








Caregiver burden syndrome has been highlighted as a neglected problem, in which a dependent person’s caregiver must change their lifestyle while facing a range of stressors which they cannot always overcome. This leads to a state of physical and mental exhaustion, hindering the caregiver’s performance at their work environment.
ObjectiveTo define the caregiver burden syndrome prevalence among formal caregivers of mentally-ill dependent patients at Clínica del Oriente in the period 2016 II (July–December) and 2017 I (January–June).
Materials and methodsA descriptive cross-sectional observational study was carried out in a population of formal caregivers of with mental illness institutionalised at either of the two facilities of Clínica del Oriente, La Ceja and El Carmen de Viboral. We used a survey with sociodemographic, clinical and work-related variables, and the Zarit Burden Interview.
Results53 caregivers were analysed; 11 had the syndrome (20.8%), 17% had mild burden and 3.8% severe burden.
ConclusionThe prevalence of caregiver burden syndrome in formal caregivers was lower than found in studies on informal caregivers.
El síndrome de carga del cuidador se ha destacado a través del tiempo como una problemática ignorada, en la que el cuidador de una persona dependiente debe permutar su estilo de vida y enfrentarse a diferentes factores estresores que, en ocasiones, no alcanza a controlar, lo que desencadena un estado de agotamiento físico y mental, obstaculizando su desenvolvimiento en el entorno laboral.
ObjetivoDefinir la prevalencia de síndrome de carga del cuidador en cuidadores formales de paciente dependiente con enfermedad psiquiátrica en la Clínica del Oriente para el semestre 2016 II (julio-diciembre) y 2017 I (enero-junio).
Materiales y métodosSe ejecutó un estudio observacional descriptivo de corte transversal en una población de cuidadores formales de pacientes con enfermedad psiquiátrica institucionalizados en la Clínica del Oriente, la cual tiene 2 sedes, ubicadas en La Ceja y en El Carmen de Viboral. La investigación se realizó por medio de una encuesta con variables sociodemográficas, clínicas y laborales, y la escala de sobrecarga de Zarit y Zarit.
ResultadosSe analizó a 53 cuidadores, 11 cuidadores presentaron el síndrome (20,8%), el 17% presentaba sobrecarga leve y el 3,8% sobrecarga intensa.
ConclusiónLa prevalencia del síndrome de carga del cuidador en cuidadores formales fue menor a lo encontrado en estudios sobre cuidadores informales.
Caregiver burden syndrome (CBS) can be defined as a disorder that occurs in those people who play the role of primary caregiver for someone who becomes dependent due to various limitations, whether functional or mental. It is mainly characterised by physical and mental exhaustion.1
A caregiver is someone who assists or cares for another person affected by any type of disability, handicap or incapacity that hinders or prevents the normal development of their daily life activities or social relationships. He/she is in charge of meeting the physical and emotional needs of the patient on a daily basis, keeping him/her linked to society and providing him/her with affection, showing solidarity with the person suffering. There are two types of caregivers: formal and informal caregivers. The former are those who receive remuneration for performing the work of a caregiver, whether or not they are trained, and the latter are those who perform this work without remuneration and without being trained, motivated mainly by affection for the patient. This unpaid position is mainly filled by family.2
Currently, there are few records on the distribution of CBS in formal caregivers and studies have focused mainly on informal caregivers. Ignorance of the prevalence of the syndrome in formal caregivers has been identified as a problem, because failure to identify it can lead the professional caregiver to perform their work inadequately.
Studies carried out in informal caregivers have found a higher incidence of anxiety, depression and physical health problems.3 The difficulties they face are characterised mainly by feelings of burden, stress and sadness.4 Other psychiatric symptoms that appear in caregivers are irritability, a grieving reaction, dependence, fear of the disease, behavioural changes, a feeling of guilt for not being able to properly care for the patient, and affective alterations that can lead to the appearance of suicidal ideas.5
The work of caring for a person with dependency or disability implies seeing life in a different way, modifying the functions to which they are accustomed, making decisions in the midst of complicated alternatives, taking on responsibilities, or performing tasks and actions related to physical, social, psychological and religious care to meet the changing needs of the person cared for.6
What we propose to demonstrate is that, although the prevalence of CBS could be higher in informal caregivers due to the emotional burden that the work of caring for a family member involves, it is also common in formal caregivers due to the working conditions under which they exercise their profession. Among studies carried out in Colombia, one of them, carried out in Cali, reported a prevalence of CBS in informal caregivers of 47%.1
Early detection of caregiver burden syndrome allows for intervention to preserve the person’s health, which in turn impacts the health of the patient they care for.
