




Objetivo. El objetivo de este estudio es establecer el perfil termográfico de los miembros inferiores en jóvenes jugadores de fútbol de élite.
Método. En el estudio participaron 100 jugadores de fútbol de categorías sub-19 de clubes de fútbol brasileños de primera división (15,5 ± 1,37 años; 67,93 ± 9,62 kg; 177,49 ± 8,67 cm). Mediante dos termogramas se obtuvieron las temperaturas máximas y medias de la piel (TSK) de cuatro regiones corporales de interés (RDI) correspondientes a la vista anterior y posterior de la pierna y del muslo. Se empleó el test de Wilcoxon para comparar las diferencias de la TSK bilateral, con un nivel de significación α < 0,05.
Resultados. Los valores medios de la TSK en la vista anterior fueron los siguientes: muslo derecho 30,2 ± 1,9°C, muslo izquierdo 30,2 ± 1,9°C, pierna derecha 29,8 ± 1,8°C y pierna izquierda 29,9 ± 1,8°C. En la vista posterior, los valores fueron los siguientes: muslo derecho 30,3 ± 1,8°C; muslo izquierdo 30,2 ± 1,8°C; pierna derecha 29,6 ± 1,9°C y pierna izquierda 29,4 ± 1,9°C. El análisis estadístico no mostró diferencias significativas en las temperaturas medias o máximas tomadas en las RDI elegidas. Un histograma de las frecuencias de TSK para cada RDI permitió establecer valores para hiper e hipotermia.
Conclusión. Los jóvenes jugadores de fútbol de élite analizados mostraron simetría térmica contralateral. La TSK media para pares de RDI era para cada uno≤ 0,2°C. Cada RDI mostró un perfil térmico específico. La TSK mostró un perfil térmico normal de los atletas.
Objective. The objective of this study was to establish the thermographic profile of the lower limbs in elite young soccer players.
Method. One hundred soccer players from the U-19 categories of a first division Brazilian football club (15.5 ± 1.37 years; 67.93 ± 9.62 kg; 177.49 ± 8.67 cm) participated in the study. Two thermograms allowed us to record maximum and average skin temperatures (TSK) in four body regions of interest (ROIs) of the lower limbs corresponding to the anterior and posterior view of the leg and thigh. The Wilcoxon test was used to compare bilateral TSK differences with a significance level of α < 0.05.
Results. Average values of TSK in the anterior view were as follows: right thigh 30.2 ± 1.9°C, left thigh 30.2 ± 1.9°C, right leg 29.8 ± 1.8°C, and left leg 29.9 ± 1.8°C. In the posterior view, the values were as follows: right thigh 30.3 ± 1.8°C, left thigh 30.2 ± 1.8°C, right leg 29.6 ± 1.9°C, and left leg 29.4 ± 1.9°C. The statistical analysis did not show significant differences between sides in the selected ROIs for average or maximum temperatures. A histogram of TSK frequencies for each ROI allowed establishment of values for hyper-and hypothermia.
Conclusion. The elite young soccer players analyzed showed contralateral thermal symmetry. The average TSK differences for paired ROIs were each ≤ 0.2°C. Each ROI exhibited a specific thermal profile. The registered TSK indicated a normal thermal profile of the athletes.
INTRODUCTION
The development of new technologies applied to sport has allowed better understanding of the physiological responses to training and competition, has helped to determine the appropriate training load and has provided information about the physical condition of athletes. There have been published studies monitoring heart rate1-2, controlling creatine kinase3 or global positioning system (GPS)4. Recently, infrared thermography (IRT) has been proposed as a tool to be employed5-8, with interesting applications both in sports medicine9-10 and physical therapy11 or as a way of determining training load12.
IRT is a technique that records the radiant heat of a body by recording infrared emission, which lies in a range of the electromagnetic spectrum that the human eye is unable to identify9,13. This technique allows visualization of the temperature of the body surface in real time with sensitivity up to 0.025°C and precision reaching 1 %, non-invasively and without any physical contact with the subject14. Other advantages of the technique are that it is fast and harmless, highly reproducible, and does not involve the emission of radiation14-16. These characteristics enable scientists to obtain the general and local thermal profile of the subject and, if performed routinely, to conduct real-time monitoring of skin temperature (TSK), gathering information about the complex thermoregulatory system of the human body13.
In the medical field, IRT has been used to identify a number of problems related to different types of pain syndromes17, changes in the skin18, vascular defects19, neurological defects20, muscle and tendon injuries9-10, all of which have direct applications to sports.
The use of IRT has also been linked to the prevention of orthopedic injuries21-22. Under normal conditions, TSK is similar between the sides of the body23. TSK differences greater than 0.7°C between contra-lateral limbs or body areas have been associated with structural or physiological abnormalities in athletes6,9. Thus, IRT can be an important tool in preventing injuries when bilateral thermal differences are identified.
To allow meaningful interpretation of thermographic data, it is necessary to establish a normal profile in different population groups without any pathology. Studies to this end are few, but there is some research that has established thermal profiles in populations of non-athletes in groups of Chinese24, Finnish25, Portuguese26, Thai27, and even in Mexican children28. These data allow us to evaluate thermal normality in different body segments and to observe bilateral differences.
No reference baseline study has been performed to characterize the epidemiological thermography profile of athletes, especially in soccer players. The construction of these TSK normative data can help establish normal patterns in different parts of the body, with a focus on the lower limb, allowing skin assessment of general or local hyperthermic or hypothermic conditions. TSK differences between hemispheres may indicate the presence of a problem and may reduce the subjectivity of the assessment. Establishment of normal values at rest may also contribute to the understanding of changes in TSK and allow the use of IRT as an exploratory analysis tool in clinical settings including physical therapy or physical training. Thus, the aim of this study was to establish thermographic profiles of the lower limbs in young soccer players, which will serve as a starting point for future applications of this technique in soccer.
METHOD
This cross-sectional study analyzed 100 soccer players in the basic categories of a Brazilian first division soccer club aged between 15 and 19 years (age: 15.5 ± 1.37 years, body mass: 67.93 ± 9.62 kg and height: 177.49 ± 8.67 cm). Leg dominance was right-sided in 77 and left-sided in 23 cases. The subjects performed systematized training five times a week, 90 minutes per session, during the preparatory period of the season.
The study was approved by the Ethics Committee of the Federal University of Viçosa (UFV), with registration number 40928260540, following all of the criteria set forth by the Brazilian legislation for human studies, in accordance with National Health Board Resolution 196/96. Because the study subjects were minors, permission for them participate was given by their parents; all subjects were volunteers and received no reward.
Considering that TSK measurements are prone to multiple sources of interference, the following exclusion criteria were applied: a) history of kidney problems; b) performing physical therapy in the past two days; c) consuming any diuretic or antipyretic drug and any food supplement such as creatine that could interfere with water or body temperature homeostasis in the last two weeks; d) smoking; e) skin burns; f) topical treatments with creams, ointments or lotions; g) pain symptoms in any region of the body; h) fever in the last seven days; i) sleep disorders; and j) musculoskeletal injuries meeting the criteria of the Fédération Internationale de Football Association Medical Assessment and Research Centre (F-MARC)29. These injury criteria include any physical complaint reported by a player due to training or during a football game, regardless of needing medical attention or stopping the football activity. All subjects reported the absence of any type of sports injury according to these criteria.
Thermographic images were collected using a thermal imager IRT-25 (Fluke®, Everett, USA) with a measurement range of -20 to +350°C, an accuracy of ± 2°C or 2 %, a sensitivity of ≤ 0.1°C, an infrared spectral band from 7.5 to 14 microns, a refresh rate of 9 Hz and an FPA (Focal Plane Array) of 160 x 120 pixels. The distance between the subject and the camera was 4 m, and the index of human skin emissivity was set to 0.98.
Data collection followed the standards proposed by the European Association of Thermology30. The images were taken in the morning before performing any intense physical exercise or training in the previous 24 hours. The temperature during data collection was maintained at 21 ± 1°C, and the acclimation period was set at 15 minutes, surpassing the minimum time of 8 minutes of stabilization proposed in 2012 by Roy et al.31. Prior to and during the procedure, the subjects were asked to avoid any sudden and intense movement, or rubbing, scratching or crossing their legs.
