








Clinical practice guidelines (CPG) are a set of recommendations for professionals, patients, and families, in order to make decisions about health care. The CPG respond to the need for concise, accurate, practical, and up to date information. In the field of mental health, Colombia has developed three GPC; alcohol (GPC-OH), depression (GPC-TDA), and schizophrenia.
ObjectivesTo describe the Web Portal traffic related to psychiatry guidelines, with emphasis on the number of visits, distribution throughout Colombian cities, and estimating user behaviour patterns.
MethodsAn evaluation was made of the traffic at the Clinical Practice Guidelines Web Portal of the Ministry of Health and Social Protection between 2013 and 2015 (two years of observation since the inauguration of the Portal).
ResultsOut of the 45 GPC published on the website, the CPG-OH represented 1.21% of all page views of the Portal. CPG-TDA reached 1.52% (accumulated percentage of 2.73%), being the eighth most consulted guideline, with CPG-OH being number 16. The highest mean monthly number of visits for this group of guideliness was for the CPG-OH for health professionals (353 visits/month), and the lowest was for the CPG-AD for patients and relatives (24 single visits/month). Bogotá D.C. was the city where health carers accessed the guidelines more often. The guidelines for patients and relatives were consulted more in Villavicencio, Cúcuta, Manizales, Pereira, and Pasto.
ConclusionsThe web portal partially fulfils the purpose of circulating the CPG in Colombia. The visits to the CPG of mental health is quite low, and requires better dissemination strategies that allow the use of information and communication technology.
Las guías de práctica clínica (GPC) son un conjunto de recomendaciones para que profesionales, pacientes y familiares tomen decisiones sobre la atención en salud. Las GPC responden a la necesidad de información concisa, veraz, práctica y actualizada. En Colombia, en relación con la salud mental se han desarrollado las GPC de alcohol (GPC-OH) y depresión (GPC-TDA).
ObjetivosDescribir el tráfico del portal web de GPC relacionado con las guías de psiquiatría, poniendo el énfasis en el número de consultas, la distribución por ciudades colombianas y la estimación de patrones de comportamiento de los usuarios.
MétodosSe evaluó el tráfico en el portal web de GPC del Ministerio de Salud y Protección Social entre 2013 y 2015 (2 años de observación desde el lanzamiento del portal).
ResultadosDe las 45 GPC publicadas en el portal, la GPC-OH acaparó el 1,21% de todas las páginas del portal vistas. La GPC-TDA alcanzó el 1,52% (ambas guías acumuladas, el 2,73%), la novena guía más consultada del portal y la GPC-OH, la décimo sexta. Tuvo la media mensual de visitas más alta en este grupo de guías la GPC-OH de profesionales de la salud (353 visitas/mes) y la más baja, la GPC-TDA de pacientes y familiares (24 visitas únicas/mes). Bogotá D.C. es la ciudad desde donde los servidores de salud accedieron con mayor frecuencia a las guías. Las de familiares fueron más consultadas en Villavicencio, Cúcuta, Manizales, Pasto y Pereira.
Conclusionesel portal cumple parcialmente el propósito de difundir las GPC en Colombia. La difusión de las GPC de salud mental es bastante baja y requiere la elaboración de estrategias de difusión que permitan un mayor uso de tecnologías de la comunicación y la información.
