






Rotator cuff tears are the leading cause of pain and functional disability of the shoulder. Conservative treatment is an essential part of their management. Despite the limited evidence, rehabilitation is the mainstay of the treatment for rotator cuff tears associated to impingement syndrome. There are current reports on the utility of strengthening with resistance, particularly by eccentric exercise.
This report aims to present an overview of the efficacy of eccentric exercises in tendinopathies and current evidence of its benefit in rotator cuff tears.
Four studies published on eccentric strengthening for rotator cuff tears were analysed. There is theoretical evidence about its usefulness in this pathology, but only a controlled clinical trial has been published with data on improvement in strength but not in pain or functionality.
ConclusionsMore studies are needed with better methodological designs in order to generate evidence of their utility and recommendation.
Las lesiones del manguito rotador son la principal causa de dolor y discapacidad funcional del hombro. El tratamiento conservador es parte fundamental de su manejo. Existen publicaciones recientes sobre la utilidad del fortalecimiento excéntrico en este tipo de lesiones asociadas a pinzamiento subacromial.
El presente reporte tiene como objetivo mostrar un panorama general sobre la utilidad de los ejercicios excéntricos en las tendinopatías y la evidencia actual de su beneficio en las lesiones del manguito rotador.
Se analizan 4 estudios publicados sobre fortalecimiento excéntrico en lesiones del manguito rotador. Existe evidencia teórica sobre su utilidad en la patología, aunque solo un ensayo clínico controlado ha sido publicado con datos sobre mejoría en la fuerza pero no en el dolor o la funcionalidad del hombro.
ConclusionesEs necesario realizar más estudios con mejores diseños metodológicos para tener mayor evidencia de su utilidad y poder generar algún grado de recomendación.
Rotator cuff is the anatomical term to describe the tendon complex that is made up of the supraspinatus, infraspinatus, subscapularis and teres minor muscles. It is an integral component in shoulder movement and stability. Its affectation represents one of the main causes of joint pain and dysfunction1. Approximately 4% of people between 40-60 years suffer from partial or complete tear and up to 54% of adults over 60 years suffer from this affectation2. Its aetiology is multifactorial. Factors related to tear development are classified into intrinsic (hypovascularity, ageing-related metabolic alterations), extrinsic (subacromial compression) and traumatic (acute or repetitive microtraumatisms)3.
Symptoms can be classified into 2 groups: those caused by subacromial bursitis and tendinitis (pain, inflammation, reduced mobility) and those caused by tendon tear (decrepitation, weakness and atrophy). In general, both types coexist simultaneously4.
Subacromial compressionThe concept of subacromial compression syndrome was introduced in 1972 by Neer to describe a group of pathologies that produced pain when raising the shoulder and whose causes included bursitis, tendinitis, calcifications and rotator cuff tears5. It was later defined as a mechanic irritation of the rotator cuff and the bursa when compressed in the subacromial area and clinically characterized by painful shoulder abduction, reduced active mobility and progressive loss of strength and muscular function6,7. Such symptoms may or may not be associated with tendon complex tears8.
Treatment of rotator cuff lesions and subacromial compressionThe treatment of rotator cuff tears includes surgical and non-surgical approaches. Among them are included the use of analgesic and anti-inflammatory drugs, rehabilitation, infiltrations with local anaesthetics, steroids or high molecular weight hyaluronates, tear debridement or open or arthroscopic repair9.
In a review published by Cochrane library about rotator cuff lesion management, it was established that there was scarce evidence to support or reject the efficiency of one treatment over another10, though it is generally recommended to start with the least invasive, conservative management for a period from 6 to 12 weeks, assess the response and, in each case, consider surgical treatment2,11.
Despite limited evidence, rehabilitation is the cornerstone of conservative management for rotator cuff tears with or without subacromial compression9.
