
Pancreatic pseudocyst is a complication of acute pancreatitis and it usually manifests with abdominal pain. We report the case of a 45-year-old man with a history of acute pancreatitis who presented with abdominal pain, dyspareunia, and a palpable inguinal mass. Computed tomography scan revealed a large loculated pseudocyst that dissected through the pelvic cavity towards the inguinal canal, compressing pelvic and inguinal structures. When a patient with a history of pancreatitis develops an inguinal mass, a dissecting pancreatic pseudocyst should be suspected.
El pseudoquiste pancreático es una complicación de la pancreatitis aguda, que usualmente se presenta con dolor abdominal. Reportamos el caso de un hombre de 45 años de edad con historia de pancreatitis aguda, que se presentó con dolor abdominal, dispareunia y una masa inguinal palpable. La tomografía computada mostró un gran pseudoquiste loculado, que disecó a través de la cavidad pélvica hacia el canal inguinal, comprimiendo estructuras pélvicas e inguinales. En pacientes con historia de pancreatitis, el desarrollo de una masa inguinal debe crear sospecha de un pseudoquiste pancreático disecante.
Pancreatic pseudocyst is a collection of pancreatic exocrine secretions in or around the pancreas, usually as a result of acute pancreatitis.1,2 Other etiologies include chronic pancreatitis, pancreatic duct obstruction, trauma, or malignancy.3 It usually forms at the lesser peritoneal sac, surrounding the pancreas, but unusual locations and sizes have been described. We present the case of a patient with a large pancreatic pseudocyst that dissected down to the inguinal area, manifesting as abdominal discomfort and dyspareunia.
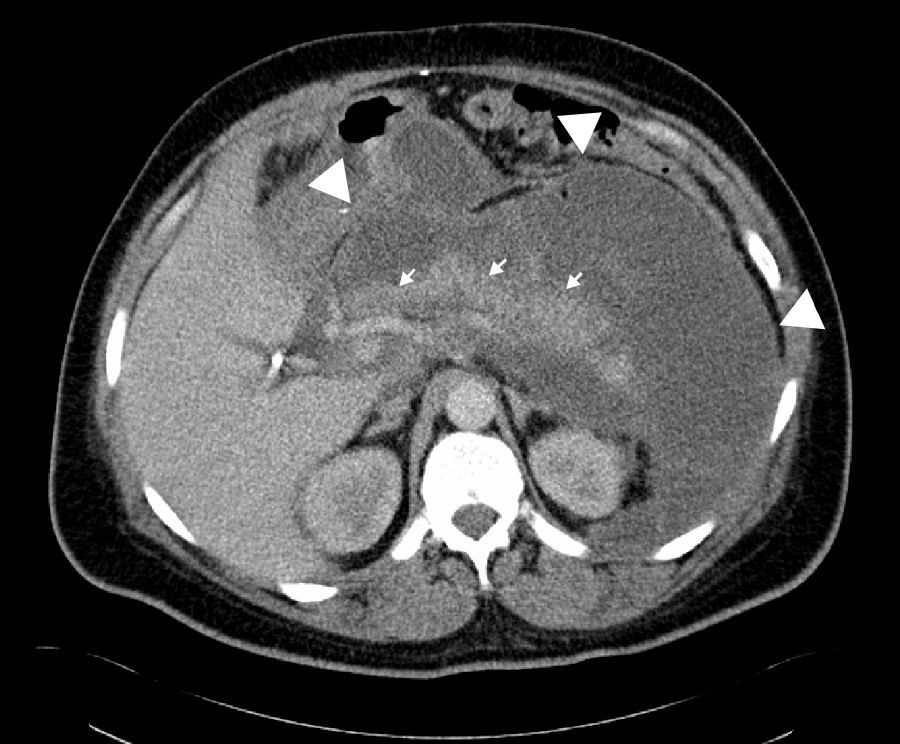
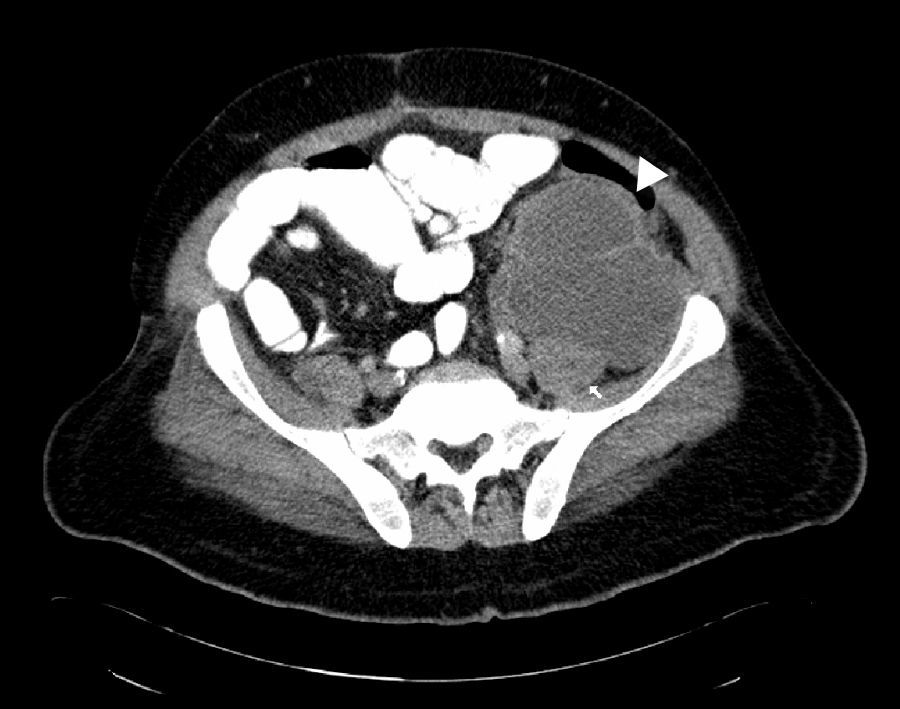
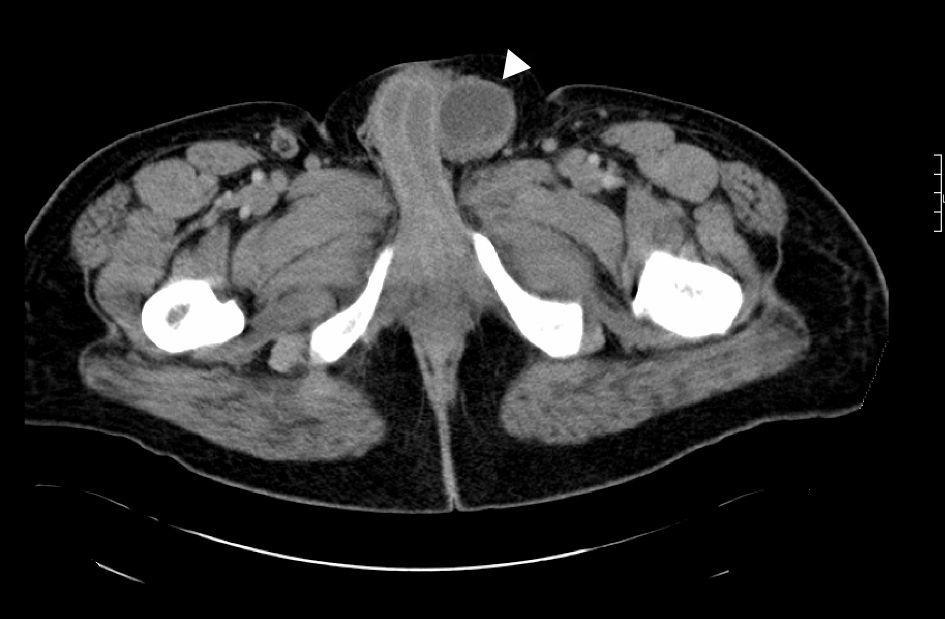
Case reportThis is a 45-year-old African American male presenting with a 2-week history of abdominal pain, anorexia, and pain during intercourse. His history was significant for an episode of severe alcohol related pancreatitis two months prior complicated with multiorgan failure and a prolonged hospitalization. There was no mention of dysuria, urethral discharge, testicular pain, history of pelvic surgery or prior similar complains in the past. Physical exam was significant for normal vital signs, and diffusely tender distended abdomen without organomegaly. A 2 x 4cm tender