The exponential increase in the volume of scientific literature and the greater demands made on their time in clinical practice are obstacles that prevent healthcare professionals from keeping abreast of new developments in their areas of expertise. For this reason, healthcare professionals need to update their knowledge base using reliable and practical guidelines that summarise large volumes of information and synthesise the best evidence available to scientifically support their clinical decisions.1
Clinical practice guidelines (CPGs) drawn up in Colombia by various universities and scientific societies, together with the Ministry of Health and Social Protection and the Colombian Administrative Department of Science, Technology and Innovation (COLCIENCIAS), are systematically developed as a set of recommendations to help professionals, patients and relatives make decisions about the most appropriate healthcare for a specific clinical condition. CPGs respond to the need for concise, reliable, accurate, practical and up-to-date information, and their use enables health services to achieve a greater level of standardisation and efficiency. CPGs are also designed to resolve any doubts doctors might have about the different therapies available and the evidence to support their use.2
Despite their importance, several challenges must be overcome before the implementation, use and adherence to CPGs can have an impact on patient care. Estimates suggest that only one third of CPGs are commonly used.3,4 This is in part because the process of building CPGs is detached from the mechanisms designed to implement them, which in turn do not take into account the specific barriers encountered in health services where the CPG is supposed to be applied systematically.5 This raises the need for alternative CPG dissemination and implementation strategies that go beyond the printed page and take advantage of the power of digital technologies,6 which are integrated into electronic medical records,7 and which become a cornerstone of routine patient management.8 This prompted the development of the CPG web portal, defined as a CPG communication and dissemination model that allows their content to be efficiently summarised and presented online.9
The CPGs included in the first version of the portal were developed by several Colombian research groups that developed these recommendations following the methodology contained in the Methodology for the Development of Comprehensive Healthcare Guidelines10 as part of the 500 and 513 COLCIENCIAS call for proposals for the creation of a projects’ bank for the development of evidence-based comprehensive care guidelines (CCG).11,12 The team in charge of building the portal, made up of members of the Department of Epidemiology and Biostatistics of the Faculty of Medicine of the Pontificia Universidad Javeriana, adapted the set of CPGs thus developed to the requirements of the portal. The team included specialists, clinical epidemiologists, general practitioners, rural physicians, other healthcare professionals and specialised computer science engineers. The project was carried out in two stages: the first, the design of the portal, culminated in the launch of the website on 23 July 2015. The second phase, maintenance and development, was undertaken by the original team until March 2014, after which the portal and its administration were taken over by the Ministry of Health. The use of the portal to disseminate CPGs was included in the Guideline Implementation Manual, published jointly by the Ministry of Health and the Instituto de Evaluación de Tecnologías en Salud (Institute for Health Technology Assessment [IETS]),13 and has been promoted by the Ministry since the launch of the CPGs.14
The CPGs developed at this stage include the “Clinical Practice Guideline for the early detection, diagnosis and treatment of the acute phase of intoxication in patients with alcohol abuse or dependence” and the “Comprehensive care guideline for the early detection and diagnosis of depressive episodes and recurrent depressive disorder in adults”. Various versions of the “CPG Comprehensive care of adults with a diagnosis of depressive episodes or recurrent depressive disorder”,13,14 which respond to the need to provide Colombian doctors with evidence-based guidelines to treat medical conditions prioritised by the Ministry of Health, are presented on the portal. These two CPGs, it should be noted, address the most prevalent mental health problems in Colombia.
Online dissemination of guidelines for the management of high-impact psychiatric conditions is a new approach to CPG implementation that harnesses the power of information and communication technologies to disseminate evidence-based medicine, and it is therefore important to measure traffic on the portal and describe user access patterns to the alcohol (CPG-OH) and the depressive disorder (CPG-ADD) CPGs.
These patterns will highlight any deficiencies in the communication strategy and indirectly measure the impact that CPGs can have in clinical practice by analysing online user access patterns. They will also enable portal managers to detect the need for updates, new dissemination strategies, and the need to optimise the online resource. In addition, implementation of the CPGs and their dissemination via the Portal must be analysed using specific information access metrics that, in turn, identify the way in which visitors use the Portal, and will eventually determine the efficacy of this tool.
The aim of this study has been to describe CPG-OH- and CPG-ADD-related CPG portal traffic, particularly the distribution of CPG access according to cities in Colombia, and to estimate user access patterns using standard website analysis metrics.
MethodsUser traffic in the CPG-OH and CPG-ADD guidelines in the CPG portal was obtained from http://gpc.minsalud.gov.co in the period between 23 July 2013 and 23 July 2015 (2 years following the launch of the portal) using Google Analytics. The data was exported to a Google Sheets spreadsheet and statistical analysis was performed on Excel 2013, Stata 13 and Xlstat V.2015.
The variables analysed were: a) page views: total number of pages viewed; repeat views of the same page are also counted (pages refer to the pages hosting the CPG-OH and CPG-ADD); b) unique page views: number of sessions during which the specified page has been viewed at least once; a unique page view is counted for each uniform resource locator (URL)+page title combination; c) unique visitor: session by a user who accesses the guidelines only once; d) return visitor: session by a user who returns to the guidelines; e) average session: session length, from time of access to the time of exit from the guideline viewed, and f) bounce rate: percentage of unique page views (or web sessions), in other words, the number of page views in which a person leaves the website from the landing page without browsing any further.
Each of these variables was studied relative to the access pattern of each version of the CPG-OH and CPG-ADD guidelines for healthcare professionals and for patients and relatives. Traffic-related variables were described as relative frequencies and averages, in addition to the CPG access patterns in the main Colombian cities. Averages were compared using one-way ANOVA. If the ANOVA assumptions were not met, the Kruskal–Wallis test was used. Proportions were compared using the χ2 test and the Marascuilo procedure for comparing multiple proportions.6 Statistical significance was established as p<0.05.
ResultsThe portal presents three versions of the CPGs: full version in PDF format, summary version for healthcare professionals (HTML version and PDF format), and a version for patients and carers (HTML version and PDF format). The CPGs for healthcare professionals are identified by the image of a doctor, while CPGs for patients and relatives carry the image of a patient-doctor consultation. The first content section of the online version of each guideline contains evidence-based recommendations, giving easy access to the clinical questions and their respective recommendation.
The online versions of the CPG-OH and CPG-ADD can be accessed by specialty, by developer and alphabetically. All recommendations in all guidelines include the clinical question, the degree of evidence and the strength of the recommendation. The other sections of the online version maintain the outline of the original document (e.g. introduction, methodology, references, etc.). The CPGs include flow charts, tables and figures that summarise the evidence-based recommendations. In the online version of the CPG, this additional information was accessed via a tab in which the images are arranged into sections with graphic content that can be downloaded in slideshow format (.ppt and .pptx).
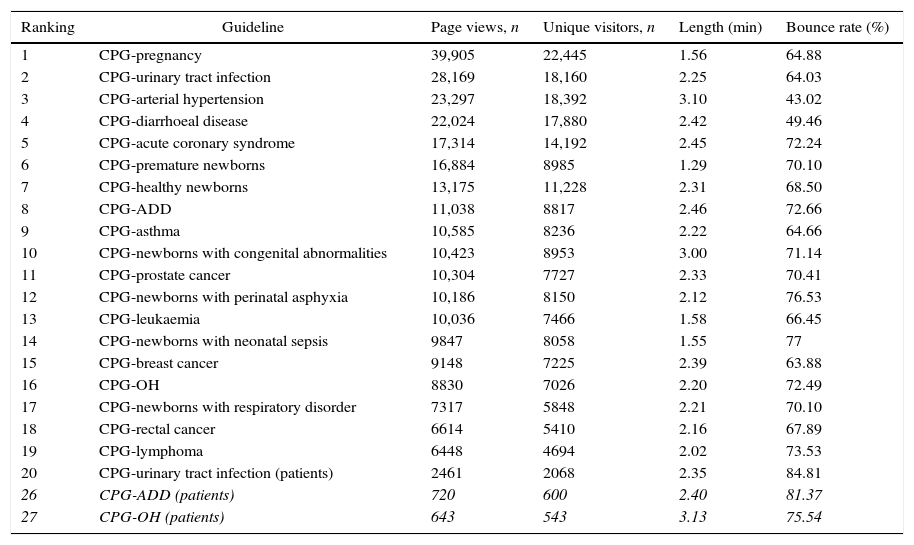
During the two study years, CPG-OH for healthcare professionals accounted for 1.21% of all portal page views, while CPG-ADD reached 1.52% (the sum of both these CPGs is 2.73%), making the CPG-ADD the ninth most consulted guideline of the portal, and the CPG-OH the sixteenth, while the CPG-ADD and CPG-OH for patients and relatives ranked 26 and 27, respectively (45 CPGs in total are published on the portal; the schizophrenia CPG was not included in this analysis as it was only included in the portal in October 2014).