The aim of rehabilitation is to reduce pain and the inflammatory process, favour cicatrisation, maintain and increase mobility arches and restore glenohumeral and scapulothoracic balance. Such goals are accomplished by implementing therapeutic exercise programs that include different types of muscular strengthening3.
Eccentric contraction exerciseEccentric strengthening consists of making contractions while enlarging the muscle or in terms of movement, the resistance produced by the distance of muscular inserts. This type of contraction is made when joint movement is stopped12. Eccentric concentration is coachable and also presents the following theoretical advantages: preferential recruitment of IIb fibre, which stimulates quick-reaction fibres and, hypothetically, is efficient in the prevention of tendon-related lesions, it increases active muscular tension, promotes generation of tensions from 30 to 50% higher than the maximum isometric strength, reduces sensitivity of Golgi tendon organs, increases the collagen density in the tendon, consumes little metabolic and nervous energy, and has a reduced impact on muscular volume. Eccentric exercise exposes the tendon to a greater burden than concentric and, apparently, produces a repair effect after muscular micro-tears13. Some of the inconveniences of eccentric training may include a high rate of muscular fatigue and the risk of lesion in the event of training with inappropriate technique14.
Effects of eccentric concentration on tendonsAlfredson15 discovered that during every eccentric exercise sequence, there was a temporary interruption of blood flow in tendon neovessels. This was demonstrated through Doppler ultrasonography, by means of which it was possible to observe tendon vascularity after 12 weeks of eccentric training16. Some studies also report a reduction of 45% of abnormal flow of peritendinous capillary blood, with effects pain in patients with Achilles tendinopathy17.
Repetitive burden and unburden pattern caused by eccentric exercise provides ongoing mechanical stimulus, which would induce tendon remodelling, similar to the burden exercised on the bone during mechanical stimulation with high frequencies18.
Langberg et al.19 reported the existence of an increase of collagen synthesis in damaged tendons as a result of an eccentric training programme for 12 weeks, as well as an increase in the concentration of peritendinous type I collagen, which was clinically related to a reduction in pain levels. Such finding was not found in healthy tendons.
Eccentric exercise performed on a regular basis theoretically reduces pain due to the ongoing desensitization of peripheral mechanisms of transmission, the central adaptation by agonist and antagonistic muscular groups, and the increase in tendon resistance, which reduce the possibility of the inflammatory process20.
Treatment with eccentric muscle training is defined by some authors as painful, who even use the term “painful eccentric muscle training.” Said program has provided positive clinical results in patients with chronic Achilles tendinopathy, in whom histological changes compatible with favourable structural modifications of the tendon 21,22 have been found, although there are recent reports with contrary results that show limited effectiveness of the treatment23,24. Therefore, its usefulness is controversial. Some examples of eccentric contraction exercises for deltoids, supraspinatus and muscles of the rotator cuff are illustrated in figures 1-4.




