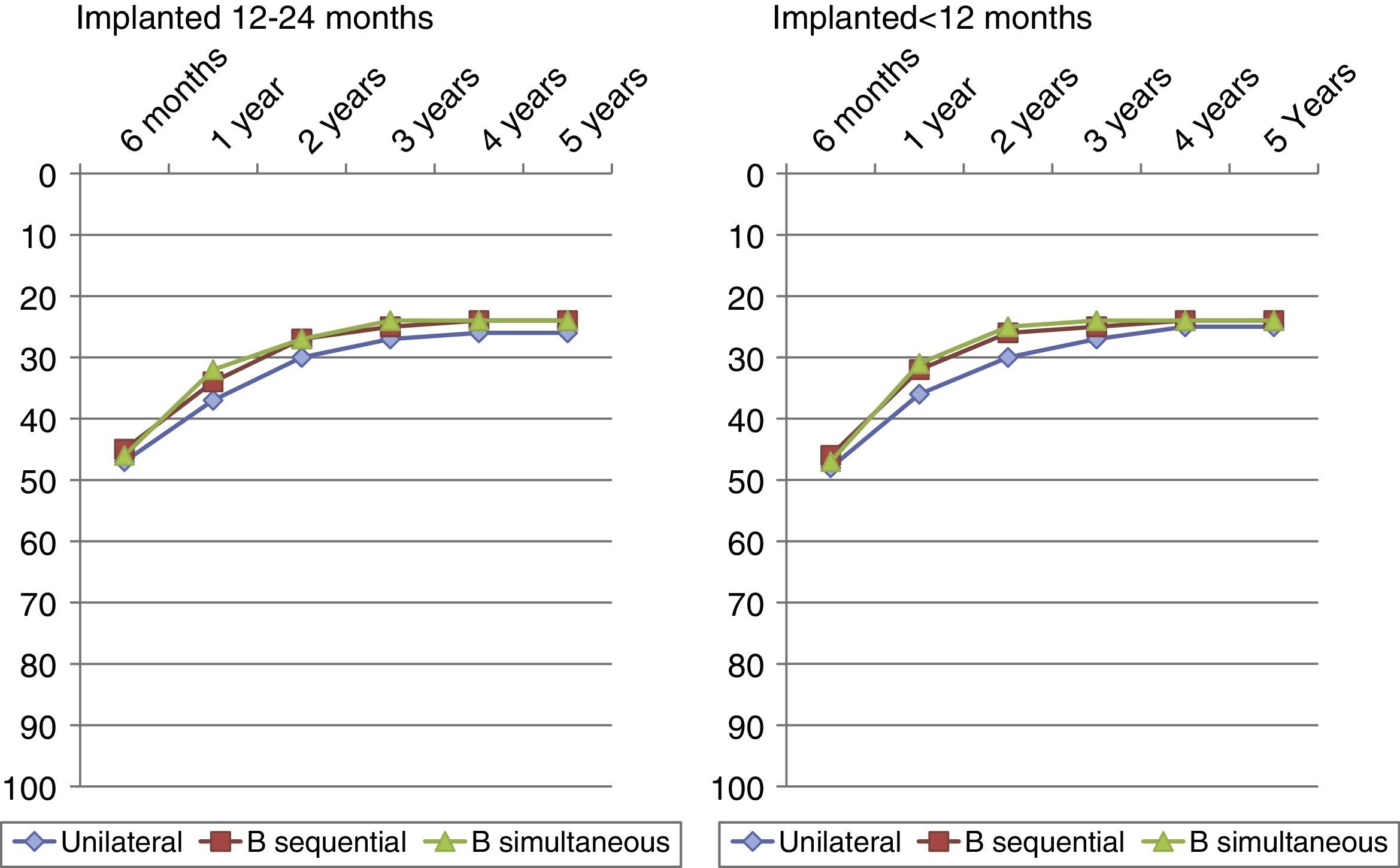
Fig. 2 shows the mean auditory thresholds in each age group throughout our study. These thresholds in both the group with implantations during their first year of life and those with implantations between 12 and 24 months, obtained similar values, of around of 25±dB after 3 years of cochlear implantation, and maintained stability over time. We find there is a similar situation if we compare the average thresholds obtained by children with unilateral implants compared to those with bilateral implants. The Student's t-test for comparing audiometric thresholds of the different groups did not show up any statistically significant differences between any of them, with significance level results above those established in this study (P>.05).

Average hearing thresholds obtained in children with a single implant compared with bilateral implants, sequentially and simultaneously implanted, 5 years after surgery, comparing those who received the implant during their first year of life and those who received it when they were two.
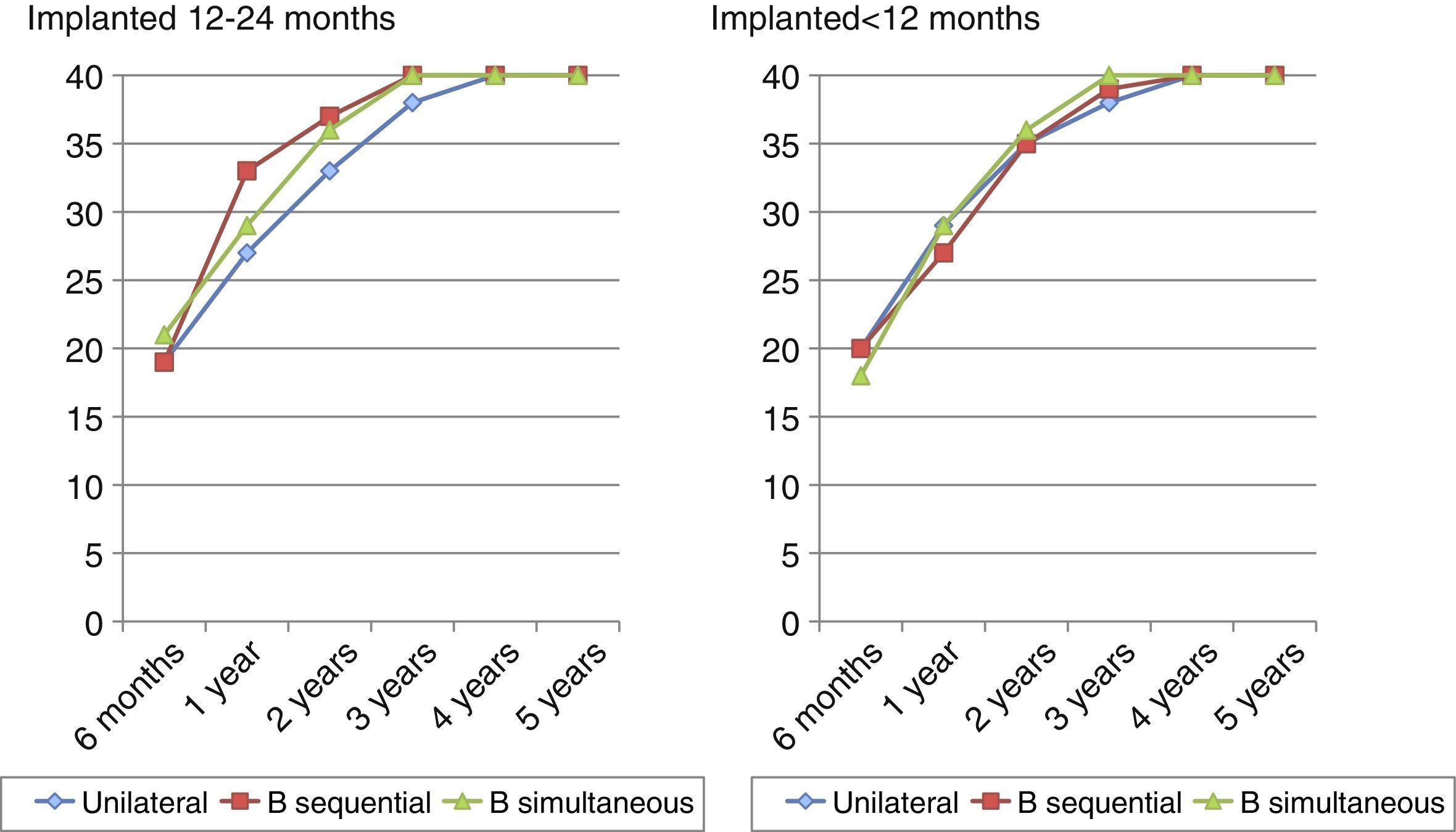
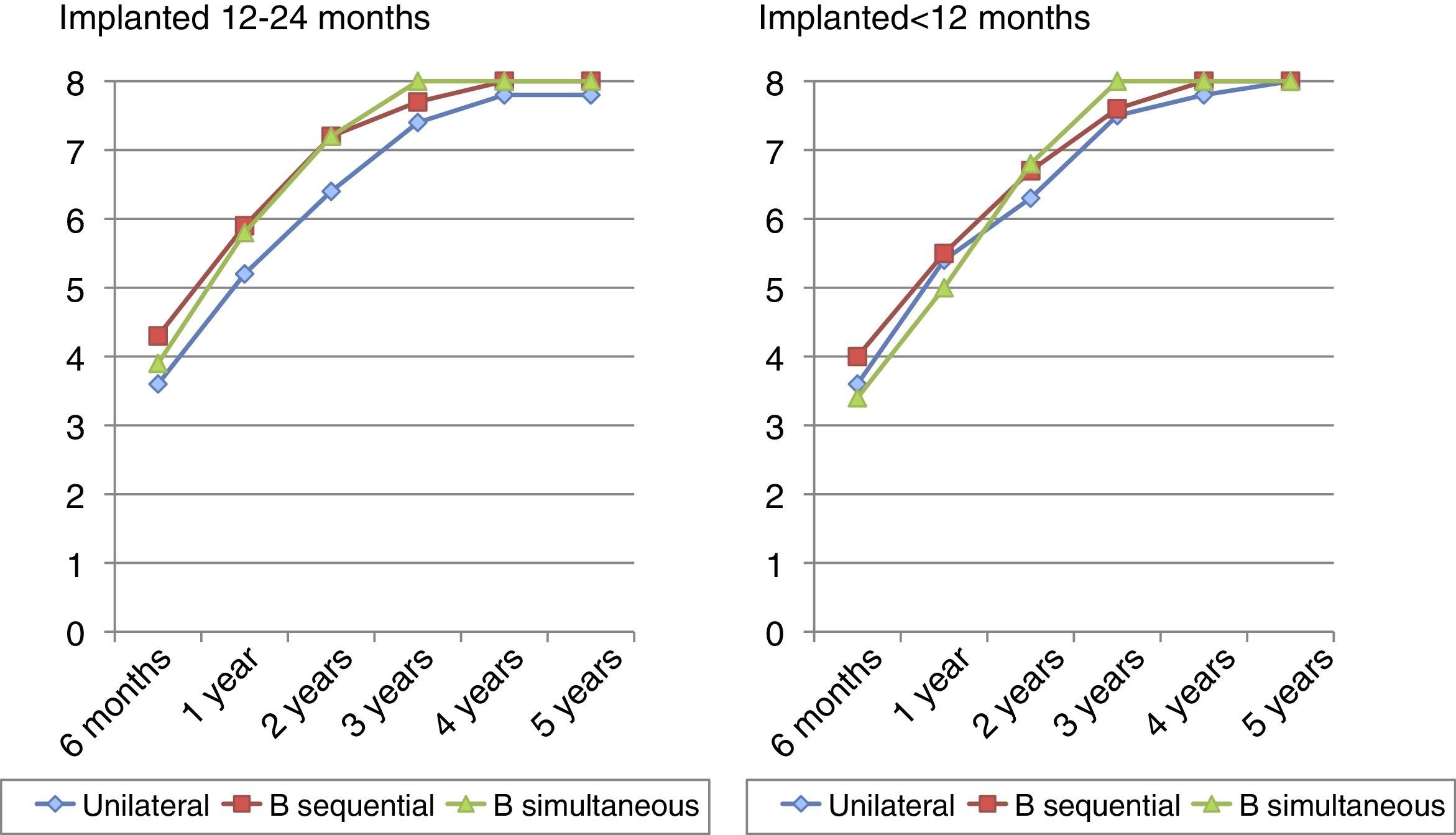
In Fig. 3 the results obtained were compared with the IT-Mais scale in patients under one year of age compared with those who had implantations between 12 and 24 months, with a similar behaviour being appreciated in them, and maximum scores from 3 years post-implantation. If we compare the outcome for patients with unilateral implants to those with bilateral implants, we may observe that there are no marked differences in annual scores, despite the fact that the bilateral implant patients, both sequential and simultaneous, obtained 40 points 3 years post-implant, whilst the unilateral patients obtained this 4 years post-implant. However, these differences were not statistically significant.

