



Identificar los factores asociados a mortalidad intrahospitalaria, estimar la tasa de intubación y describir la mortalidad intrahospitalaria de mayores de 65 años que requirieron ventilación mecánica invasiva (VMI) en el servicio de urgencias.
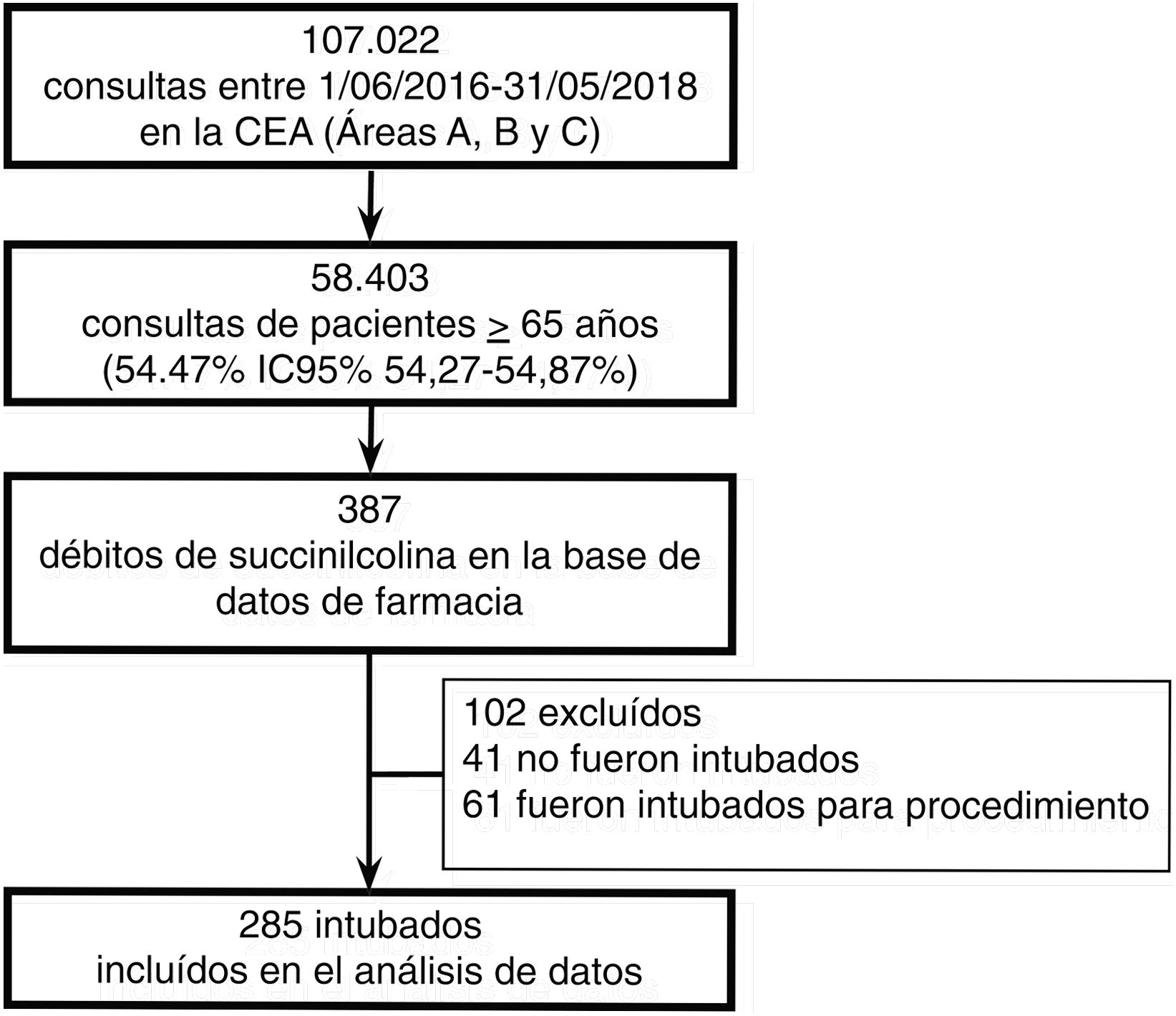
MétodosEstudio de cohorte retrospectiva con pacientes mayores de 65 años, intubados en la central de emergencias del adulto entre 2016 y 2018 en un hospital de alta complejidad. Se consignaron datos demográficos, comorbilidades y scores de severidad al ingreso. Se realizaron análisis bivariado y multivariado con regresión logística en relación a mortalidad hospitalaria y posibles confundidores.