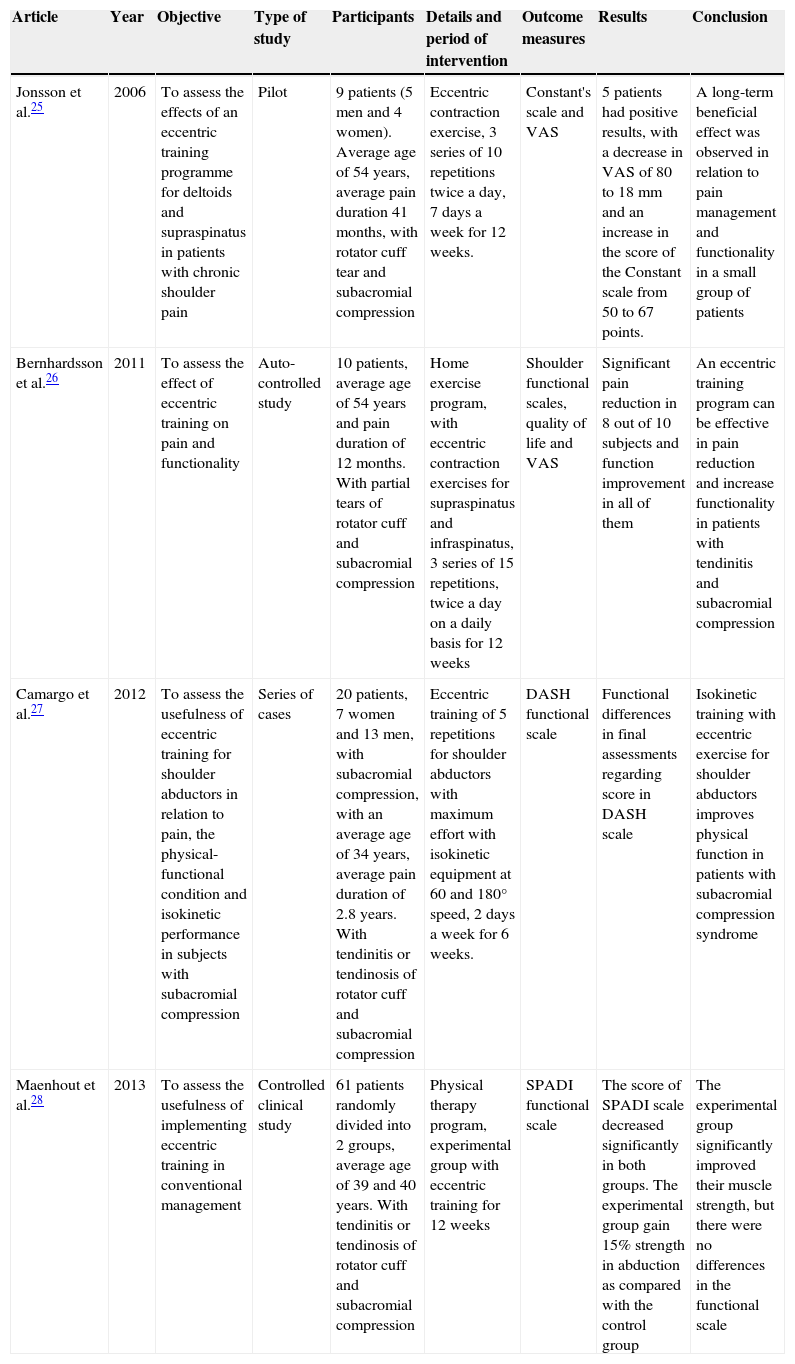
With the aim of assessing the existing evidence about the benefit of eccentric strengthening in rotator cuff tendinopathies, a search was carried out in the Pubmed electronic database with the terms: ™tendon,∫ ™tendinopathy,∫ ™tendinitis,∫ ™eccentric,∫ ™rotator cuff∫ and ™resistance training.∫ One of the first 3 terms was combined with each of the remaining 3. A total amount of 43 articles was found. After a clean-up according to the type of study (clinical study), only 4 studies were left that included treatment of rotator cuff lesions with eccentric exercises. Most of the articles found indicate results of rotator cuff lesions associated with subacromial compression. Due to the scarcity of publications, it was decided to include the analysis of those 4 articles in this report. The general characteristics of the studies included are shown in Table 1.
Characteristics of reported studies on eccentric exercises in rotator cuff lesions.