Two thermograms were taken for each evaluation (anterior and posterior); body regions of interest (ROIs) analyzed included the thighs and legs. These regions were selected by a rectangle bounded by the software (Smartview 3.1 - Fluke®, Everett, USA), which provided us with the average and maximum temperatures from each analyzed ROI.
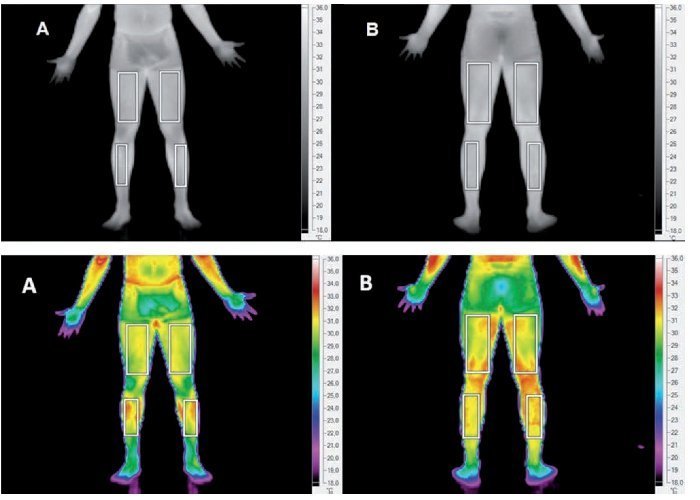
To configure the ROI, we followed the recommendations of Moreira32, who proposed drawing rectangular areas referenced by the following anatomical landmarks: for the thigh, 5 cm above the upper border of the patella and groin line, and for the leg, 5 cm below the lower border of the patella and 10 cm above the malleolus. The points corresponding to the posterior regions were marked parallel to the ground with a measuring tape determining the anterior points by marking a circumference around the analyzed region. Figure 1 shows two thermal images, anterior (A) and posterior (B), of the lower limbs with the ROI used in the study.
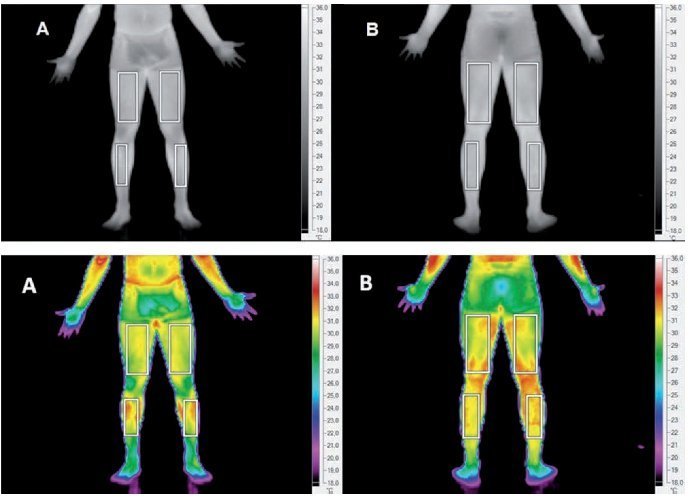
Fig. 1. Thermograms of the anterior (A) and posterior (B) lower limbs, highlighting the ROI for the assessment of TSK.
