








Laparoscopic Heller miotomy of achalasia has been classically recognized as the gold standard management in children. There is increasing experience with the peroral endoscopic miotomy (POEM) approach in pediatrics, although the series published are scarce. The objective of this study was to present our experience in primary or secondary treatment of pediatric achalasia by POEM and its clinical success rate.
MethodsWe performed a retrospective review of pediatric patients with achalasia who underwent POEM in some national centers from October 2016 to January 2023. We evaluated clinical efficacy (Eckardt score ≤3), demographic characteristics, intraoperative, preoperative and postoperative, complications, and follow-up.
ResultsFifteen POEM were performed in fourteen pediatric patients (aged 12–18 years) with achalasia. POEM was the first line treatment in 11 patients, but 4 (21.3%) had previous treatment: 1 (7,1%) pneumatic balloon dilation and 2 (14,2%) laparoscopic Heller myotomy and 1 (7,1%) previous POEM. The average age was 15 years (SD ± 1,9). The baseline Eckardt score was 7,5 (SD: ± 1,8), with the baseline GERD score being 6 (SD: ± 2,9). There was a Clavien-Dindo grade 2 postoperative adverse event corresponding to mild pneumonia (7,1%). The postoperative Eckardt and GERD score after 12 months of follow-up were 0.7 (SD ± 1,2) and 0,5 (SD ± 0,7). The study has a success rate greater than 93%.
ConclusionsPOEM seems a safe and effective procedure, with a short postoperative period for treatment of pediatric achalasia.
El tratamiento laparoscópico de la acalasia ha sido reconocido clásicamente como el de elección en pediatría. Existen pocos artículos sobre el abordaje mediante miotomía endoscopia por vía oral (POEM). El objetivo de este estudio es presentar nuestra experiencia en el tratamiento mediante POEM como tratamiento inicial o de segunda línea para la acalasia pediátrica y valorar su eficacia clínica.
MétodosRevisión retrospectiva multicéntrica nacional de los pacientes pediátricos con acalasia intervenidos mediante técnica POEM desde octubre de 2016 hasta enero de 2023. Se incluyen datos demográficos, intraoperatorios, Eckardt score y GERD preoperatorios y posoperatorios, complicaciones y seguimiento. Se considera éxito clínico Eckardt score ≤ 3.
ResultadosSe realizaron 15 POEM en 14 pacientes pediátricos con acalasia; 11 como primera línea y cuatro (21,3%) después de tratamiento previo: una (7,1%) dilatación forzada con balón, dos (14,2%) miotomías de Heller laparoscópicas y un caso de POEM previo (7,1%). La edad media de intervención fue de 15 años (desviación estándar [DE] ± 1,9). La puntuación de Eckardt inicial fue de 7,5 (DE: ± 1,8), siendo el GERD inicial de 6 (DE: ± 2,9). Se registró una complicación posoperatoria de grado 2 de Clavien-Dindo correspondiente a una neumonía leve (7,1%). La puntuación de Eckardt y GERD posoperatorias tras 12 meses de seguimiento fueron de 0,7 (DE ± 1,2) y 0,5 (DE ± 0,7). La tasa de éxito fue superior al 93%.
ConclusionesEl abordaje endoscópico de la acalasia puede considerarse un procedimiento seguro, eficaz y podría ser de primera línea para el tratamiento de la acalasia pediátrica.