Materials and methodsAn observational, descriptive, cross-sectional study was carried out in a population of formal caregivers of patients with psychiatric illness at the Clínica del Oriente centres in the cities of La Ceja and El Carmen, during the second semester of 2016 (July–December) and first semester of 2017 (January–June).
SampleThe shift roster was requested for the institution’s caregivers, who numbered 53. We used the roster to plan several visits the centres so as to make contact with all the staff. All the caregivers agreed to participate in the research and signed the informed consent for it.
Inclusion criteria- none–
Formal caregivers of institutionalised dependent patients at the Clínica del Oriente.
- none–
Caregivers of dependent patients who wished to participate voluntarily and signed the informed consent.
- none–
Formal caregivers diagnosed with a basic psychiatric illness before starting their work as caregivers.
- none–
Formal caregivers of a dependent psychiatric patient who did not wish to participate in the study.
In order to explain the study and its scope, the interested individuals were presented with the informed consent and the confidentiality agreement, which was read and explained so that there was no doubt about its content.
The sociodemographic and clinical variables of interest were recorded via a survey consisting of 34 questions.
The methodological instrument that best defines the presence of caregiver burden syndrome is the Zarit Scale (ZS), an objectively-rated psychometric test composed of 22 Likert-type questions with 1–5 points for each question. The results add up to a total score of between 22 and 110 points. This result classifies the caregiver as having: “no burden” (≤46), “mild burden” (47–55) or “severe burden” (≤56).1 The ZS has a sensitivity of 100%, a specificity of 77.7%, a negative predictive value of 86.6%, and a positive predictive value of 100%.7
Statistical analysisA Microsoft Excel database was created for the 53 caregivers and their responses to the variables of interest (sociodemographic, clinical and work variables). A univariate analysis was carried out, in which the frequency and percentage distribution of each variable were determined. Subsequently, a bivariate analysis was conducted on the OpenEpi platform in order to determine the possible association between the independent variables and burden by means of Fisher's exact test, taking into account a 95% confidence level (p < 0.05).
ResultsAfter collecting the information from the two centres of the Clínica del Oriente: La Palestina in the municipality of La Ceja, Antioquia, and the Santa Ana, in the municipality of El Carmen de Viboral, Antioquia, 53 surveys were collected.
Table 1 shows the frequencies of the sociodemographic variables of the 53 formal caregivers surveyed, of which 31 were female (58.5%). In terms of age, of the total population studied, 33 (62.2%) were under 30 years of age, 12 (22.6%) were between 31 and 49 years of age, and 2 (3.7%) were over 50 years of age. Regarding marital status, the majority were single (32/53, 60.3%). Likewise, the majority reported not having children (27/53, 50.9%). 58.4% (31/53) stated that they lived in the municipality of La Ceja. The most frequent socioeconomic stratum was stratum 3 (34/53, 64.1%), the majority in rental accommodation (23/53, 43.4%). Regarding the perception of satisfied basic needs, 83% (44/53) answered yes and 16.9% (9/53), no. Most caregivers (79.2%) provided financially for other people. 88.6% (47/53) belonged to the Catholic religion and the rest were Christians, Jehovah’s Witnesses or did not practise any religion.
Sociodemographic variables of formal caregivers from the Clínica del Oriente, 2017.
| Variable | No. | % |
|---|---|---|
| Gender | ||
| Female | 31 | 58.5 |
| Male | 22 | 41.5 |
| Age, years | ||
| 30 or under | 33 | 62.3 |
| 31–49 | 12 | 22.6 |
| 50 or over | 2 | 3.8 |
| Did not respond | 6 | 11.3 |
| Marital status | ||
| Single | 32 | 60.4 |
| Cohabiting | 9 | 17.0 |
| Married | 7 | 13.2 |
| Separated | 5 | 9.4 |
| Number of children | ||
| None | 27 | 50.9 |
| 1 child | 16 | 30.2 |
| 2 or more children | 10 | 18.9 |
| Nursing home | ||
| La Ceja | 31 | 58.5 |
| Rionegro | 11 | 20.8 |
| El Carmen | 6 | 11.3 |
| Medellín | 2 | 3.8 |
| El Retiro | 1 | 1.9 |
| La Unión | 1 | 1.9 |
| Santuario | 1 | 1.9 |
| Socio-economic stratum | ||
| Stratum 2 | 13 | 24.5 |
| Stratum 3 | 34 | 64.2 |
| Stratum 4 | 3 | 5.7 |
| Did not respond | 3 | 5.7 |
| Type of accommodation | ||
| Rental | 23 | 43.4 |
| Family home | 11 | 20.8 |
| Own home | 19 | 35.8 |
| Perception of needs | ||
| Yes | 44 | 83.0% |
| No | 9 | 17.0 |
| Dependents | ||
| None | 11 | 20.8 |
| 1 person | 14 | 26.4 |
| 2 or more people | 28 | 52.8 |
| Religion | ||
| Catholic | 47 | 88.7 |
| Christian | 2 | 3.8 |
| Jehovah’s Witness | 1 | 1.9 |
| None | 2 | 3.8 |
| Did not respond | 1 | 1.9 |
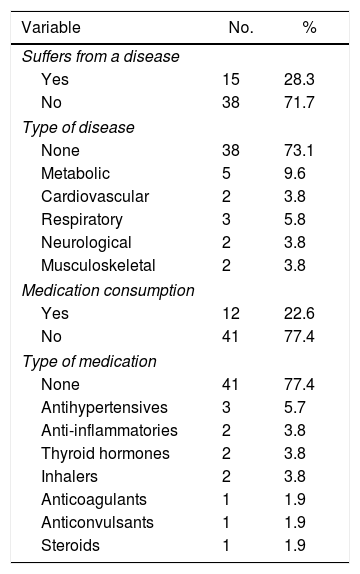
Table 2 shows the frequencies of the clinical variables. Of the 53 caregivers surveyed, the majority responded that they did not have any disease, 71.7% (38/53), and 28.3% (15/53) had some disease, with metabolic diseases being the most frequent (5/53, 9.6%). Regarding the consumption of drugs, 77.4% (41/53) of those surveyed did not consume any medication and of the 22.6% (12/53) who did consume medications the majority used antihypertensive drugs (3/53, 5.7%).
Clinical variables of formal caregivers from the Clínica del Oriente, 2017.
| Variable | No. | % |
|---|---|---|
| Suffers from a disease | ||
| Yes | 15 | 28.3 |
| No | 38 | 71.7 |
| Type of disease | ||
| None | 38 | 73.1 |
| Metabolic | 5 | 9.6 |
| Cardiovascular | 2 | 3.8 |
| Respiratory | 3 | 5.8 |
| Neurological | 2 | 3.8 |
| Musculoskeletal | 2 | 3.8 |
| Medication consumption | ||
| Yes | 12 | 22.6 |
| No | 41 | 77.4 |
| Type of medication | ||
| None | 41 | 77.4 |
| Antihypertensives | 3 | 5.7 |
| Anti-inflammatories | 2 | 3.8 |
| Thyroid hormones | 2 | 3.8 |
| Inhalers | 2 | 3.8 |
| Anticoagulants | 1 | 1.9 |
| Anticonvulsants | 1 | 1.9 |
| Steroids | 1 | 1.9 |
Table 3 shows the frequencies of the work variables. Of the 53 caregivers surveyed, 28 (52.8%) had had their job for less than two years, and 42 (79.2%) were freelancers. The position most commonly held was that of trainer (39/53, 73.6%), and 92.5% (49/53) worked from 6 to 12 h a day with at least one hour of break time according to 90.6% (48/53) of those surveyed. Regarding the number of patients under their care, 68.0% (18/53) of the caregivers stated that they took care of an average of 30–60 patients per day. Regarding the time invested in travelling to the institution, 94.3% (50/53) reported spending less than 60 min. Of these, 56.6% (30/53) travelled by private transport and 43.4% by public transport (23/53). 100% (53/53) of those surveyed stated that they had a good relationship with their co-workers. 94.3% (50/53) felt comfortable with the position held and 5.7% (3/53) did not. 79.2% (42/53) stated that they had time for recreation and 20.8% (11/53) did not. Likewise, 94.3% (50/53) reported having time for their family and 86.8% (46/53) reported having time to rest. 56.6% (30/53) of those surveyed stated that they were happy with their salary and 43.4% (23/53) were not. 100% (53/53) reported having a good relationship with their boss.
Work variables of formal caregivers from the Clínica del Oriente, 2017.
| Variable | No. | % |
|---|---|---|
| Time at the institution | ||
| Under 2 years | 28 | 52.8 |
| More than 3 years | 13 | 24.5 |
| 2–3 years | 10 | 18.9 |
| Did not respond | 2 | 3.8 |
| Contract type | ||
| Freelance | 42 | 79.2 |
| Service provision | 11 | 20.8 |
| Position at the institution | ||
| Trainer | 39 | 73.6 |
| Nursing assistant | 14 | 26.4 |
| Daily working hours | ||
| 6 h or less | 1 | 1.9 |
| 6–12 h | 49 | 92.5 |
| 12 h or more | 3 | 5.7 |
| Work breaks | ||
| 1 h or less | 48 | 90.6 |
| More than 1 h | 5 | 9.4 |
| Patients in their care | ||
| 30 or under | 18 | 34.0 |
| 30–60 | 18 | 34.0 |
| 60 or more | 16 | 30.2 |
| Did not respond | 1 | 1.9 |
| Home-work travel time | ||
| Under 60 min | 50 | 94.3 |
| Over 60 min | 3 | 5.7 |
| Means of transport | ||
| Private | 30 | 56.6 |
| Public | 23 | 43.4 |
| Relationship with colleagues | ||
| Good | 53 | 100 |
| Enjoys what he/she does | ||
| Yes | 50 | 94.3 |
| No | 3 | 5.7 |
| Recreation time | ||
| Yes | 42 | 79.2 |
| No | 11 | 20.8 |
| Time for family and friends | ||
| Yes | 50 | 94.3 |
| No | 3 | 5.7 |
| Time to rest | ||
| Yes | 46 | 86.8 |
| No | 7 | 13.2 |
| Salary satisfaction | ||
| Yes | 30 | 56.6 |
| No | 23 | 43.4 |
| Relationship with boss | ||
| Good | 53 | 100 |
Fig. 1 shows the prevalence of CBS, which occurred in 11 of the interviewed caregivers (20.8%). Of these 11 formal caregivers, 17% had mild burden and 3.8% severe burden (Fig. 2).


Table 4 shows the bivariate analysis of the factors that were considered related to CBS. It was found, with respect to the sociodemographic variables, that the caregivers most affected by the syndrome, without any statistically significant association, were those of male sex, aged 50 years or less, single, without children, from socioeconomic stratum 3, in rental accommodation and with more than two people to support. According to a comparison with the clinical variables, it was possible to show that most of the caregivers with the syndrome did not present with any disease, without statistically significant association. With regard to work variables, caregivers who had been at the institution for under three years, who were trainers, with time off from work of an hour or less, with 30 patients or less, with travel time between home and work under 60 min, with time for recreation, family and friends, and those who considered that their salary was inadequate were the most affected by CBS, without a statistically significant association. Only one variable was statistically significant (p < 0.05), in which it was found that 100% of the workers who answered that they were not enjoying their job had the syndrome.
Association between caregiver burden syndrome and risk variables.