In this group of guidelines, the CPG-OH for healthcare professionals received the highest average number of page views per month (353 page views/month), with the CPG-ADD for patients and relatives (24 unique visitors/month) ranking lowest in the average number of page views per month (p<0.1). The number and pattern of page views per month according to the type of guideline are shown in Fig. 1.
 during the study period. In the case of CPG-OH (for healthcare professionals), two access peaks are observed in August 2013 and March 2015. Access to the CPG-ADD peaks in the same months. The sudden decrease in page views in month 8 (February 2014) is due to a suspension of the portal for server maintenance. CPG-OH: clinical practice guidelines on alcohol abuse; CPG-ADD: clinical practice guidelines on depressive disorder.")
Comparison of the number of CPG page views according to the type of guideline and view (page views and unique visitors) during the study period. In the case of CPG-OH (for healthcare professionals), two access peaks are observed in August 2013 and March 2015. Access to the CPG-ADD peaks in the same months. The sudden decrease in page views in month 8 (February 2014) is due to a suspension of the portal for server maintenance. CPG-OH: clinical practice guidelines on alcohol abuse; CPG-ADD: clinical practice guidelines on depressive disorder.
The average session was 0.02.54; the CPG with the shortest session was the CPG-OH for healthcare professionals (return views) (0.02.19) and that with the highest was the CPG-OH for patients and relatives (return views) (0.03.51). The average session did not differ significantly between the different guidelines or type of users (p=0.74) (Fig. 2).
. CPG-OH: clinical practice guidelines on alcohol abuse; CPG-ADD: clinical practice guidelines on depressive disorder.")
Average session on each CPG by healthcare professionals and patients and relatives. In the case of CPG-OH, there is greater variability in the average session on CPG for patients and relatives while there is greater homogeneity in the case of CPG-ADD; however, a significant difference was observed between the average session and the type of CPG (p=0.74). CPG-OH: clinical practice guidelines on alcohol abuse; CPG-ADD: clinical practice guidelines on depressive disorder.
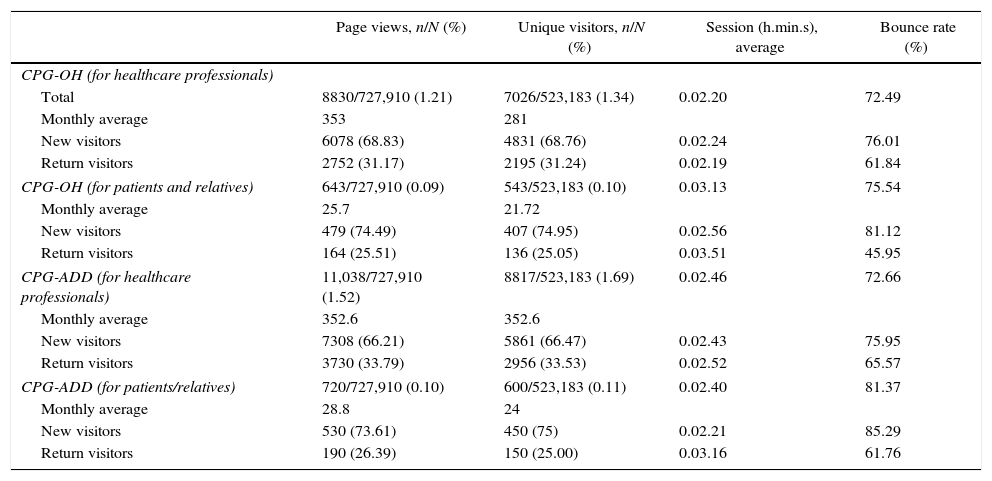
The average bounce rate was 75.15%; the CPG-ADD for patients and relatives obtained the highest percentage (85.29%), while the CPG-OH for patients and relatives obtained the lowest (45.95%) (p=0.8) (Fig. 3). Tables 1 and 2 show the usage patterns according to type of guideline and type of user.
.")
Usage patterns for CPG-OH and CPG-ADD. Total page views on the portal: 727,910. Total unique visitors on the portal: 523,183.
| Page views, n/N (%) | Unique visitors, n/N (%) | Session (h.min.s), average | Bounce rate (%) | |
|---|---|---|---|---|
| CPG-OH (for healthcare professionals) | ||||
| Total | 8830/727,910 (1.21) | 7026/523,183 (1.34) | 0.02.20 | 72.49 |
| Monthly average | 353 | 281 | ||
| New visitors | 6078 (68.83) | 4831 (68.76) | 0.02.24 | 76.01 |
| Return visitors | 2752 (31.17) | 2195 (31.24) | 0.02.19 | 61.84 |
| CPG-OH (for patients and relatives) | 643/727,910 (0.09) | 543/523,183 (0.10) | 0.03.13 | 75.54 |
| Monthly average | 25.7 | 21.72 | ||
| New visitors | 479 (74.49) | 407 (74.95) | 0.02.56 | 81.12 |
| Return visitors | 164 (25.51) | 136 (25.05) | 0.03.51 | 45.95 |
| CPG-ADD (for healthcare professionals) | 11,038/727,910 (1.52) | 8817/523,183 (1.69) | 0.02.46 | 72.66 |
| Monthly average | 352.6 | 352.6 | ||
| New visitors | 7308 (66.21) | 5861 (66.47) | 0.02.43 | 75.95 |
| Return visitors | 3730 (33.79) | 2956 (33.53) | 0.02.52 | 65.57 |
| CPG-ADD (for patients/relatives) | 720/727,910 (0.10) | 600/523,183 (0.11) | 0.02.40 | 81.37 |
| Monthly average | 28.8 | 24 | ||
| New visitors | 530 (73.61) | 450 (75) | 0.02.21 | 85.29 |
| Return visitors | 190 (26.39) | 150 (25.00) | 0.03.16 | 61.76 |
CPG-OH: clinical practice guidelines on alcohol abuse; CPG-ADD: clinical practice guidelines on depressive disorder.
Most viewed clinical practice guides on the portal.
| Ranking | Guideline | Page views, n | Unique visitors, n | Length (min) | Bounce rate (%) |
|---|---|---|---|---|---|
| 1 | CPG-pregnancy | 39,905 | 22,445 | 1.56 | 64.88 |
| 2 | CPG-urinary tract infection | 28,169 | 18,160 | 2.25 | 64.03 |
| 3 | CPG-arterial hypertension | 23,297 | 18,392 | 3.10 | 43.02 |
| 4 | CPG-diarrhoeal disease | 22,024 | 17,880 | 2.42 | 49.46 |
| 5 | CPG-acute coronary syndrome | 17,314 | 14,192 | 2.45 | 72.24 |
| 6 | CPG-premature newborns | 16,884 | 8985 | 1.29 | 70.10 |
| 7 | CPG-healthy newborns | 13,175 | 11,228 | 2.31 | 68.50 |
| 8 | CPG-ADD | 11,038 | 8817 | 2.46 | 72.66 |
| 9 | CPG-asthma | 10,585 | 8236 | 2.22 | 64.66 |
| 10 | CPG-newborns with congenital abnormalities | 10,423 | 8953 | 3.00 | 71.14 |
| 11 | CPG-prostate cancer | 10,304 | 7727 | 2.33 | 70.41 |
| 12 | CPG-newborns with perinatal asphyxia | 10,186 | 8150 | 2.12 | 76.53 |
| 13 | CPG-leukaemia | 10,036 | 7466 | 1.58 | 66.45 |
| 14 | CPG-newborns with neonatal sepsis | 9847 | 8058 | 1.55 | 77 |
| 15 | CPG-breast cancer | 9148 | 7225 | 2.39 | 63.88 |
| 16 | CPG-OH | 8830 | 7026 | 2.20 | 72.49 |
| 17 | CPG-newborns with respiratory disorder | 7317 | 5848 | 2.21 | 70.10 |
| 18 | CPG-rectal cancer | 6614 | 5410 | 2.16 | 67.89 |
| 19 | CPG-lymphoma | 6448 | 4694 | 2.02 | 73.53 |
| 20 | CPG-urinary tract infection (patients) | 2461 | 2068 | 2.35 | 84.81 |
| 26 | CPG-ADD (patients) | 720 | 600 | 2.40 | 81.37 |
| 27 | CPG-OH (patients) | 643 | 543 | 3.13 | 75.54 |
CPG: clinical practice guidelines; OH: alcohol; ADD: depressive disorder.
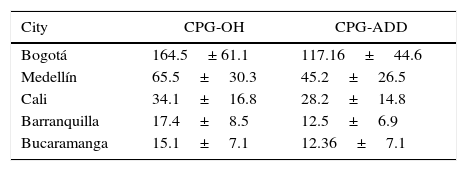
Most healthcare professionals accessed the guidelines from the city of Bogotá. Table 3 shows the average page views from each city. There was no difference in the average page views on the CPG-OH and CPG-ADD (p=0.2); access patterns according to city were similar for both guidelines (Fig. 4).
Average number of page views per month on clinical practice guidelines by healthcare professionals according to city.
| City | CPG-OH | CPG-ADD |
|---|---|---|
| Bogotá | 164.5± 61.1 | 117.16±44.6 |
| Medellín | 65.5±30.3 | 45.2±26.5 |
| Cali | 34.1±16.8 | 28.2±14.8 |
| Barranquilla | 17.4±8.5 | 12.5±6.9 |
| Bucaramanga | 15.1±7.1 | 12.36±7.1 |
CPG-OH: clinical practice guidelines on alcohol abuse; CPG-ADD: clinical practice guidelines on depressive disorder.
The highest number of page views was made from Bogotá (both CPGs p<0.1).

The CPG-OH and CPG-ADD for patients and relatives were mostly viewed from cities other than the 5 main cities from which healthcare professionals accessed the guidelines. Compared with page views made by healthcare professionals, the CPG-OH for patients and relatives were viewed proportionately more often from cities such as Villavicencio, Cúcuta and Manizales, and the CPG-ADD for patients and relatives were viewed more often from Villavicencio, Pasto and Pereira (Fig. 5).
Discussion
The use of portal access pattern analysis to evaluate CPG implementation strategies is rarely used in the scientific literature related to the use and implementation of evidence-based medicine, and we were only able to find a few isolated data. For example, the National Institute for Health and Care Excellence (NICE) reports that its website receives one million page views per month, but does not describe other measurements or usage patterns.15 India's Maternal Child Healthcare portal, which contains various evidence-based documents and recommendations for the care of pregnant women and newborn babies, used Google Analytics to describe portal usage patterns, and reported that since the launch of the portal in July 2010, it has received 44 unique visitors per month, with an average session of 4min and a bounce rate of 27.6%.16 Apart from the above sites, however, there are no studies describing patterns of use of online libraries, even though knowledge exchange portals (KEP) are emerging as useful platforms that can facilitate knowledge management and evidence-based decision-making in public health.17 KEPs typically contain information relevant to a specific health area and have a single point of access (web portal) that integrates all the different information and, depending on the characteristics of the site, the creation of new knowledge, the transfer of information and clinical practice decision-making support for users.18
Depressive disorder and alcohol abuse are prevalent and high-impact diseases in Colombia,19–21 and for this reason the Ministry of Health has prioritised the development of specific CPGs to address these problems. However, although recommendations for implementing CPGs have been drawn up,22 their impact on clinical practice is unknown, and information needs to be collected on the extent to which they are used. Researchers investigating evidence-based medicine must look to other industries, such as the financial and business sectors, to acquire knowledge management strategies that can be used to evaluate the impact and usefulness of their development strategies, which are today almost exclusively based on information and communication technologies (ICT).23
The analysis presented here is the first step in the implementation of knowledge management strategies in the healthcare sector. It provides information on CPG usage patterns, and shows that the guidelines are accessed from the main cities in Colombia, and hardly ever from Amazonia and Orinoquía, with a high percentage of rebounds (ideally <50%) and an average session of <3min, with patients and relatives making very little use of the guidelines.