Achalasia is a rare neuromuscular disorder of the oesophagus characterised by impaired relaxation of the lower oesophageal sphincter (LOS) and decreased oesophageal peristalsis. Although as yet there is no cure for the underlying neuropathology, there are treatments for symptomatic relief of patients with achalasia.1 Management includes medical treatment, chemical, mechanical or pneumatic paralysis (forceful dilation) of the LOS, peroral endoscopic myotomy (POEM) or surgery using a minimally invasive approach involving a laparoscopic Heller myotomy (HM) with associated fundoplication.2
HM has been considered the gold standard for the treatment of oesophageal achalasia symptoms, improving efficacy and, in particular, clinical recurrence compared to endoscopic forceful dilation. Dilation therapy can also require more frequent reintervention due to recurrence of symptoms in paediatric patients. Although the safety and efficacy of HM for the surgical management of paediatric achalasia is well established in the literature, significant operative complications and long-term problems have also been described in this population. These include intraoperative oesophageal perforation, recurrent dysphagia and the need for repeat surgery or pneumatic dilation after HM.3
There is currently a worldwide trend towards minimally-invasive surgery and natural orifice transluminal endoscopic surgery (NOTES), being postulated as the next step in achalasia surgery. The POEM procedure consists of performing sphincter myotomy in a similar way to HM, but based on NOTES, that is, through the oral cavity using a gastrointestinal endoscope.4
POEM was initially described in 2008 and published in 2010 by Inoue et al. in a series of 17 adult patients with five months of follow-up. It was subsequently applied in paediatrics for the first time in 2012 and described in the literature in 2015.5–10
The success rates of POEM published in the literature appear to be similar to those of HM,11 so it is currently considered a first-line treatment option (along with HM) for the management of this disorder in the adult population.
Although there is growing experience in POEM in paediatrics, few series in this population are described in the literature. The main aim of this study was to evaluate the clinical efficacy of POEM.
Material and methodsA multicentre retrospective study was performed to evaluate outcomes in paediatric patients (aged ≤18 years) with achalasia who underwent POEM.
A multicentre POEM registry database was created in 2016 at Hospital de la Santa Creu i Sant Pau and Hospital Universitario de Navarra. This database prospectively collects demographic data on age and height, age of onset of achalasia symptoms, studies performed, achalasia classification, previous treatments, intraoperative data, preoperative and postoperative Eckardt score and GERDQ score, intraoperative and postoperative complications, success rate (clinical success score ≤3) and follow-up of patients undergoing POEM.
Objectives and variablesThe primary objective of the study was to evaluate the clinical efficacy of POEM, which was measured as Eckardt score ≤3 at three months after the intervention. Technical success was defined as the percentage of patients in whom the technique could be completed.
The secondary objectives evaluated were clinical recurrence at 12 and 24 months (Eckardt score >3), complications during the procedure or during follow-up (assessed using the Clavien-Dindo classification12), the presence of gastro-oesophageal reflux (oesophagitis in the follow-up endoscopy) and the need for treatment with a proton-pump inhibitor (PPI).
Surgical techniquePreoperative, surgical and postoperative protocols are not standardised across centres, although similar general recommendations are followed. We recommend a liquid diet the day before and fasting on the day of the procedure. However, this recommendation should be personalised based on the preparation and findings in previous endoscopies; in the event of abundant residue, the diet duration is extended to three or five days. In general, no prior admission or specific treatment is required. Endotracheal intubation is performed in the operating theatre or in the endoscopy room using a rapid induction sequence to reduce the risk of bronchoaspiration. The patient is placed prone and preoperative intravenous antibiotic prophylaxis is given with a single dose of cefazolin (40 mg/kg/dose, maximum 8 g/day). In the event of allergy to penicillin, gentamicin (5 mg/kg/dose, maximum 240 mg/day) and clindamycin (20 mg/kg/dose, maximum 3 g/day) are administered. The electrosurgery units and their parameters are adapted to the type of scalpel and are the same as those used in adult patients.
The details of performing POEM endoscopic surgery are described below with some modifications from the technique initially described by Inoue et al.6:
- 1.
Access to the oesophagus with a flexible endoscope, preferably located in the right posterior area, approximately 7–10 cm proximal to the oesophagogastric junction. Injection of normal saline with methylene blue or indigo carmine in this area (Fig. 1a).
- 2.
Mucosotomy at the injection site using a scalpel (such as a Triangle TipKnife J [Olympus Medical, Tokyo, Japan] or Splash M-knife [Pentax Medical, Tokyo, Japan]) (Fig. 1b).
- 3.
Creation of a submucosal tunnel by instillation of the normal saline solution with methylene blue and submucosal dissection with electrocoagulation. The tunnel extends 2–3 cm distal to the gastric cardia (Fig. 2a).
- 4.
Myotomy of the circular muscle fibres 2 cm from the start of the mucosotomy, that is, 5 cm from the LOS, and descending to 2 cm below the oesophagogastric junction, with a total myotomy length of 7–10 cm. It is possible to try to preserve the longitudinal muscle fibres and this could decrease the incidence of subsequent gastro-oesophageal reflux or herniation of the mucosa due to the myotomy, or increase the recovery of peristalsis (Fig. 2b).