non-reducible mass was palpated in the left inguinal region. Pertinent laboratory results included mild leukocytosis, normal pancreatic enzymes and normal transaminases. Urine analysis was unremarkable. Abdominal CT with contrast revealed a large septated fluid collection of approximately 30cm in diameter, extending from the lesser sac to the left side of the pelvis into the left inguinal canal and scrotum. The collection was compressing against the stomach, duodenum, spleen, but there was no radiological signs of obstruction (Fig. 1). It dissected following the path of the left psoas muscle down to the pelvis (Fig. 2). At the level of the inguinal canal, it compressed against perineal structures including the base of the penis (Fig. 3). Communication of the retroperitoneal and inguinal collection was determined by visualization of the continuum through the different tomographic cuts. At all levels the collection presented with Hounsfield units ranging from five to 15, corresponding to the attenuation coefficient of cystic fluid. Percutaneous drainage was precluded due to the multiloculated nature of the pseudocyst. Considering persistence of abdominal pain and inability to advance diet, the patient underwent laparoscopic surgical drainage, and 3.5 liters of non-purulent fluid was retrieved. Seven days after the surgery, the patient presented with tachycardia, fevers, worsening abdominal pain and increased output from surgical drains. Cultures confirmed peritonitis with Pseudomona aeruginosa and methicillin resistant Staphylococcus aureus. The patient required a total of five laparotomies for debridement and retroperitoneal washout, as well as prolonged antibiotic therapy. Late complications included wound infection and incisional hernia that were later repaired. Follow up CT of the abdomen revealed a 5cm cystic lesion in the tail of the pancreas with no evidence of pelvic collections. At that time there was no further complains of dyspareunia.
 surrounding the pancreas and compressing hollow viscus. Small arrows show the location of the pancreas.")
 dissecting through the left psoas muscle pathway. Small arrow indicated the left psoas muscle.")
, and compressing the base of the penis.")
