





Gallstone ileus is an unusual complication of cholelithiasis, occurring in <0.5%. It is responsible for 1–4% of cases of mechanical obstruction.1 Bouveret's syndrome is an uncommon form of gallstone ileus, first described in 1896 by Leon Bouveret,2 comprising 1–3% of cases.3
A 90-year-old man presented with a 2-day history of abdominal pain and postprandial vomiting. Laboratory investigations revealed leukocytes 18.7×103μL, reactive C protein 14mg/dL, bilirubin 2.61mg/dL, aspartate aminotransferase 96U/L, alanine aminotransferase 96U/L, alkaline phosphatase 310U/L and gamma-glutamyl transferase 528U/L. Abdominal ultrasound showed pneumobilia, dilated common bile duct (CBD) and scleroatrophic gallbladder with cholelithiasis.
He presented a high likelihood of choledocholithiasis based on clinical predictors and was referred to endoscopic retrograde cholangiopancreatography (ERCP), which was unsuccessful due to gastric stasis bulky, not identifying the pylorus. To exclude gastroduodenal obstruction, he performed an upper gastrointestinal endoscopy revealing an impacted gallstone at pylorus that was successfully treated with endoscopic extraction combined with mechanical lithotripsy. A fistulous stoma was visualized on the duodenal bulb (Fig. 1). ERCP demonstrated a dilated CBD filled with multiple gallstones and confirmed cholecystoduodenal fistula (Fig. 2). Endoscopic sphincterotomy was performed being the CBD explored with biliary balloon and Dormia basket. Following the procedure CBD had no residual stones, presenting good drainage of contrast. The planned conservative treatment was successful and the patient was discharged 15 days later.
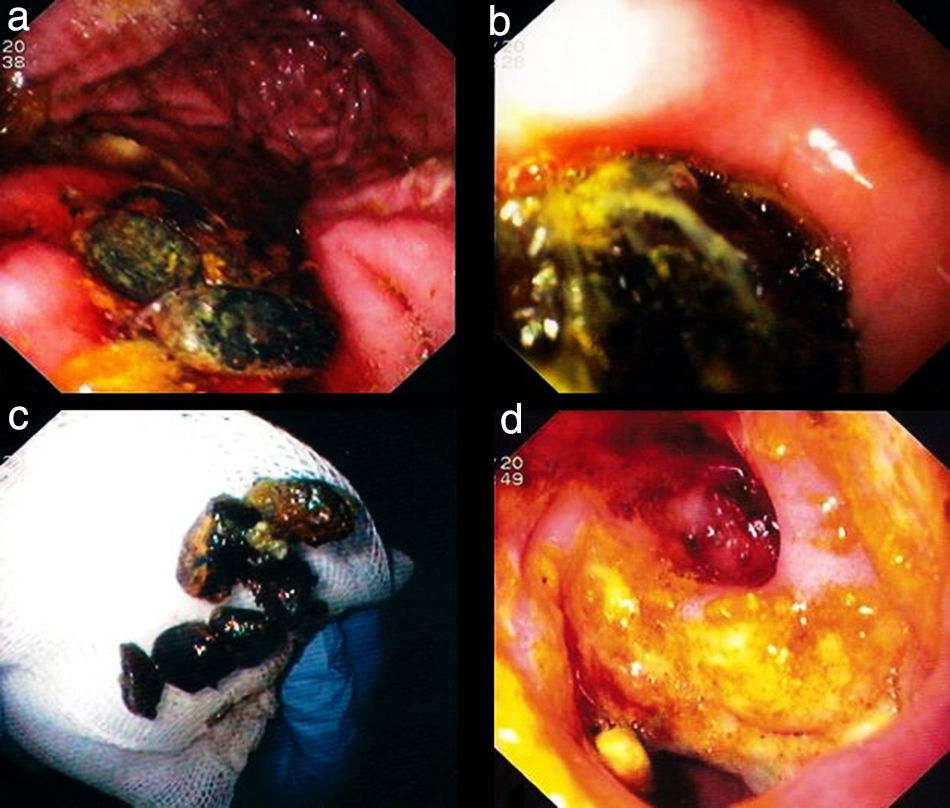
 and an impacted gallstone at pylorus (image b). Retrieved gallstones after mechanical lithotripsy with snare and Dormia basket (image c). Endoscopic view of the duodenal bulb: fistulous stoma with surrounding duodenal bulb mucosa extensively ulcerated (image d).")
Upper gastrointestinal endoscopy showing gallstones in the gastric corpus (image a) and an impacted gallstone at pylorus (image b). Retrieved gallstones after mechanical lithotripsy with snare and Dormia basket (image c). Endoscopic view of the duodenal bulb: fistulous stoma with surrounding duodenal bulb mucosa extensively ulcerated (image d).
. A 14mm dilated CBD filled with multiple gallstones, a scleroatrophic gallbladder with cholelithiasis and a patent cystic duct (image b and c). Cholecystoduodenal fistula was confirmed after contrast injection (image c).")
Endoscopic retrograde cholangiopancreatography. Plain abdominal radiograph before contrast injection showing pneumobilia and air route from gallbladder to duodenum topography, suggestive of biliary enteric fistula (image a). A 14mm dilated CBD filled with multiple gallstones, a scleroatrophic gallbladder with cholelithiasis and a patent cystic duct (image b and c). Cholecystoduodenal fistula was confirmed after contrast injection (image c).
Bouveret's syndrome is defined as gastric outlet obstruction secondary to an impacted gallstone in the duodenum or pylorus, which enter into the bowel through a biliary enteric fistula. Endoscopy made the diagnosis in nearly all cases, identifying the obstructing gallstone in 69%. Endoscopic treatment should be considered a first-line option, because of low morbidity and negligible mortality.4 Fistula repair is considered unnecessary due to spontaneous closure, especially when the cystic duct is patent.5

