




Bacteremia caused by Staphylococcus aureus is a significant entity due to its frequency and severity. The epidemiology of the strains that cause these invasive infections, both methicillin-sensitive Staphylococcus aureus (MSSA) and methicillin-resistant Staphylococcus aureus (MRSA), varies by region and by country.1
MRSA clonal complex 398 (CC398) strains, which are usually epidemiologically linked to swine raised as livestock are often detected in Spain.2 There are limited data on the MSSA CC398 variant, but they are considered an emerging entity in countries such as France3–5 and Portugal.6
To determine the significance of these strains in invasive infections in our setting, we analyzed S. aureus isolates (first isolate/patient) from blood cultures at Hospital Royo Villanova (HRV) in Zaragoza, Spain, over a 30-month period (01/06/2015–31/12/2017). A total of 84 S. aureus isolates (30 MRSA and 54 MSSA) were obtained; of these, 77 (27 MRSA [all mecA-positive] and 50 MSSA) could be recovered and were included in this study.
We determined the sensitivity to antimicrobial agents of the 77 S. aureus strains (Combo 31, MicroScan®, Beckman, and agar diffusion panels) and determined whether the strains belonged to the CC398 lineage by PCR.7 In the latter (CC398), we analyzed the presence of genes for antibiotic resistance by phenotype of resistance detected (blaZ, erm(A), erm(B), erm(C), erm(T), or msr(A)).8 We also studied genes for macrolide resistance in the S. aureus isolates from non-CC398 lineages in order to compare them to those from the CC398 lineage.
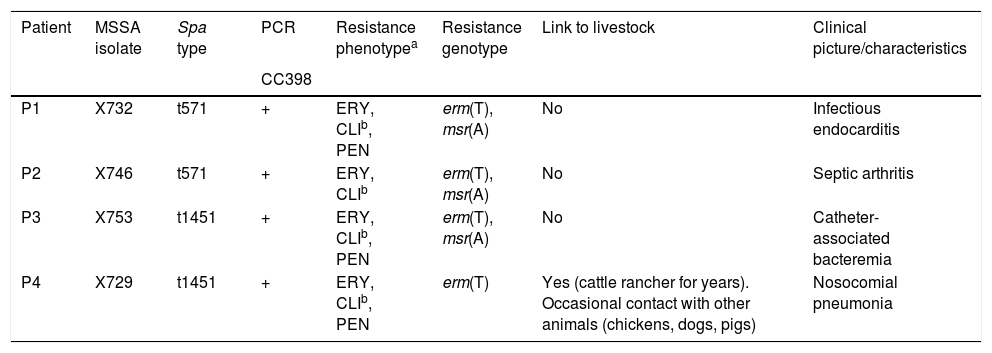
A total of 4 CC398 isolates, all MSSA, were detected, amounting to 8% of the MSSA strains and 5.2% of all S. aureus strains. They were ascribed to 2 different spa types: t571 and t1451 (Table 1). No MRSA was associated with CC398 (all were sensitive to tetracycline). The 4 MSSA CC398 isolates lacked the tetracycline-resistant phenotype (marker of MRSA CC398) and all had (inducible) resistance to erythromycin and to clindamycin, said resistance being mediated by the unusual erm(T) gene, which in 3 strains coexisted with the msr(A) gene (Table 1). Of the non-CC398 isolates, 12 (16.4%) had (inducible) resistance to erythromycin and clindamycin, said resistance being mediated by the erm(A) gene or the erm(B) gene, detected along with the msr(A) gene in 9 of them. The erm(T) gene was not found in non-CC398 S. aureus. Therefore, (inducible) resistance to erythromycin/clindamycin mediated by the erm(T) gene may be a phenotypic marker for MSSA CC398, consistent with other series,3,9 unlike resistance to tetracycline, which is characteristic of MRSA CC398. The 4 MSSA CC398 isolates were sensitive to all other antibiotics, with the sole exception of penicillin, whereas the MSSA non-CC398 isolates were also resistant to ciprofloxacin (n = 32), aminoglycosides (n = 16), mupirocin (n = 14) and/or cotrimoxazole (n = 1).
Characteristics of MSSA CC398 isolates from blood cultures.
| Patient | MSSA isolate | Spa type | PCR | Resistance phenotypea | Resistance genotype | Link to livestock | Clinical picture/characteristics |
|---|---|---|---|---|---|---|---|
| CC398 | |||||||
| P1 | X732 | t571 | + | ERY, CLIb, PEN | erm(T), msr(A) | No | Infectious endocarditis |
| P2 | X746 | t571 | + | ERY, CLIb | erm(T), msr(A) | No | Septic arthritis |
| P3 | X753 | t1451 | + | ERY, CLIb, PEN | erm(T), msr(A) | No | Catheter-associated bacteremia |
| P4 | X729 | t1451 | + | ERY, CLIb, PEN | erm(T) | Yes (cattle rancher for years). Occasional contact with other animals (chickens, dogs, pigs) | Nosocomial pneumonia |
PCR: polymerase chain reaction; MSSA: methicillin-sensitive Staphylococcus aureus.
CC398 is an emerging lineage among invasive MSSA strains accounting for 8% of these strains at our hospital. In France it has been detected with a frequency that is variable but has been growing in recent years,3 with figures as high as 20% in a 2017 series.4 In addition to its presence in cases of bacteremia, cases of it as a cause of other serious infections such as pneumonia, endocarditis and joint infections have been reported in France9; this is consistent with our small series. One of the spa types detected in our study is t571, which is linked to infections of nosocomial or healthcare-related origin without any link to livestock, and which is gaining prominence in countries near Spain such as France and Portugal.3,5,6 More subject to debate is the epidemiology of t1451, and although in two of the cases presented a prior professional link to livestock was found, more studies are needed to arrive at valid conclusions.
The dispersion of these strains is concerning due to both their increasing frequency in geographic settings near Spain and their association with greater virulence and serious infections.3–5,9,10
The study, despite its limited number of cases, seems to point to the presence of CC398 among invasive MSSA isolates. It would be useful to extend the study to other hospitals and other epidemiological settings in order to acquire more complete knowledge of the emerging MSSA CC398 lineage.
FundingStudy funded by project SAF2016-76571-R of the Spanish State Research Agency (AEI) and by the European Regional Development Fund (ERDF) of the EU.
Conflicts of interestO.M. Mama has a predoctoral Women-for-Africa grant from the Universidad de La Rioja (UR) and L. Ruiz-Ripa has a predoctoral grant from the UR. The authors declare that they have no conflicts of interest.
Please cite this article as: Mama OM, Aspiroz C, Ruiz-Ripa L, Torres C. Importancia del complejo clonal CC398 en las bacteriemias por Staphylococcus aureus en un hospital secundario de Aragón. Enferm Infecc Microbiol Clin. 2020;38:394–395.
This study was presented at the 23rd National Conference of the Spanish Association for Infectious Diseases and Clinical Microbiology (SEIMC) in Madrid, Spain, on 23-25 May 2019.
- Comparative severity of COVID-19 cases caused by Alpha, Delta or Omicron SARS-CoV-2 variants and its association with vaccination
- Mild SARS-CoV-2 infection in vulnerable patients: implementation of a clinical pathway for early treatment
- Impact on tuberculosis diagnostic during COVID-19 pandemic in a tertiary care hospital
- Secondary syphilis mimicking systemic rheumatic disease: Report of 2 cases

Enfermedades Infecciosas y Microbiología Clínica (English Edition) follows the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals