




Enteroviruses are a family of viruses that predominantly infect the paediatric population, with non-specific clinical manifestations occurring in many cases. Infections generally present as flare-ups during the summer months, or as sporadic cases throughout the year. The main clinical manifestations are meningitis, self-limited febrile syndromes, exanthema, diarrhoea and neuromuscular diseases,1,2 although there are very few data on their involvement in acute respiratory infections (ARIs).
Some studies seem to indicate that they may be the leading viruses that cause these infections during the winter months.3,4 As such, we conducted a prospective study on their detection in these diseases. During the period between July 2015 and March 2016, we performed a prospective study on the presence of enterovirus in respiratory samples from all paediatric patients (<15 years of age) admitted to the Emergency Department with a suspected ARI. Clinical diagnoses were made based on the patients’ symptoms and chest X-rays,3,4 while viral detection was performed using a commercially available real-time RT-PCR gene amplification technique (Allplex® Respiratory Full Panel Assay; Seegene, South Korea). This technique differentiates between enterovirus and rhinovirus, but cannot serotype different enteroviruses. The enterovirus-positive samples were sent to the National Microbiology Centre of Madrid, where the final serotyping was performed.
2827 samples were analysed over the course of the study, of which 1646 (58.2%) tested positive. Of these, 98 (5.9%) corresponded to enterovirus and only 80 strains could be serotyped (81.6%). These 80 cases amount to 4.8% of the positive samples and 2.8% of the total samples analysed.
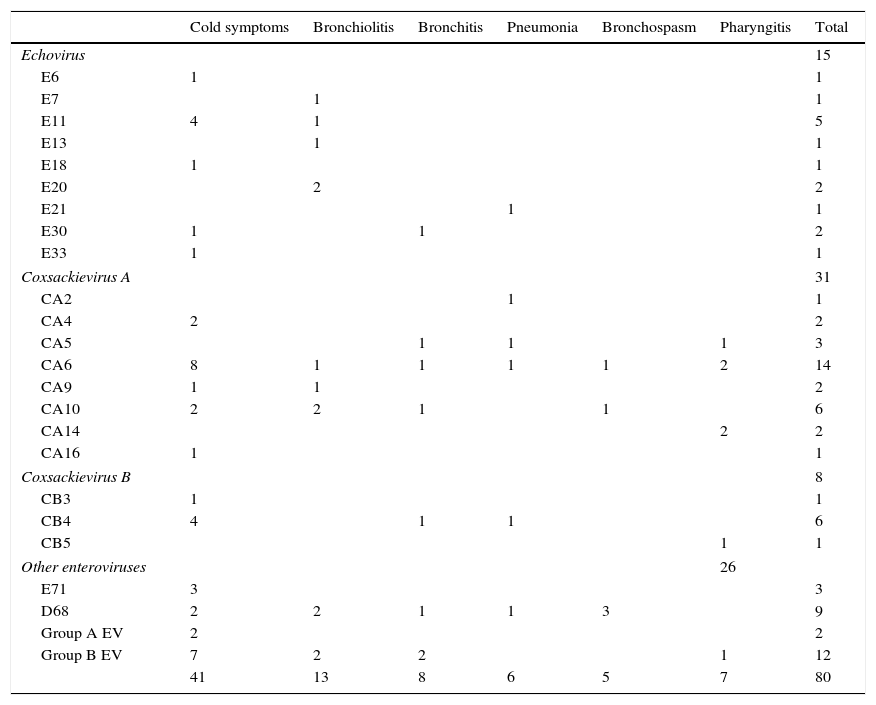
Serotyping showed that 18.7% were Echovirus, 38.7% Coxsackievirus A, 10% Coxsackievirus B and 32.5% other enteroviruses (Table 1). The most commonly detected types were: Coxsackievirus A6 (17.5%), enterovirus group B (15%) and EV-D68 (11.2%). Among the Echoviruses, type E11 was most common (33.3%); of the group A and B coxsackieviruses, A6 (19.3%) and B4 (50%) were the most prevalent. Moreover, in 7 cases (8.7%), co-infections with other viruses were detected, predominantly rhinovirus.