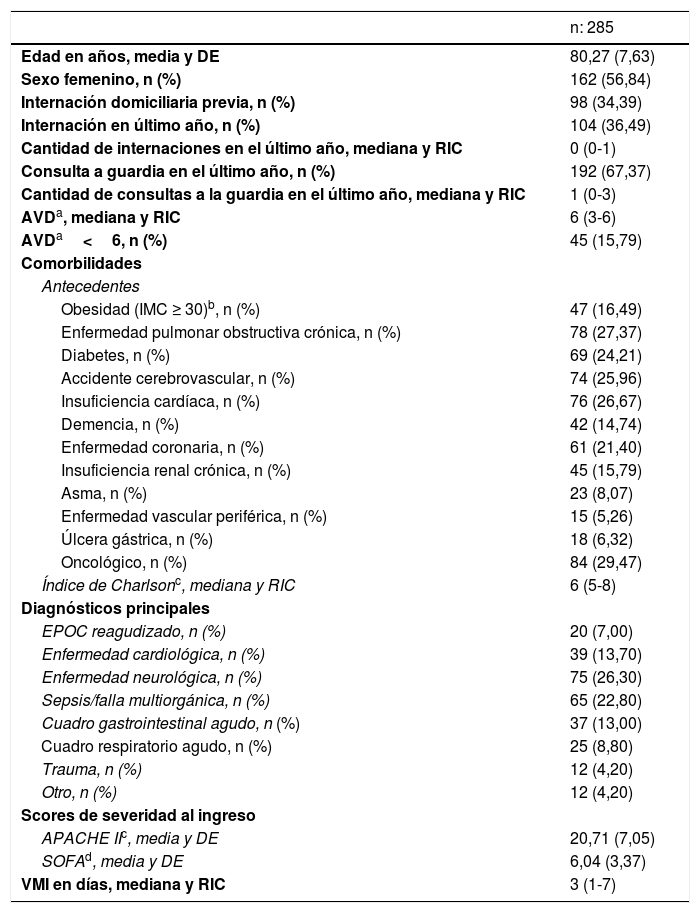
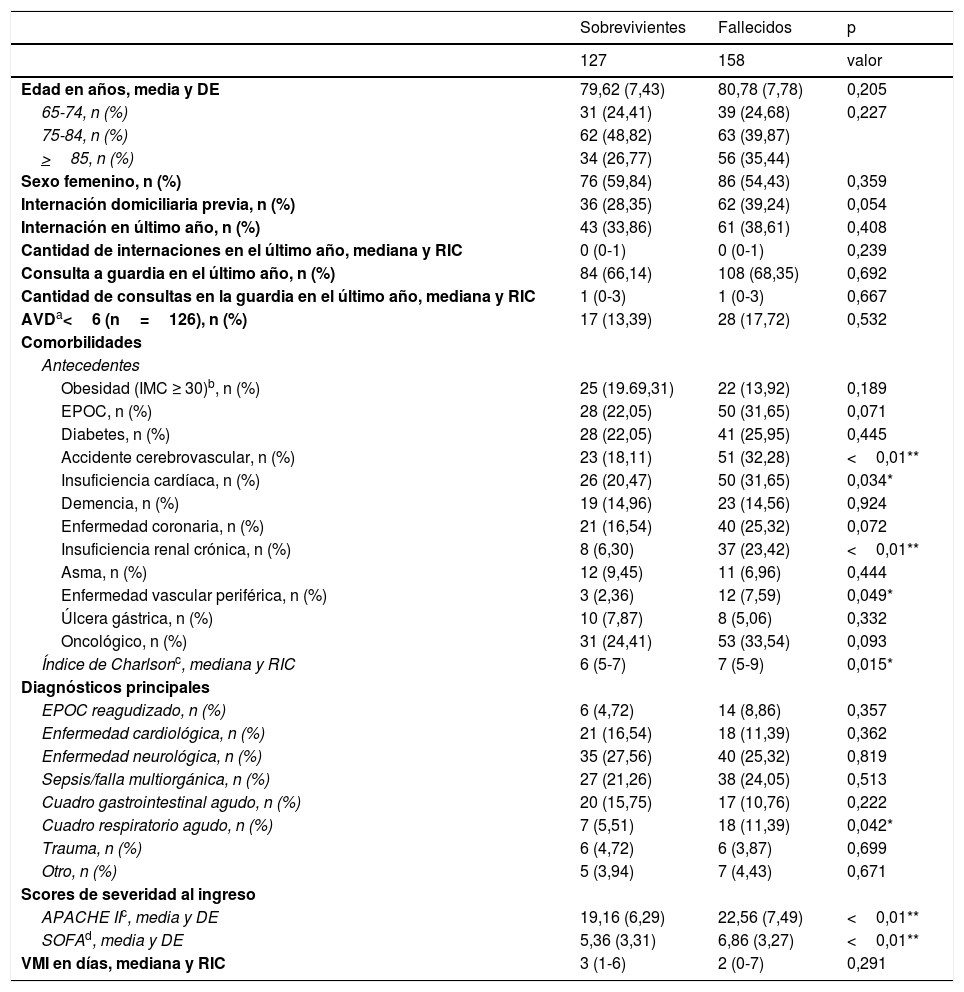
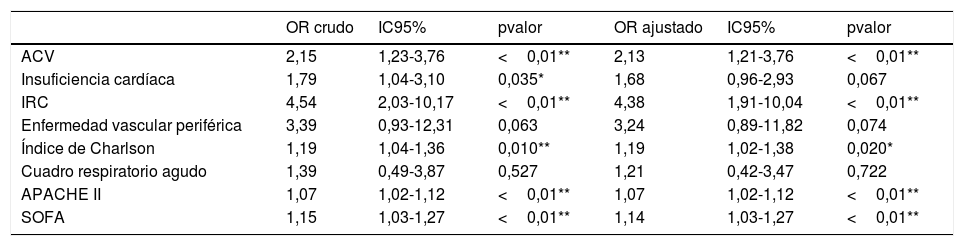
ResultadosUn total de 285 pacientes con media de 80 años requirieron VMI en urgencias durante una mediana de 3 días, y con media de 20 puntos de severidad según APACHE II. La tasa de VMI resultó 0,48% (IC95% 0,43-0,54), y 55,44% (158) fallecieron. Los factores asociados a mortalidad tras el ajuste por edad y sexo fueron: accidente cerebrovascular (OR 2,13; IC95%1,21-3,76), insuficiencia renal crónica (OR 4,38; IC95%1,91-10,04), índice de Charlson (OR 1,19; IC95%1,02-1,38), APACHE II (OR 1,07; IC95%1,02-1,12) y SOFA (OR 1,14; IC95%1,03-1,27).
DiscusiónNuestra tasa de VMI fue inferior a la declarada por Johnson et al. en Estados Unidos en 2018 (0,59%). La mortalidad intrahospitalaria de nuestro estudio superó la predicha por el score de APACHE II (40%) y de SOFA (33%), sin embargo fue consistente con la reportada por Lieberman et al. en Israel y Esteban et al. en Estados Unidos.
ConclusionesSi bien la tasa de requerimiento de VMI en el servicio de emergencias fue baja, más de la mitad fallecieron durante su hospitalización. Las enfermedades cerebrovasculares y renales preexistentes y los altos puntajes en el índice de comorbilidades y en los scores de gravedad al ingreso fueron predictores independientes para mortalidad intrahospitalaria.
To identify factors associated with in-hospital mortality, to estimate the intubation rate and to describe in-hospital mortality in patients over 65 years old with invasive mechanical ventilation (IMV) in the emergency department (ED).
MethodsRetrospective cohort study of patients over 65 years old, who were intubated in an ED of a high complexity hospital between 2016 and 2018. Demographic data, comorbidities, and severity scores on admission were described. Bivariate and multivariate analyses were performed with logistic regression according to mortality and possible confounders.
ResultsA total of 285 patients with a mean age of 80 years required IMV in the emergency department, for a median of 3 days, and with a mean APACHE II score of 20 points of severity. The IMV rate was .48% (95% CI .43-.54), and 55.44% (158) died. Mortality-associated factors after age and sex adjustment were stroke (OR 2.13; 95%CI 1.21-3.76), chronic kidney failure, (OR 4.,38; 95%CI 1.91-10.04), Charlson index (OR 1.19; 95%CI 1.02-1.38), APACHE II score (OR 1.07; 95%CI 1.02-1.12), and SOFA score (OR 1.14; 95%CI 1.03-1.27).
DiscussionOur IMV rate was lower than that stated by Johnson et al. in the United States in 2018 (.59%). In-hospital mortality in our study exceeded that predicted by the APACHE II score (40%) and SOFA (33%). However it was consistent with that reported by Lieberman et al. in Israel and Esteban et al. in the United States.
ConclusionsAlthough the IMV rate was low in the ED, more than half the patients died during hospitalization. Pre-existing cerebrovascular and renal diseases and high results in the comorbidities index and severity scores on admission were independent factors associated with in-hospital mortality.
Artículo
Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora