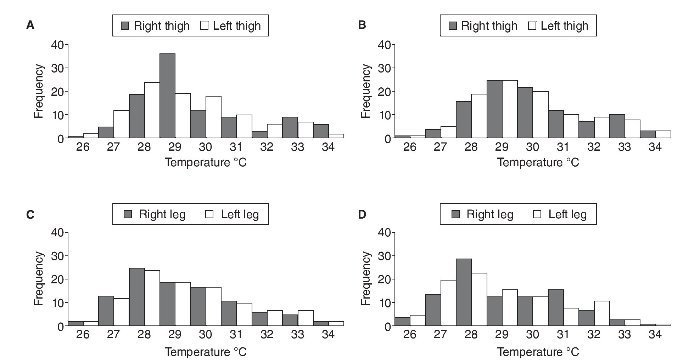
The average and maximum TSK of each ROI were considered for the statistical analysis. Subsequently, these data were transferred to Sigma-plot 11.0 software. The results of frequency analysis of the recorded TSK
were grouped in ranges of occurrence of temperature from 26°C to 34°C and are represented by a histogram (fig. 2). The normality of the data was assessed by the Shapiro-Wilk test, and differences between the right and left sides were detected by the Wilcoxon test. In addition, intraclass correlation coefficients (ICCs) were used to probe the reliability and reproducibility of the paired values for each ROI. A significance level of α < 0.05 was adopted for all calculations.
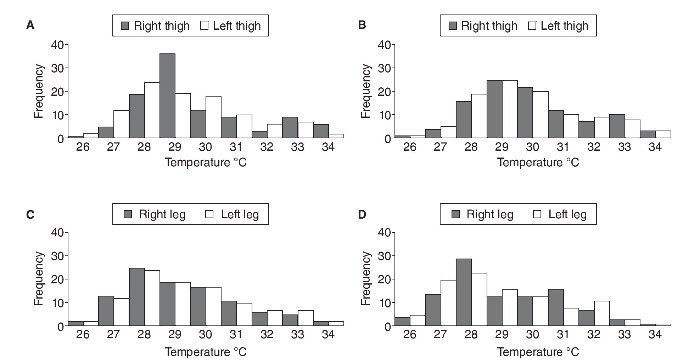
Fig. 2. Frequency distribution of the averaged TSK (°C) in the lower extremities. Anterior (A) and posterior (B) thigh and anterior (C) and posterior (D) leg.
RESULTS
Table 1 and table 2 show the mean values and standard deviations of the mean and maximal skin temperatures (TSK), respectively, for each ROI and their intra-class correlation coefficients (ICCs).


The results of the statistical analysis reached non-significant differences (p < 0.05) in the comparison between both sides in the selected ROIs for both the average and maximum temperatures. In addition, the high CCI levels suggest high reliability and reproducibility of the measurements.
Figure 2 summarizes the frequency distribution of the averaged TSK in the studied players in the thigh and leg in anterior and posterior views.
DISCUSSION
The main finding of this study was the identification of TSK symmetry between contralateral sides of the studied ROIs in young soccer players for both the average and maximum TSK (tables 1 and 2, respectively). There was a non-significant difference (< 0.2°C) in the averaged TSK between the left and right sides in anterior and posterior views of both the thigh and leg for the soccer players studied (table 1). Analyzing the obtained maximum TSK in each ROI, we again found an average difference < 0.1°C (table 2).
Our results point to a thermal equilibrium of TSK in the studied ROIs. Given that none of the soccer players had a diagnosed injury, the data support the fact that, under normal conditions and as a reference standard for thermographic evaluation of soccer players, there should be a thermal symmetry between contralateral regions.
The normal range of temperature differences between a ROI and its corresponding contralateral region both in normal subjects and in athletes has not yet been established. Some authors have suggested different values (0.3°C33, 0.4°C34 or 0.5°C27) in a population of non-athletes. In athletes, Hildebrandt et al.9 established a value greater than 0.7°C as the limit of asymmetry between contralateral ROIs. The results of our study indicated a range of symmetry lower than any previously reported in the literature. However, further exploratory studies are needed to establish the normal reference range more reliably.
With regard to the differences between the ROI in the anterior leg, asymmetry is acceptable considering the reference threshold of 0.7°C for athletes proposed by Hildebrandt et al.9; however, a total of nine cases showed the temperature of the right leg to be higher than in the left leg. It is of value to note that Gómez-Carmona et al.35 reported significantly higher TSK values in the dominant leg in professional soccer players, likely due to greater physical load on this leg. This observation is considered a typical characteristic of the soccer player's thermal profile, without association with any risk of injury. When these nine athletes were analyzed individually, we observed that in all cases, the TSK was higher in the dominant leg, which agrees with this theory and may explain these results. Such differences may represent a specific thermoregulatory behavior in this sample; taking into consideration that no athletes in the study reported any pain or injury.