| Caregiver burden syndrome | |||
|---|---|---|---|
| Variable | Yes | No | p |
| Gender | |||
| Female | 5 | 26 | 0.49 |
| Male | 6 | 16 | |
| Age | |||
| 50 or over | 1 | 1 | 0.38 |
| 50 or younger | 9 | 36 | |
| Marital status | |||
| Single | 7 | 25 | 1 |
| Other | 4 | 17 | |
| Number of children | |||
| No children | 7 | 20 | 0.5 |
| Children | 4 | 22 | |
| Socio-economic stratum | |||
| Stratum 2 | 3 | 10 | 0.7 |
| Other strata | 7 | 30 | |
| Type of accommodation | |||
| Rental | 5 | 18 | 1 |
| Own home | 6 | 24 | |
| Basic needs satisfied | |||
| No | 2 | 7 | 1 |
| Yes | 9 | 35 | |
| Dependents | |||
| 1 or more people | 8 | 34 | 0.67 |
| None | 3 | 8 | |
| Presence of diseases | |||
| Yes | 5 | 10 | 0.25 |
| No | 6 | 32 | |
| Time at the institution | |||
| Under 3 years | 9 | 29 | 0.7 |
| More than 3 years | 2 | 11 | |
| Position at the institution | |||
| Trainer | 1 | 29 | 0.25 |
| Nursing assistant | 1 | 13 | |
| Break time | |||
| 1 h or less | 1 | 38 | 1 |
| More than 1 h | 1 | 4 | |
| Daily work hours | |||
| 12 h or less | 10 | 40 | 0.5 |
| 24 h | 1 | 2 | |
| Patients in their care | |||
| 60 or less | 7 | 29 | 1 |
| 61 or more | 3 | 13 | |
| Home-work travel time per day | |||
| Over 60 min | 2 | 1 | 0.1 |
| Under 60 min | 9 | 41 | |
| Enjoys what he/she does | |||
| Yes | 3 | 0 | 0.007 |
| No | 8 | 42 | |
| Recreation time | |||
| No | 2 | 1 | 0.1 |
| Yes | 9 | 41 | |
| Time for family and friends | |||
| No | 1 | 2 | 0.5 |
| Yes | 10 | 40 | |
| Time to rest | |||
| No | 8 | 38 | 0.14 |
| Yes | 3 | 4 | |
| Adequate salary | |||
| No | 7 | 16 | 0.17 |
| Yes | 4 | 26 | |
An observational descriptive cross-sectional study was carried out in a population of formal caregivers of dependent patients from the Clínica del Oriente. After applying the instrument to diagnose CBS and collecting the corresponding information obtained in both locations of the Clínica del Oriente, it was observed that, of the 53 caregivers surveyed, 58.4% were women, which is consistent with the study conducted in 2007, where it was noted that 87.3% of women were responsible for carrying out the role of caregiver.4 Among the caregivers, it was found that 62.3% were aged 30 years or less and the majority were single (60.4%), which is consistent with the study carried out in 2015 in which the majority of those who filled the role of caregiver were people between 23 and 32 years old (47%) and of single marital status (54%).8 However, there was also a contrast with the 2010 study, in which the majority of caregivers were approximately 39.5 years old. Regarding the socioeconomic stratum, in our study the majority belonged to socioeconomic stratum 3 (64.2%), which differentiates it from the last cited study, in which the majority of caregivers belonged to socioeconomic stratum 4 (66%).8
An article published in 20089 reported that the majority of caregivers presented with moderate burden, a fact that differs from what was found in the present investigation, in which the majority of caregivers did not present with burden (79.2%) and, of those who did have the syndrome, most had mild burden, which can be attributed to the time spent with patients during a day. Regarding this, it was found that 97.5% of caregivers worked between 6 and 12 h a day. Of these, 10 people experienced burden. Only one worker of the three who worked 24 h presented with burden.
The article published in 20083 reported that the majority of the caregivers with CBS were nursing staff from a nursing home for the elderly, which differs from the present study, in which the majority held the position of trainer.
It should be noted that 13.2% and 20.8% of the respondents reported not having time to rest or do recreational activities, respectively, which indicates that caregivers lack adequate coping strategies to adapt to the situation, as the 1999 study made reference to.10
It should be mentioned that 22.6% of the caregivers used medications, a fact that is significant if we look at other studies (Pérez, 2006 and Crespo and López, 2004), where more than 30% of the caregivers used drugs to sleep or calm their nerves on a regular basis. 28.3% of those surveyed had some disease, with metabolic diseases being predominant (9.6%). In various studies, associations were found between high levels of stress and physical health problems, and use of psychotropic medication and chronic problems.
A meta-analysis carried out in 200311 revealed that caregivers were at higher risk of developing health problems than those who were not.