Although the portal has been promoted since its launch, and is included in the Guideline Implementation Manual,13 our findings suggest that it does not fulfil its purpose in reaching more remote regions. This could be due to poor Internet coverage, lack of dissemination of the CPGs, or lack of specialists in these remote areas. However, the CPGs were developed for use in the primary care setting, and 56% of the Colombian population now have access to the Internet,24 suggesting that poor dissemination in these regions could be responsible for the low number of views, and that inclusion in the Implementation Manual, whose use in health centres has never been evaluated, does not suffice to raise awareness of the existence of these CPGs. It is also striking to observe the short average session (≈3min) and a high bounce rate. Considering the complexity of the information contained in the guidelines, it would be reasonable to expect users to stay longer and explore related issues or use the resources available on the portal. This could be due to users downloading the PDF file directly without consulting the online version, or that the design of the portal does not attract users.
Finally, the number of page views on guidelines developed for patients and relatives is low. This is unfortunate, since Colombia is one of the few countries to have developed CPGs for the general public. Considering that the portal is the main documentary source of CPGs, it is safe to say that scant use is made of the resources available, and the website does not appear to reach its target population. This is of particular concern in the context of the psychiatric conditions addressed, in which the participation of the family is fundamental.
This study has several limitations, such as the inability to determine the demographic characteristics and the specialist fields of portal users. In addition, our results are limited to access patterns, and it is impossible to know whether the CPGs were read, implemented in clinical practice, or adapted to hospital services. Nevertheless, our findings show the need for some improvements to the portal: a) allow user registration, indicating the type of user (general practitioner, specialist, patient, etc.) and other demographic characteristics that can be used to create mailing lists and to distribute information. At a future date, this information could be used to define user needs, and would allow users to express their opinions and make suggestions, thus giving the developers information that would enable them to improve the portal and tailor it to the needs of its users; b) invigorate the portal and update the information presented, since it has remained practically the same since its launch in 2013; c) introduce the latest information viewing and management technologies that link the portal to mobile devices. The portal was originally launched along with mobile applications for iOS and Android, but these were withdrawn by the Ministry of Health and have not been updated, thus preventing users from accessing the CPGs and the information they contain directly from their office or from remote areas that only have mobile phone coverage, but no Internet. These strategies are in line with the E-Mental Health campaign, which has been shown to be effective, especially in remote areas where no specialists are available25; d) incorporate specific design rules for health-related websites, such as HON (Health on the Net)26; e) allow the portal to be promoted on social networks; f) reactivate sections of the portal that allow users to interact, such as the blog, the training section and user comments; and g) develop innovative ways to present guideline recommendations, such as animations, interactive flowcharts or decision trees.
The three psychiatry guidelines (Depressive Disorder, Alcohol Abuse and Schizophrenia) currently published on the CPG portal should form the basis for a strategy of dissemination and implementation of evidence-based decision-making that in turn revolves around digital knowledge management processes. At a future date, this strategy should include the use of metrics, such as those proposed in this study, which can guide communication and innovative implementation strategies based on epidemiological parameters such as, for example, disease prevalence according to geographical location, or the lack of specialists.
ICTs, including social networks, online research and medical informatics, are among the best means of disseminating health-related knowledge, both among the general population and among vulnerable or remote patient populations.26–28 In addition, recommendations on internet- or mobile device-based reporting of clinical experiments have already been drafted.29–32 Therefore, publishing psychiatry CPGs in digital format and on a Colombian website can improve the dissemination of health-related knowledge in such areas, and can form the basis for studies that more accurately measure the extent to which such knowledge reaches healthcare professionals and patients and their families, and its impact on the healthcare system and ministerial policies.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Suárez-Obando F., Restrepo C.G. Patrones de consulta en la web de las guías de práctica clínica sobree manejo del trastorno depresivo y el abuso-dependencia del alcohol. Rev Colomb Psiquiat. 2017;46:194–202.