| Article | Year | Objective | Type of study | Participants | Details and period of intervention | Outcome measures | Results | Conclusion |
|---|---|---|---|---|---|---|---|---|
| Jonsson et al.25 | 2006 | To assess the effects of an eccentric training programme for deltoids and supraspinatus in patients with chronic shoulder pain | Pilot | 9 patients (5 men and 4 women). Average age of 54 years, average pain duration 41 months, with rotator cuff tear and subacromial compression | Eccentric contraction exercise, 3 series of 10 repetitions twice a day, 7 days a week for 12 weeks. | Constant's scale and VAS | 5 patients had positive results, with a decrease in VAS of 80 to 18mm and an increase in the score of the Constant scale from 50 to 67 points. | A long-term beneficial effect was observed in relation to pain management and functionality in a small group of patients |
| Bernhardsson et al.26 | 2011 | To assess the effect of eccentric training on pain and functionality | Auto-controlled study | 10 patients, average age of 54 years and pain duration of 12 months. With partial tears of rotator cuff and subacromial compression | Home exercise program, with eccentric contraction exercises for supraspinatus and infraspinatus, 3 series of 15 repetitions, twice a day on a daily basis for 12 weeks | Shoulder functional scales, quality of life and VAS | Significant pain reduction in 8 out of 10 subjects and function improvement in all of them | An eccentric training program can be effective in pain reduction and increase functionality in patients with tendinitis and subacromial compression |
| Camargo et al.27 | 2012 | To assess the usefulness of eccentric training for shoulder abductors in relation to pain, the physical-functional condition and isokinetic performance in subjects with subacromial compression | Series of cases | 20 patients, 7 women and 13 men, with subacromial compression, with an average age of 34 years, average pain duration of 2.8 years. With tendinitis or tendinosis of rotator cuff and subacromial compression | Eccentric training of 5 repetitions for shoulder abductors with maximum effort with isokinetic equipment at 60 and 180° speed, 2 days a week for 6 weeks. | DASH functional scale | Functional differences in final assessments regarding score in DASH scale | Isokinetic training with eccentric exercise for shoulder abductors improves physical function in patients with subacromial compression syndrome |
| Maenhout et al.28 | 2013 | To assess the usefulness of implementing eccentric training in conventional management | Controlled clinical study | 61 patients randomly divided into 2 groups, average age of 39 and 40 years. With tendinitis or tendinosis of rotator cuff and subacromial compression | Physical therapy program, experimental group with eccentric training for 12 weeks | SPADI functional scale | The score of SPADI scale decreased significantly in both groups. The experimental group gain 15% strength in abduction as compared with the control group | The experimental group significantly improved their muscle strength, but there were no differences in the functional scale |
Jonsson et al.25 revealed the results obtained from a pilot study which included 9 patients (5 women and 4 men, with an average age of 54 years) who suffered from chronic shoulder pain, diagnosed with subacromial compression and rotator cuff lesion, in protocol study for surgical treatment. They underwent a supervised eccentric training programme for supraspinatus muscles and deltoids (3 sets of 15 repetitions, twice a day, 7 days a week for 12 weeks). There were assessments of pain through a visual analogue scale (VAS), of the level of satisfaction (using Likert's scale) and functionality (using Constant's scale). Five of them were satisfied with the treatment, with significant pain reduction of 62 to 18mm (p < 0.05) and a score increase from 65 to 80 (p < 0.05) in Constant's scale. After 52 follow-up weeks, those five patients continued to be satisfied and were removed from the surgical waiting list. They continued with VAS of 31mm and Constant score of 81. Two of those patients had partial tear of supraspinatus tendon and three of them had tendinitis and compression. The authors conclude that, despite the fact that this is a preliminary study, a long-term beneficial effect was observed related to pain and functionality with the programme of painful eccentric muscle training for supraspinatus and deltoids. They also declared to continue with monitored studies in order to reproduce the obtained results25.
Bernhardsson et al.26 published a study aimed at assessing the eccentric training effect on pain intensity and shoulder functionality in patients with subacromial compression. It is a sort of “before and after” auto-controlled study, with a home training programme of supervised exercises and supported by visits to a physiotherapy clinic. Ten patients with an average age of 54 ± 8.6 years were included, with an average pain duration of 12 ± 9.1 months. They underwent the strengthening programme for 12 weeks; initial pain intensity was measured with VAS, and function with the Patient-Specific Functional Scale, the Constant scale and quality of life using the Western Ontario Rotator Cuff Index. The authors reported that pain intensity decreased significantly in 8 out of 10 subjects and all the patients saw improvement in their shoulder function. The average Constant score increased significantly from 44 to 69 points (p = 0.008) and the average score of the Western Ontario Rotator Cuff Index increased from 51 to 71% (p = 0.021). The authors concluded that a strengthening training programme with eccentric exercises for rotator cuff muscles and the scapular waist can be effective in pain reduction and increases functionality in patients with tendinitis and subacromial compression, when the right pattern of movement is followed26.
Camargo et al.27 reported a series of cases aimed at assessing the benefits of eccentric training for shoulder abductors related to pain, the physical-functional condition and isokinetic performance during eccentric abduction in subjects with subacromial compression syndrome. Twenty patients were included, with an average pain duration of 2.8 ± 2.9 years. Five assessments were made, a baseline (0) and four subsequent assessments. For the functionality assessment, DASH questionnaire was used and it was previously validated in patients with subacromial compression. Firstly, both shoulders were assessed with an isokinetic dynamometer, registering the maximum torque of 5 repetitions. The exercise protocol was performed twice a week, every other day, in the same position as the assessment, in a training range of 60° (20°-80°). For each training day, 3 sets of 10 repetitions were performed with a resting period of 3minutes between every set. As a result, the authors reported statistically significant differences in relation with the effect measured by the DASH scale. There were no differences (p = 0.25) found between assessments 1 and 2. However, assessment 4 showed lower values compared to assessment 1 (p < 0.01), 2 (p = 0.02) and 3 (p = 0.02); likewise, torque peak, total work and acceleration improved significantly after the intervention (p < 0.05). This study indicates that isokinetic training with eccentric exercise for shoulder abductors improves the physical function of the upper extremity in patients with subacromial compression syndrome27.
Maenhout et al.28 published the only controlled randomized clinical study so far, in which 61 patients diagnosed with subacromial compression were included. They were randomly divided into 2 groups: a control group with conservative treatment for subacromial compression (n = 30, average age of 39.4 ± 13.1 years) and an experimental group, which included conventional treatment and eccentric training (n = 31, average age of 40.2 ± 12.9 years). The isometric force was measured in abduction ranges of 0°, 45° and 90° for rotations. In order to measure pain and shoulder function, the SPADI questionnaire was used. In the same manner, patients were asked about their subjective perception of improvement. Both groups underwent physiotherapy for 12 weeks with ongoing supervision. At home, the control group performed rotator cuff strengthening exercises once a day. The experimental group performed the same exercises once a day and eccentric exercise with burden twice a day. At the end of the treatment, there was a significant overall increase in strength in both groups. Moreover, the score of the SPADI scale decreased significantly. The experimental group gained 15% strength in scapular abduction compared to the control group, even though there were no differences in their perception of improvement. The authors concluded that adding eccentric training with burden resulted in gaining strength, but it was not better to reduce pain and improve shoulder function28.
ConclusionsPublished studies show positive results in favour of the use of this kind of exercise in tendinopathies related to the rotator cuff. However, only one controlled clinical study shows objective improvement in strength, but not in pain management or functionality.
It is necessary to take into consideration that all studies included patients diagnosed with rotator cuff lesions related to subacromial compression, so it is important to include subjects without compression and determine whether that group would also benefit from this treatment.
Further studies need to be carried out, with better designs and a larger number of patients in order to obtain better evidence and to be able to provide some grade of recommendation about its usage, which cannot be established with the current data.
Conflict of interestThe authors declare that there are no conflicts of interest.
Please cite this article as: Macías-Hernández S.I. et al. Fortalecimiento excéntrico en tendinopatías del manguito de los rotadores asociadas a pinzamiento subacromial. Evidencia actual. Cirugía y Cirujanos. 2015; 83: 74–80.