Main respiratory infections caused by different types of enterovirus.
| Cold symptoms | Bronchiolitis | Bronchitis | Pneumonia | Bronchospasm | Pharyngitis | Total | |
|---|---|---|---|---|---|---|---|
| Echovirus | 15 | ||||||
| E6 | 1 | 1 | |||||
| E7 | 1 | 1 | |||||
| E11 | 4 | 1 | 5 | ||||
| E13 | 1 | 1 | |||||
| E18 | 1 | 1 | |||||
| E20 | 2 | 2 | |||||
| E21 | 1 | 1 | |||||
| E30 | 1 | 1 | 2 | ||||
| E33 | 1 | 1 | |||||
| Coxsackievirus A | 31 | ||||||
| CA2 | 1 | 1 | |||||
| CA4 | 2 | 2 | |||||
| CA5 | 1 | 1 | 1 | 3 | |||
| CA6 | 8 | 1 | 1 | 1 | 1 | 2 | 14 |
| CA9 | 1 | 1 | 2 | ||||
| CA10 | 2 | 2 | 1 | 1 | 6 | ||
| CA14 | 2 | 2 | |||||
| CA16 | 1 | 1 | |||||
| Coxsackievirus B | 8 | ||||||
| CB3 | 1 | 1 | |||||
| CB4 | 4 | 1 | 1 | 6 | |||
| CB5 | 1 | 1 | |||||
| Other enteroviruses | 26 | ||||||
| E71 | 3 | 3 | |||||
| D68 | 2 | 2 | 1 | 1 | 3 | 9 | |
| Group A EV | 2 | 2 | |||||
| Group B EV | 7 | 2 | 2 | 1 | 12 | ||
| 41 | 13 | 8 | 6 | 5 | 7 | 80 | |
The aforementioned 80 patients comprised 63 boys (78.7%) and 17 girls (21.3%), the mean age of whom was 2.2 years (range: 6 days to 9 years). The majority of cases were detected between the months of November and February, and the main related conditions were: cold symptoms (51.2%), bronchiolitis (16.2%), bronchitis (10%), pharyngitis (8.2%), pneumonia (7.5%) and bronchospasm (6.2%).
Among those with cold symptoms, Coxsackievirus A was detected in 34.1%, Echovirus in 19.5% and group B EV in 17%. In the patients with bronchiolitis, Echovirus and Coxsackievirus A accounted for 38.4% and 30.7%, respectively, while the main virus involved in the bronchitis cases was Coxsackievirus A (37.5%). Of the 6 pneumonia cases, 50% were triggered by Coxsackievirus A, while EV-D68 was the most common type amongst patients with bronchospasm (60%). As for pharyngitis, Coxsackievirus A was behind 71.4% of cases.
10 of the patients (12.5%) required hospitalisation, although none was admitted to the ICU. The main diseases endured by these patients were pneumonia (40%), bronchospasm (40%) and bronchiolitis (20%). No patients died as a result or complication of an enterovirus infection. A history of asthma was the main factor associated with this type of infection. Of the 8 cases (10%), 3 (37.5%) were associated with EV-D68.
The involvement of enteroviruses in ARIs seems to depend on the time of year under analysis and the socio-sanitary conditions of the country in question. Accordingly, annual rates of 4–15%5–7 have been reported, which is very similar to the 4.8% found in our study.
As regards the type of enterovirus involved, the absence of a predominant type seems to have been demonstrated.2,8,9 The most commonly involved forms were Coxsackieviruses A9 and A16, Coxsackieviruses B1-6 and Echoviruses 2, 4, 6 and 11.8 In one study by Trallero et al.,10Echoviruses 6 (17%) and 11 (10%) were proven to be the most common forms in ARIs. In our study, we detected 23 different types of enterovirus, thus confirming its heterogeneity.
Enterovirus-related ARIs predominantly affect children under 5 years of age1,2,5 and particularly those younger than 12 months, with bronchiolitis symptoms occurring frequently.5,7 Our patients had a mean age of 2.2 years and bronchiolitis was the second most-common disease, although non-specific cold symptoms were predominant. Some studies have also implicated enteroviruses as triggers of pneumonia (1–7%).2,5 The 6 cases observed in this study represented 7.5% of the ARIs caused by enterovirus. No patients were found to have associated neurological symptoms.
Please cite this article as: Reina J, Cabrerizo M, Aliaga F. Infecciones respiratorias agudas comunitarias causadas por enterovirus en la población pediátrica. Enferm Infecc Microbiol Clin. 2017;35:133–135.