This issue of side dominance in athletes is interesting because the overload of some areas used in repetitive patterns of movement in sports such as tennis or judo could be linked to normal asymmetric thermal profiles, which are not considered normal in other sports (i.e., cycling or running) with symmetric movement patterns.
The average temperatures obtained in the lower limbs of the players evaluated (table 1) are in agreement with data reported by Niu et al.27 in an Asiatic sample, where the average values were almost identical in the anterior (30.2°C in right and left thighs) and in the posterior views (30.3°C right and left thighs). In the legs, the results were slightly higher in the posterior (30.4°C in right and left) and in the anterior views (29.9°C in left and right).
Continuous thermal monitoring of athletes allows their thermal profile to be established. An abnormal increase (acute or chronic) in the TSK in both legs or only in one of the contralateral ROIs may be related to an inflammatory process that may result in an injury. The microdamage in active muscles caused by training and competition is often accompanied by an inflammatory response and increased TSK in some areas12. Thus, IRT can be used to monitor the effects of the training load.
Identification of thermal imbalances may be key to injury prevention. Observation of a ROI with a TSK higher than usual (local hyperthermia) could be a sign of an inflammatory problem9-10,33, while local hypothermia may be suggestive of a degenerative process9-10,23 with reduced blood flow in the affected area.
Figure 2 shows the frequency distribution of the average TSK of the lower limbs and it illustrates a distinct profile between the regions of the thigh and leg. Higher temperatures are observed in the thigh area, which is expected as the closer the examined ROI is to the central body (formed by the major organs, which produce most of the body heat at rest), the higher its TSK 36. Thus, when we observe a reversal of this situation, the alteration of the normal thermal profile should be brought to the attention of the coaching staff.
In the thigh, the usual temperature ranges on the anterior and posterior views are normally between 29 and 30°C, encompassing 47.8 % of 400 ROIs analyzed. No normal TSK for soccer players has yet been established, making our work a pioneering endeavor. We propose that a TSK below 27°C may be related to a condition of hypothermia caused by reduced local blood flow, whereas a TSK above 33°C could suggest an inflammatory process. In both cases, we recommend reducing the load or even suspending training, performing a medical evaluation of the athlete and, when necessary, starting an appropriate physical therapy protocol.
In the leg, both the anterior and posterior distribution was more heterogeneous (between 27 and 32°C), suggesting the need for greater attention when TSK readings are out of this range. It is important to note that these temperature ranges depend on the analyzed ROI, the type of camera, the acclimation time and the climatic conditions of the room. If data collection is performed under other conditions, the normal ranges will change. Therefore, it is important to maintain standard conditions for measuring thermal images.
We recommend including thermographic evaluation in the daily training routine. The assessment history of each player allows the identification of any abnormality in the TSK with greater precision because each athlete will be compared to his habitual thermal profile.
One limitation of this study is the lack of longitudinal follow-up and objective imaging diagnoses (i.e., MRI or echography) to correlate the relationship between cases of TSK higher than 0.7°C with any physical problem in the area. However, the present study does provide the first thermographic profile of junior Brazilian soccer players, which could be a reference point for new studies and professional practice.
In conclusion, soccer players from the U-19 demonstrated contralateral thermal symmetry with an average TSK difference between ROIs of less than 0.2°C. This symmetric pattern suggests that athletes had a normal thermographic evaluation.
Acknowledgements
The authors express appreciation to the CNPq for the postdoctoral scholarship in area thermography, to the CAPES for the Master's scholarship, and to the FAPEMIG for funding the project.
Conflict of interest
The authors declare that they have no conflict of interest.
History of the article:
Received January 5,2013
Accepted July 10,2013
Correspondence:
J. C. Bouzas Marins.
Universidade Federal de Viçosa. Departamento de Educação Física - LAPEH.
Av. PH Rolfs s/n - Campus Universitário CEP: 36570-900 - Viçosa - MG - Brasil.
E-mail: jcbouzas@ufv.br