- 5.
Closure of the oesophageal mucosa with haemostatic clips (Fig. 3).
 access to oesophageal mucosa, b) oesophageal mucosectomy.")
 creation of oesophageal submucosal tunnel, b) circular fibre myotomy.")

In the postoperative period, we do not perform imaging tests per protocol. Patients start a liquid diet 24 h after POEM, progress to a soft or liquidised diet after 48 h for two days and subsequently start introducing solids. Patients can be discharged after 24–48 h.
At each hospital, POEM was performed by the same endoscopist assisted by the paediatric surgery team. The endoscopists who performed the procedures have extensive experience in therapeutic endoscopy, including oesophageal interventions such as endoscopic mucosal resection and submucosal dissection (each having performed over 100 POEM in the adult population).
Clinical follow-up data were collected at postoperative visits at three, six, 12 and 24 months. Patient-reported outcomes were assessed by telephone calls, post or follow-up appointments. Objective assessment was planned with an oesophageal transit study one month after the procedure and a gastrointestinal endoscopy six months after the procedure.
ResultsA total of 15 POEM interventions were performed in 14 patients with achalasia at two Spanish centres, Hospital de la Santa Creu i Sant Pau in Barcelona and Hospital Universitario de Navarra in the Navarre region, between October 2016 and December 2023.
The mean age of the patients at the time of the intervention was 15 years (standard deviation [SD] = 1.9), with male prevalence and an average weight of 56 kg (SD = 13.6). Three patients had achalasia type I (21.4%) and 11 type II (78.6%) according to the Chicago classification in the high-resolution manometric study. POEM was performed as first-line therapy in 11 patients (79.7%) and after previous treatment in four (28.5%); one (7.1%) had previously been treated with pneumatic balloon dilation, two (14.2%) by laparoscopic HM and one (7.1%), ineffective POEM. Mean weight at 12 months of follow-up was 68.2 kg (SD = 10.4). The characteristics of our patients are shown in Table 1.
Baseline characteristics of the patients.
| Case | Age | Gender | Achalasia (type) | Time with symptoms (months) | Previous dilation | Previous Heller myotomy |
|---|---|---|---|---|---|---|
| 1 | 15 | Female | 2 | 18 | No | No |
| 2 | 16 | Male | 2 | 24 | No | No |
| 3 | 16 | Male | 2 | 60 | No | No |
| 4 | 16 | Male | 2 | 36 | No | Yes |
| 5 | 16 | Female | 2 | 24 | No | No |
| 6 | 17 | Female | 2 | 12 | Yes | No |
| 7 | 17 | Male | 2 | 70 | No | Yes |
| 8 | 18 | Female | 1 | 120 | No | No |
| 9 | 18 | Male | 2 | 11 | No | No |
| 10 | 12 | Male | 2 | 5 | No | No |
| 11 | 14 | Male | 1 | 6 | No | No |
| 12 | 17 | Male | 2 | 8 | No | No |
| 13 | 14 | Male | 1 | 6 | No | No |
| 14 | 12 | Male | 2 | 4 | No | No |
The baseline Eckardt score ranged from 5 to 10 (mean ± SD: 7.8 ± 1.6), with the baseline GERDQ score ranging from 1 to 10 (mean ± SD: 6.2 ± 2.8). The operating time was 41–240 min (mean ± SD: 90 ± 50.6) and no intraoperative complications were recorded.
The POEM procedure was completed in all cases (100% technical success). During the postoperative period, one complication was recorded; a case of mild pneumonia (7.1%), which resolved with oral antibiotic therapy (Clavien-Dindo grade 2). Mean hospital stay was four days (mean ± SD: 4.2 ± 3.9), with a mean follow-up of 28.6 months (SD ± 16.9). During follow-up, clinical improvement was found in all patients, with Eckardt score ≤3 showing clinical efficacy at three months in 13 patients (93%). One patient showed partial clinical improvement (Eckardt score of 4 with previous score of 10) three months after POEM and so a second POEM was performed. After reintervention, the patient’s Eckardt score was 0 during follow-up (12 months).