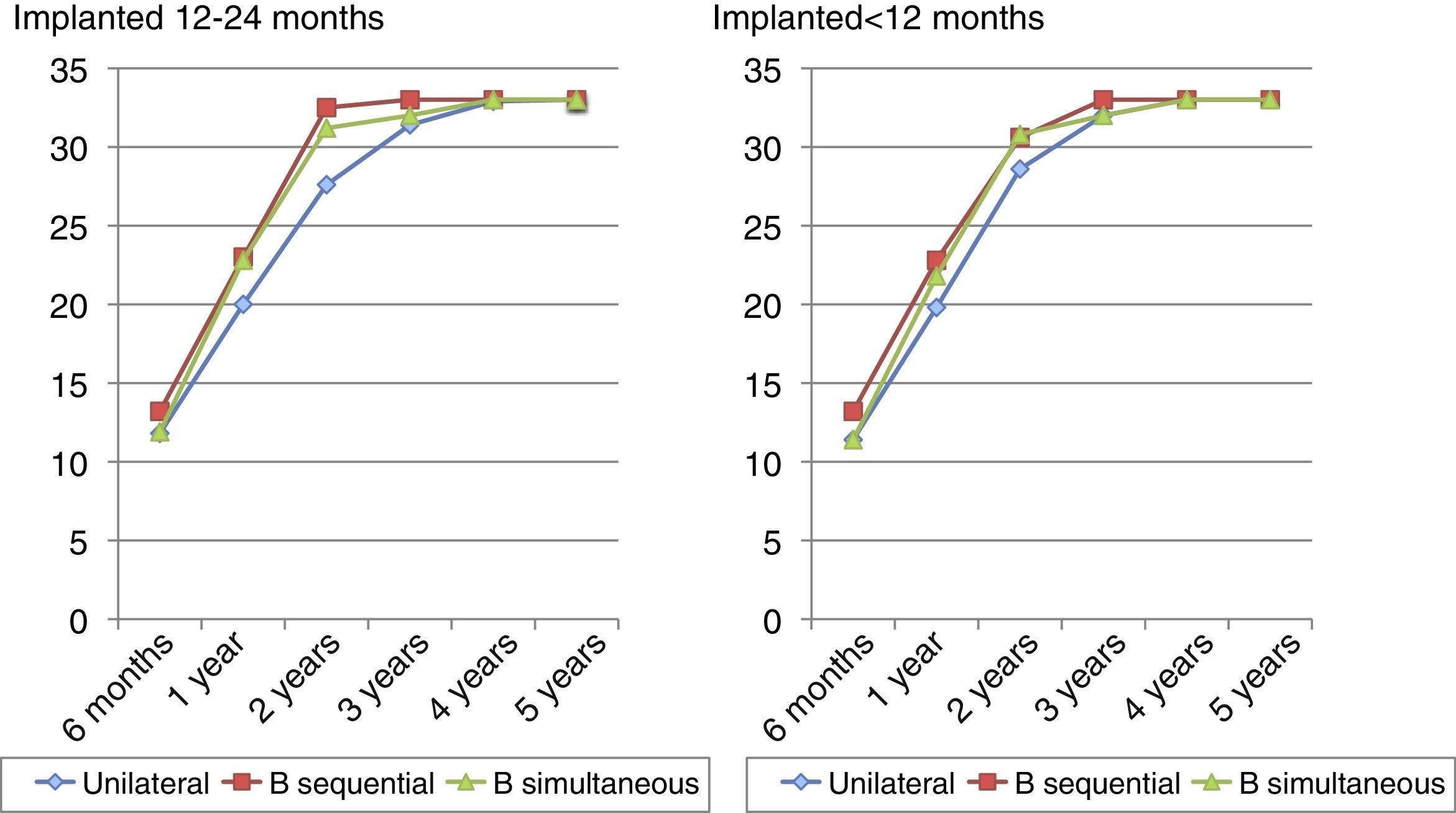
Fig. 4 shows the results for the Nottingham auditory performance scale and here we observe how the great majority of children in both groups achieve category 8 between 3 and 5 years post-implant. Statistical comparison of the outcome achieved by the 2 age groups in the test reveals statistically significant levels above those established for this study (P>.05), and there are therefore no statistically significant differences in this aspect between both groups following implantation. If we compare the results of this questionnaire in children with a single implant to those with 2, maximum scores for bilateral implants at 3 years after implantation are detected, whilst those children with only one implant obtain this result 5 years after surgery. The group of children who were given implants between 12 and 24 months did not obtain the maximum score even 5 years after implantation. However, statistical comparisons do not provide us with significance levels under 0.05.

In the LittlEars test, children with normal hearing have to obtain the maximum score at 2 years of age. Fig. 5 shows us how the children with cochlear implants obtain these maximum audio-communicative skills after using the implant for 3 years, which is when they obtain the same scores as children with normal hearing. We may therefore state that children with implantations have a one-year delay in language development. In this test there is a slight difference between the 2 age groups studied, with better scores obtained in the group of children with implantations before they are 12 months old than those who received the implantation between 12 and 24 months of age. Differences are not, however, statistically significant (P>.05). Practically identical results are obtained by those children with a single implant compared with those who have bilateral implants, made evident from the absence of statistically significant differences.

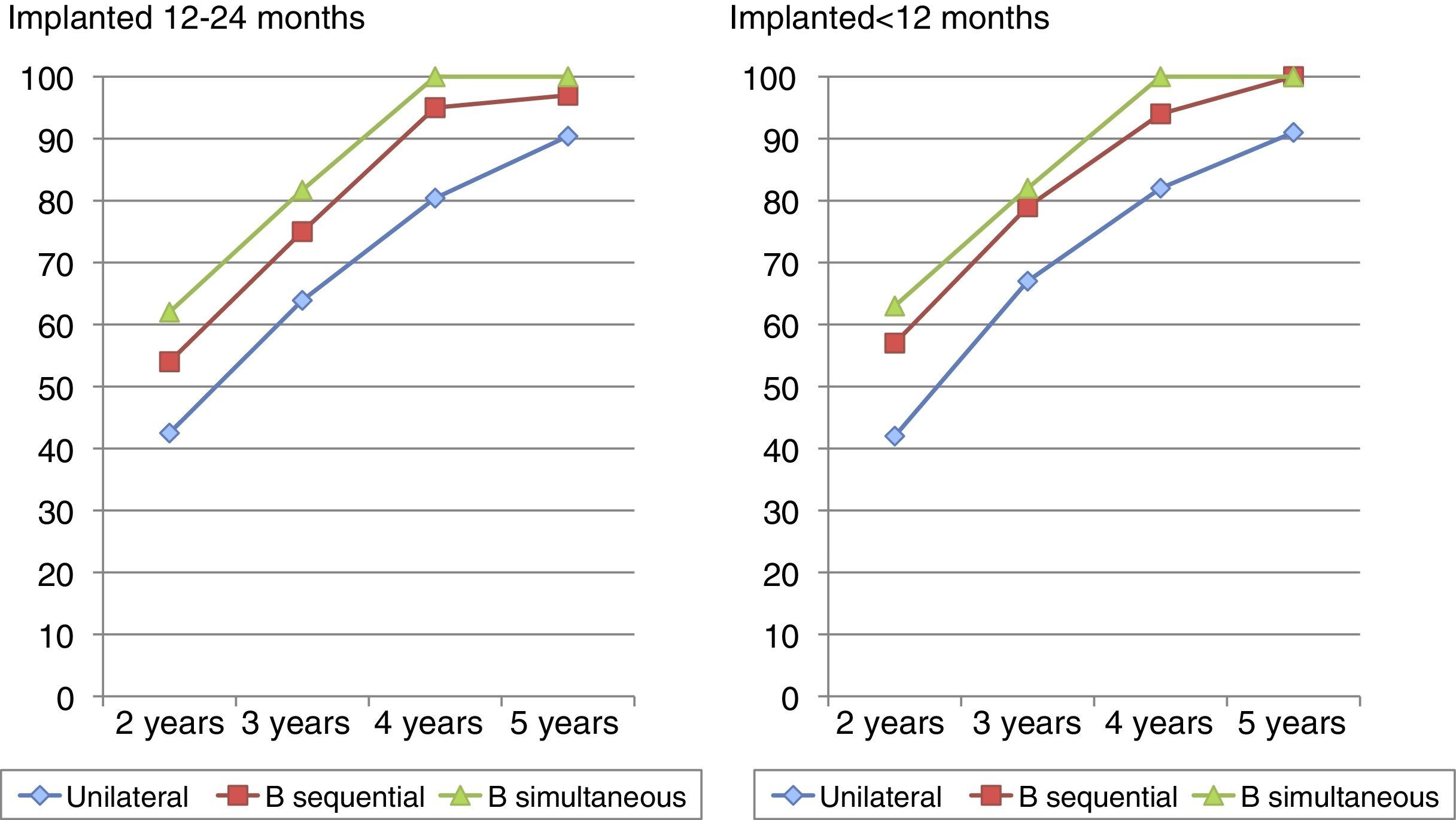
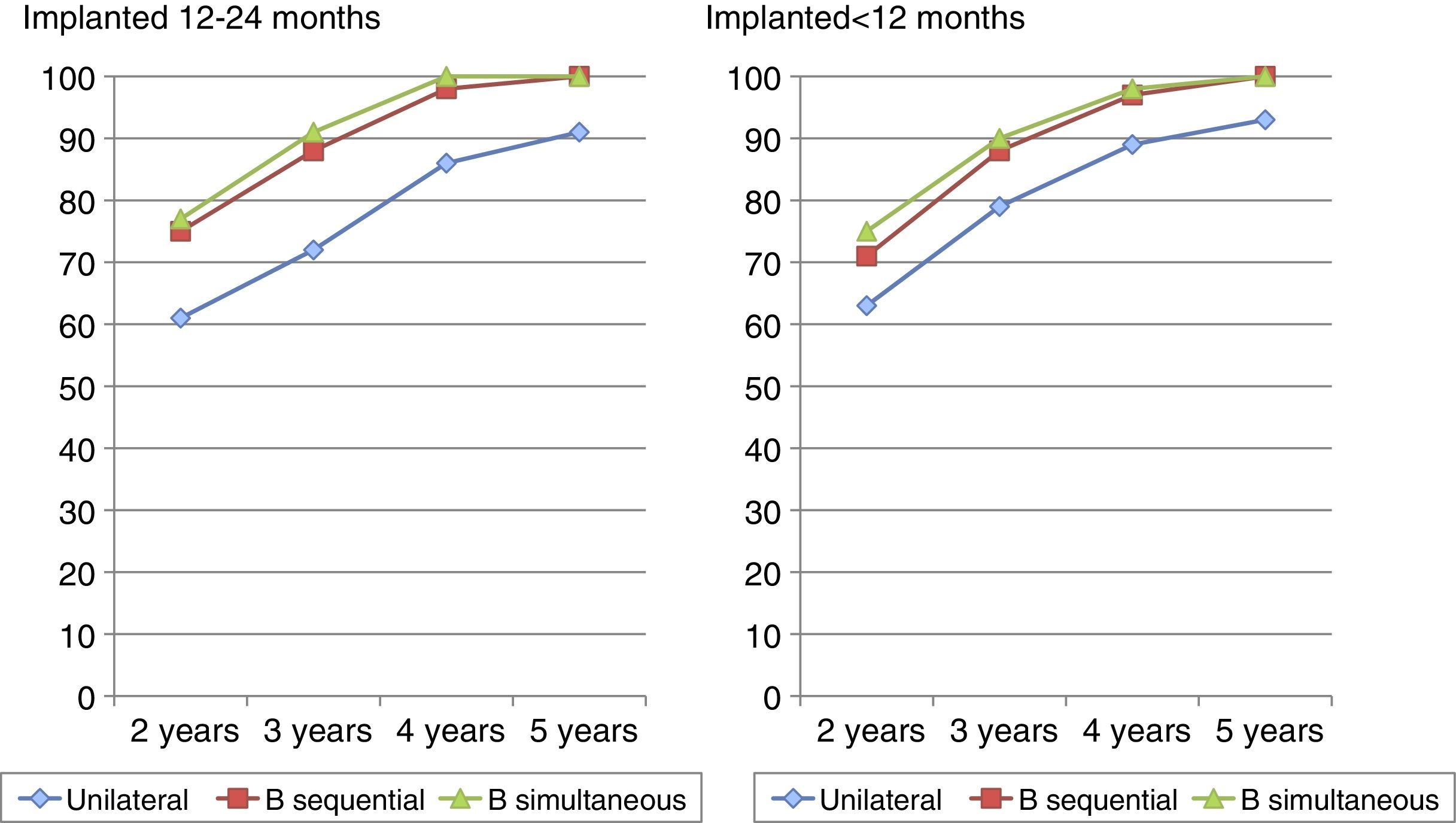
Speech tests study the child's ability to discriminate, identify, recognise and understand the spoken word. Fig. 6 shows the results of the two syllable test over time, with notable gains after 3 years of implantation, and minimal differences between the 2 age groups studied, the outcome being somewhat better for those children who had implants during their first year. A similar situation is observed for the sentences test (Fig. 7) where a gradual gain over time is appreciated after 3 years of implantation and this gain becomes slightly better when the children receives the implant during their first 12 months. In both speech tests, the comparison with the Student's t-test confirms that there are no statistically significant differences between the groups (P>.05). However, the two syllable tests and sentences test clearly show that the children with bilateral cochlear implants, whether simultaneous or sequential, are able to 100% recognise two syllables and phrases earlier, whilst the children with a unilateral implantation do not obtain similar results until five years after surgery. Spontaneous learning of language detected in children with implantations before they are one is also important. In this case, when comparing statistics between unilateral and bilateral implants, differences are statistically significant between the 2 groups (P<.05).


Finally, if we compare the results in all questionnaires and tests on speech between children who received bilateral implants when they were under 1 year of age and those who received them between 12 and 24 months no statistically significant differences are detected in any case, with similar scores being obtained throughout the annual tests and maximum scores obtained 3 years after implantation in both groups.
Similarly, if we compare hearing threshold results, and those in the IT-Mais, Nottingham, LittlEars and verbal tests between children who underwent bilateral implantation simultaneously and those who had sequential implantations, regardless of the age of implantation, there are no statistically significant differences, regardless of the fact that in almost all tests, and particularly in the two syllable tests, the results of simultaneous bilateral implantation appear to be more favourable (Figs. 2–7).
DiscussionThe aim of this study is to demonstrate both the importance of early cochlear implantation, even before one year of age, in children with severe and profound pre-lingual bilateral sensorineural hearing impairment and also to discover whether there are auditory differences and in the communication skills of these children depending on whether they have received a single implant or 2 implants.
Study design excluded biases which could distort outcome. In fact, all the children were assessed pre and post implantation by the same team and were operated on by the same surgeon. The device programming mechanism was the same in all cases, despite the fact that these devices were produced by different manufacturers (AB®, Cochlear® and Medel®). Our minimum implantation age was 9 months. Surgery was not performed earlier, even though diagnosis may even have been made from 3 months onwards, since to access a reliable diagnosis in such small children several months of tests are required.10 The average age of implantation was 11.9 months in those with implantations in the first year and 18 months in the second group. Fryauf-Bertschy et al.11 analysed 34 children with prelingual hearing impairment with cochlear implants, concluding that auditory performance is inversely related to implantation age. Other studies have demonstrated that children with hearing impairment develop a lapse in language development, compared with normal hearing children and that once auditory stimulus is implanted in early stages, they begin to develop language with almost normal speed.12,13
We were also able to verify this fact, as the children with early implantations, the total of our sample, obtain the maximum scores of the tests executed during the first 2–3 years after cochlear implantation. This indicates that children with congenital hearing impairments may develop language skills at an almost normal rhythm, provided that the implantations are performed early enough in life. So, Svirsky et al.12 compared the language skills of normal hearing children with those affected by prelingual impairment who received implantations at 2, 3, and 4 years of life. In this study we observe the differences maintained between implantation at ages below 4, and find the best results when implantations are carried out below the age of 2. In our case we found no statistically significant differences in the 2 age groups, perhaps because both included implantations carried out at below the age of 2. Although it is true that in speech tests, the best results were obtained by children who had implantations during their first year, no statistically significant differences were noted. We can still maintain, however, that when surgery is performed within the first 12 months of life, with no major surgical risks attached, spontaneous learning of language is appreciated.14
Notwithstanding, there was no observance in the analysis of audiometric threshold averages of deterioration in language performance being connected with the age of implantation, which has been argued by different authors.15,16 This does, however, suggest that although activation of the peripheral auditory pathway may be efficiently achieved at different ages of implantation, acquisition and development of language achieves its best scores when activation of the pathway is made at early ages. This is because the acquisition of language requires a flexible brain, able to make new connections and relationships to acquire complex skills such as talking and not merely peripheral input.16
Regarding bilateral compared with unilateral implantation, the recent article by Asp et al.17 confirms that the main advantage of bilateral cochlear implants is detected in better speech recognition in a noisy environment and a better localisation of sound, but there are no significant differences to children with a single implant with regards to specific hearing improvement. Other studies confirm these benefits in sound localisation,18–20 in the avoidance of head shadow effect21,22 and word perception in noise,22,23 with bilateral implantation and also to reach bilateral stimulation of pathways and auditory centres during the period of greatest neuroplasticty.24 Our study findings reveal maximum scores on the IT-Mais, Nottingham and LitllEars scales which are similar in both groups; however, in the two syllable and sentence tests we clearly see how children with bilateral implantation, either simultaneous or sequential, achieve scores of 100% earlier two syllable and sentence recognition. The differences are statistically significant and when the benefits of implantation are confirmed, therefore, the benefits of bilateral implantation compared with unilateral implantation in better recognition of the spoken work and therefore in better acquisition of the necessary socio linguistic skills for full development.
Finally, when comparing the results in all the completed questionnaires no statistically significant differences are found between children subjected to bilateral implants aged under 1 year and those who were given implants aged between 12 and 24 months. Throughout the annual tests scores are similar and maximum scores are obtained 3 years after implantation. This suggests that bilateral implantation is more important than the age at which the implant is received, provided it is done before the child is 2. However, there are no statistically significant differences between whether the implantation is simultaneous or sequential.
ConclusionsTo conclude, we may say that children under 2 with congenital hearing impairments subjected to cochlear implantation develop language in a similar manner to those with normal hearing. Moreover, if the operation takes place before they are one, excellent results in speech tests are achieved, and some spontaneous language learning is appreciated. The child thus acquires functional communication skills with their environment, which are maximum between 2 and 3 years after cochlear implant activation.
Bilateral cochlear implantation is more important than early implantation. We have proven that a better outcome is achieved than with unilateral implantation, above all in the effects of language discrimination, which is highly important at these ages. There are, however, no differences between whether bilateral implantation is simultaneous or sequential, and we have no arguments in favour of one or the other.
We reiterate that the aim of this paper is not just to ensure good early hearing screening in children with severe and profound sensorineural hearing impairments so that they may be given a cochlear implantation, but also to insist that this procedure be carried out whenever possible in the first year of the child's life and in particular, bilaterally. In this way, these children will be able to develop totally equal auditory and linguistic skills to children with normal hearing abilities.
Conflict of InterestsThe authors have no conflict of interest to declare.
Please cite this article as: Escorihuela García V, Pitarch Ribas MI, Llópez Carratalá I, Latorre Monteagudo E, Morant Ventura A, Marco Algarra J. Estudio comparativo entre implantación coclear uni y bilateral en niños de 1 y 2 años de edad. Acta Otorrinolaringol Esp. 2016;67:148–155.