Pancreatic pseudocyst is a common complication of acute and chronic pancreatitis. It is defined as a pancreatic fluid collection in the abdominal cavity surrounded by a fibrous non-epithelized capsule. This is an important feature in differentiating pseudocysts from cysts or cystic neoplasms of the pancreas. A significant number of pancreatic pseudocysts are asymptomatic and are located at the peritoneal lesser sac. The most common symptom is abdominal pain and if hollow viscus is compressed, nausea, vomiting, or early satiety may ensue. Treatment is conservative unless there are signs of infection or intractable symptoms, in which case radiological or surgical drainage is recommended.1–4 Dyspareunia, or pain during sexual intercourse, is a rare presentation in males and has been associated with conditions like chronic prostatitis, chronic pain syndrome, history of inguinal hernia repair, isolated painful ejaculation syndrome or pudendal nerve entrapment.5 In our patient, there was a chronological association between the abdominal pain and the dyspareunia, and there was no mention of other genitourinary symptoms. In his case, the dyspareunia could be associated to compression of the dorsal nerve of the penis, a branch of the pudendal nerve, which has sensory and somatic innervation.
Five other reports have described migration of pancreatic pseudocysts down through the retroperitoneum, following the psoas muscle pathway, and creating an inguinal mass.6–10 The psoas muscle passes beneath the inguinal ligament, which constitutes part of the inferior wall of the inguinal canal. We can assume that due to the anatomical vicinity, the inflammatory process can involve the inguinal canal creating a collection. None of the previous cases reported painful intercourse as part of the presentation. In three of these reports the communication between the retroperitoneal and inguinal compartments was established by fistulogram (with or without fluid amylase levels), in 1 with tomographic visualization, and one case only describe inguinal mass as part of the clinical presentation. In our case, the dissection path was confirmed by direct tomographic visualization.
In conclusion, pancreatic pseudocyst can extend from the retroperitoneum to distal locations including the inguinal canal, causing anatomical related symptoms. In patients with history of pancreatitis, the presence of an inguinal mass should arouse suspicion of a pseudocyst of the pancreas.
FundingThe authors of this manuscript we have not received funding.
Conflict of interestThe authors have no conflicts of interest to declare.