Gastroscopy at the six-month follow-up, with or without single-dose PPI depending on the patient’s clinical condition, showed grade A oesophagitis in one patient (7.1%). In six (42.8%) the PPI was continued at a single dose after endoscopic follow-up.
Follow-up was 38.9 months (mean ± SD: 38.9 ± 23.4). Postoperative Eckardt and GERDQ scores after 12 months of follow-up were 0.7 (SD ± 1.2) and 0.5 (SD ± 0.7), respectively. After 24 months of follow-up, the postoperative Eckardt and GERDQ scores were 1.1 (SD ± 1.6) and 0.5 (SD ± 0.8), respectively, with no clinical recurrence noted.
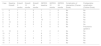
Table 2 shows the different preoperative variables (at diagnosis) and postoperative variables (at 12 months of follow-up) after performing POEM.
Pre-POEM and post-POEM characteristics.
| Case | Baseline Eckardt | Eckardt 3 months | Eckardt 12 months | Eckardt 24 months | GERDQ baseline | GERDQ 12 months | GERDQ 24 months | Complication of intervention (Clavien-Dindo) | Postoperative complication (Clavien-Dindo) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 6 | 1 | 1 | 0 | 7 | 1 | 0 | No | No |
| 2 | 7 | 0 | 0 | 0 | 1 | 0 | 0 | No | No |
| 3 | 8 | 0 | 0 | 0 | 3 | 0 | 0 | No | No |
| 4 | 9 | 0 | 0 | 0 | 9 | 1 | 0 | No | No |
| 5 | 8 | 1 | 1 | 1 | 10 | 1 | 1 | No | No |
| 6 | 10 | 0 | 0 | 0 | 4 | 0 | 0 | No | No |
| 7 | 5 | 0 | 0 | 0 | 5 | 0 | 0 | No | No |
| 8 | 8 | 0 | 0 | – | 6 | 0 | 0 | No | Pneumonia (grade 2) |
| 9 | 10 | 4 | 4 | 4 | 7 | 2 | 2 | No | No |
| 10 | 6 | 3 | 1 | – | 8 | 0 | – | No | No |
| 11 | 7 | 0 | 0 | – | 8 | 0 | – | No | No |
| 12 | 9 | 3 | 2 | 2 | 6 | 1 | – | No | No |
| 13 | 9 | 0 | 0 | – | 6 | 0 | – | No | No |
| 14 | 7 | 0 | 0 | – | 8 | 2 | – | No | No |
POEM: peroral endoscopic myotomy.
In this article, we have shown POEM to be an effective technique in paediatric achalasia, both as a first-line and secondary treatment, with rapid recovery and symptom relief immediately after the procedure and in the long term.
The most used surgical procedure for the treatment of achalasia is currently laparoscopic HM combined with an anti-reflux technique. However, this trend is currently changing in the adult population, with use of the POEM approach growing exponentially.
In our series, clinical efficacy with a single POEM was greater than 90%, similar to that of HM and to other published reports in the paediatric population. In one patient (7.1%) it was decided to perform a repeat POEM, due to a persistent Eckardt score of 4 (previously 10) after three years of follow-up. After the procedure, the clinical efficacy of POEM reached 100% during follow-up. There are very few articles on paediatric POEM, but we have been able to find the first meta-analyses reporting similar results. Success rates (Eckardt ≤3) in the region of 89%–92% are described, while in our case, it was 93% with a single POEM; a six-point decrease in the Eckardt score is described after the procedure, while in our series, we found a decrease of seven points.13,14 In terms of clinical improvement in patients with POEM, the results are in excess of 90%, and reached 100% in our patients.15
The recurrence rates described in the paediatric population at five years are 8.1%–20%, compared to 22%–39% in paediatric laparoscopic HM.14–16 In our series, there were no cases of recurrence after an average of more than two years of follow-up.