Regarding the personnel who presented with mild work burden, it was revealed that more than 50% of subjects were male, of which the vast majority were single or divorced, an element that is presented as a social risk factor in this group, since these personnel are at greater risk of having less social and emotional support due to not having a stable partner. It is also evident that the majority were trainers, who within their position and with respect to the assistants, have more responsibility for the patients and the assistants who assist them in their daily activities and, therefore, are exposed to more stress during their workday.
When observing the economic variables of this same group of personnel with mild work burden, it is evident that notably only two people reported not having their basic needs met, and the rest affirmed that they were met satisfactorily. However, only one person with mild burden reported being paid an adequate salary for their work. The rest felt that their salary was insufficient for their work, while the majority of the staff that was not part of the group that presented with work burden of some kind stated that they received adequate remuneration, a factor that plays a key role in perceiving work burden, since the monetary motivational factor is important in how the staff perceive their job and in how they face the various day-to-day circumstances and situations during their shifts, which, for the majority of this group, last 12 h, with an emphasis on dedicating more than 95% of the shift to the close care of their patients, and with 95% of this group being responsible for more than 30 patients for each shift. The sum of the aforementioned factors forces us to think about an increase in emotional burden, work stress, physical and mental exhaustion, and anxiety about providing care, mainly due to feelings of burden, stress and sadness.
The population that presented with severe burden demonstrated by the score obtained in the ZS was observed to be female, in charge of more than 30 patients, with 12-h shifts, spending 11 h providing close care for these users, and feeling that they did not receive adequate remuneration for their work. Their place of work was the Santa Ana centre, located in El Carmen de Viboral, where all patients with severe mental retardation, who require more care and are more dependent on their caregivers, are hospitalised. It is evident that the sum of these factors leads to the presentation of a severe work burden.
CBS was found in 20.8% of the formal caregivers interviewed at the institution, 17% had mild burden and 3.8% severe burden. This percentage is lower than the prevalence found in other studies. For example, in a study carried out in 2015 in the main caregivers of patients in palliative care at a university hospital, a 67% burden was found, of which 43% was severe burden and 24% mild burden.12
ConclusionsCBS was found in 20.8% of the formal caregivers interviewed at the institution, of whom 17% had mild burden and 3.8% severe burden. This percentage is lower than the prevalence found in other cited studies in informal caregivers. This may be explained by the different risk factors presented by informal caregivers compared to formal ones: caring for a sick family member, not receiving financial remuneration and performing care work for more hours a day.
A higher prevalence of CBS was evidenced at the Santa Ana centre, located in El Carmen de Viboral, where there was a greater number of patients with profound mental retardation, who are more dependent on their caregivers and require more attention, time and care. However, it is important to carry out studies that analyse the degree of dependence of patients and its association with the degree of burden of caregivers.
Most of the caregivers who presented with CBS were performing training tasks, and, within their position and with respect to the nursing assistants, had more responsibility for the Clínica de Oriente patients.
A significant association was demonstrated between severe burden and not doing an activity with which one is fully compatible.
LimitationsThe degree of dependence of patients admitted to the Clínica de Oriente was not evaluated with validated scales, which could have been helpful in finding possible associations between the degree of dependence and the degree of burden.
The sample used for the study was small, so the associations found could be due to biases. Studies with larger populations are required. A poor perception of the work environment on the part of the caregivers could have intervened so that they answered the questionnaire in an inadequate way and that, finally, they were diagnosed with CBS when it really was a possible dissatisfaction with their work and not something really related to their care work.
FundingThe resources used to carry out this research project were those of the authors of this article. No funding from other sources was received.
Conflicts of interestThe authors have no conflicts of interest to declare for this investigation.
We would like to thank the Clínica del Oriente institution, Dr Ramón Lopera, the staff and each of the caregivers for opening their doors, allowing us to carry out the study and being willing to participate in it, and making it possible to prepare and obtain the results. Likewise, we would like to thank the methodological advisor, Jorge Emilio Salazar, for his willingness and perseverance, in addition to the support he provided during the preparation of the work.
Please cite this article as: Henao Piedrahita N, Idarraga Arroyave MM, Londoño Restrepo N, López Ceballos JJ, Ramírez Serna MA, Serna Arango PA, et al. Prevalencia del Síndrome de Carga del Cuidador en Cuidadores Formales de Pacientes con Enfermedad Psiquiátrica Institucionalizados. Rev Colomb Psiquiat. 2021;50:101–107.
