




The authors describe the case of a 78-year-old patient who presented with melena for 48h. No abdominal pain or other symptoms were recalled. The patient had obesity (body mass index of 33kg/m2), arterial hypertension, type 2 diabetes mellitus and stage 3 chronic kidney disease; there were no smoking or drinking habits. The patient had been extensively studied 4 years earlier due to thrombocytopenia and splenomegaly, whose etiology remained undefined. Indeed, advanced liver fibrosis had been excluded (liver parameters were sustainedly normal, no radiological signs of cirrhosis neither endoscopic signs of portal hypertension (PH) were found, mean transient elastography-measured liver stiffness was 9.2kPa [interquartile range 0.4]); two bone marrow biopsies were under the normality. The patient was under anti-hypertensive and oral hypoglycemic drugs, daily ferrous sulphate, and erythropoietin every two weeks. At admission, the physical examination was normal, except for periumbilical ecchymosis with onset in the prior 24h (Fig. 1A1). Laboratory tests showed normocytic and normochromic anemia (hemoglobin 9.7g/dL), leukocytosis (27.2×103/μL), thrombocytopenia (100×103/μL) and a mildly deranged coagulation (international normalized ratio 1.4). The liver panel and C-reactive protein were normal. Considering the suspicion of upper gastrointestinal bleeding, an esophagogastroscopy was performed (Fig. 1A2–4). Large esophageal varices with a «white nipple sign» were identified and promptly banded. To exclude the presence of any concomitant illness that could associate with the Cullen's sign and justify the presence of leukocytosis (even more considering that the patient had chronic leukopenia), an abdominopelvic computed tomography scan with contrast was performed. It revealed a cirrhotic liver, identified esophagogastric and retroperitoneal varices and signs of splenorenal shunt; the pancreas and the remaining organs were normal, and no active bleeding was detected. The patient remained asymptomatic and hemodynamically stable, presented no additional blood losses and leukocytosis remitted.
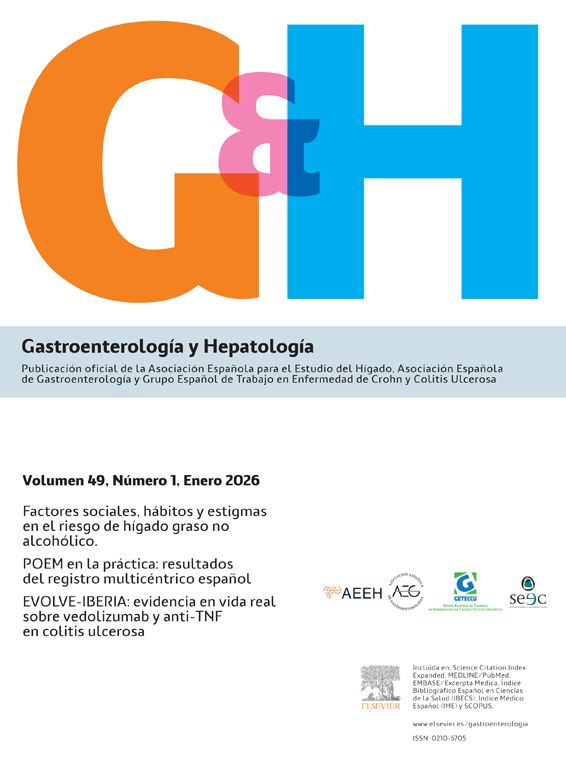
![Inspection of the abdomen (A1) and endoscopic views of the esophagus (large esophageal varices [A2], white nipple sign [A3], band ligation [A4]).](https://static.elsevier.es/multimedia/02105705/0000004600000004/v2_202304070008/S0210570522002515/v2_202304070008/en/main.assets/gr1.jpeg?xkr=ue/ImdikoIMrsJoerZ+w997EogCnBdOOD93cPFbanNcRcp7AE8pxI7/lU7i5mKGl6o67DY/uL2+/IxZemV5MIt94lf47/W9KTDkgv0tKPeV3u5+thF5l4tGoVZXDxvqhFOfx1yG7J5UV7bFs1k9b4p0G8FKbCOf1+q0uaXdq+4CarC86T6Sgx3xjP9He/Z8ORhhtm90tgUttPrKne8pxm6vFIwc8mcNldwwdu3ZZi3khNzePjxBCsj3Uh2gqq+Zg9zSm8DUhRcR4zR9LTnYwl9QzlUaT1DPyhRIpsyj9OYQ= "Inspection of the abdomen (A1) and endoscopic views of the esophagus (large esophageal varices [A2], white nipple sign [A3], band ligation [A4]).")
The bruising surrounding the umbilicus corresponds to the Cullen's sign. This sign was first described more than 100 years ago, in the setting of a ruptured ectopic pregnancy. Since then, it has been reported to occur in several clinical scenarios, including pancreatitis (the most common, appearing in 3.0–5.0% of the acute pancreatitis cases), splenic injury, perforated duodenal ulcer, acute pyelonephritis, as a manifestation of intraabdominal metastasis, among others.1,2 The common ground is that all these may course with retroperitoneal bleeding, being hypothesized that blood then spreads to the periumbilical fatty tissue through the round ligament of liver which forms part of the free edge of the falciform ligament.1 This is the second report of Cullen's sign associated with PH,3 and the first in a patient with acute variceal bleeding and without a prior diagnosis of cirrhosis. This case highlights the large interindividual heterogeneity of metabolic-associated fatty liver disease (MAFLD), and the importance of developing tools to identify the «rapid progressors», as up to one fifth of the patients without significant fibrosis may develop F3/F4 fibrosis over 5 years,4 with undeniable increase in morbidity and mortality. In addition, it must be acknowledged that, in MAFLD, PH may be present even in the absence of fibrosis, and that PH-related complications may occur with lower portal pressure gradients, when compared to other etiologies.5
Authors’ contributionsAll authors were involved in patients’ management and approved the final version of the manuscript.
FundingThis study did not receive funding.
Conflicts of interestThe authors have no conflict of interests to disclose.