With regard to PPI, there are reports in the literature of PPI use after POEM at the discretion of the treating doctor or until gastro-oesophageal reflux (GOR) is ruled out.16 In our series, PPI was administered at 20 mg (<20 kg = 10 mg/day, ≥20 kg = 20 mg/day) in a single daily dose for one month to ensure proper closure of the mucosal incision. Thereafter, it is prescribed based on the patient’s reflux symptoms. In six patients (42.8%) single-dose PPI was maintained after endoscopic follow-up, with adequate control of symptoms and oesophagitis. There are reports in the literature of reflux oesophagitis (6%–42%), recurrence (2.7%–8%) and GOR (8.1%–28%) after POEM. Other less common complications have been described, such as ulcer of the oesophagogastric junction, oesophageal perforation and mucosal tear.17–19 We cannot objectively assess gastro-oesophageal reflux using pH monitoring, as we frequently encounter family members failing to perform further follow-up pH monitoring after the obvious clinical improvement following POEM. This problem has recently been described in the literature and means the results in the study of gastro-oesophageal reflux are not consistent or comparable with other techniques such as HM,20,21 where reflux is found in 9% of paediatric patients who have pH monitoring after the laparoscopic intervention. It is important to maintain long-term follow-up of patients, in order to detect the development of GOR and assess the need for treatment in case patients develop erosive oesophagitis.
We have to highlight the importance of a multidisciplinary team with an expert in therapeutic gastrointestinal endoscopy and POEM alongside a paediatric surgery team, in order to enable the learning curve to be completed in paediatrics and ensure comprehensive patient management. In our series we have noted a shortening of the operating time and hospital stay since we introduced paediatric POEM, to the extent that the last procedure was completed in 40 min and for the last two cases, the hospital stay was only 24 h. These findings are consistent with descriptions of the POEM learning curve in adults.22
In both hospitals, the procedures were always performed by the same endoscopist, each with extensive training and having performed more than 100 POEM in the adult population to date. When adapting the procedure to the paediatric population, multidisciplinary assistance with a paediatric surgery team seems necessary to ensure comprehensive treatment of the patient and reduce possible complications.
With regard to the instruments required, we used the hybrid scalpel from the start, as its benefits have been reported in enabling injections of a solution with dye to elevate the submucosal plane and, at the same time, perform electrocoagulation without the need to change the instrument through the working channel of the flexible endoscope. This allows for shorter operating times and improved uninterrupted perception of the procedure.23 In our case, the gastroscope used was a high-definition Olympus GIF-HQ190 (Olympus Medical, Tokyo, Japan) with a 2.8-mm working channel and 9.9-mm diameter, and the scalpels used were the Triangle TipKnife J and the Splash M-knife.
Three of the patients in the series had undergone previous treatments: dilation in one case and HM in the remaining two. The patient who had undergone previous dilations had oesophageal fibrosis, which made the technique difficult and slow, but it was completed without complications. Therefore, as has been described in other series, POEM may be an appropriate option both as a first-line treatment and after previous treatments.
In our series, there was one case of postoperative pneumonia, corresponding to a grade II complication on the Clavien-Dindo scale.12 Pneumonia is the most common complication after endotracheal intubation in patients with achalasia. Despite fasting, food residue should always be suspected in any patient with achalasia. It has been reported that despite fasting, only 52% of patients with achalasia who undergo surgery have a completely empty oesophagus at the start of the procedure.4
This study has certain limitations. This is the initial experience across Spain, although we only found paediatric patients at two hospital centres. The series has few patients, with a limited follow-up time of 28.6 months (mean ± SD: 28.6 ± 16.9).
Nevertheless, based on the preliminary results of our series and those reported in the literature in the paediatric population, we believe that POEM is a promising technique in the treatment of paediatric achalasia.
ConclusionsThe endoscopic approach to paediatric achalasia appears to be a safe and effective procedure performed by a multidisciplinary team with experience in POEM. It allows for a short, painless postoperative period, with early reintroduction of diet, and can be considered as first-line treatment for paediatric achalasia. Prospective studies with larger sample sizes are needed to identify not only possible future complications not detected in this study, but also the durability of the POEM response compared to other treatment modalities for achalasia in paediatrics, and the presence of gastro-oesophageal reflux.
FundingNo funding was received for the preparation of this article.
Manuscript presented at the 60th Congress of the Sociedad Española de Cirugía Pediátrica [Spanish Society of Paediatric Surgery] in May 2023 and at the 45th Congress of the Sociedad Española de Endoscopia Digestiva [Spanish Society of Gastrointestinal Endoscopy] in November 2023.
