



Cardiac hydatid cyst is very a rare manifestation of hydatid disease. It is potentially life threatening, and characterized by its clinical polymorphism, thus making an early preoperative diagnosis challenging. The sole curative treatment of this disease is surgery, and it should be done as emergent as possible after diagnosis, in order to minimize the risk of serious complications like embolism and anaphylaxis.
We report a case of a 22 years old male who had multivesicular cyst formation in the left ventricle free wall, which was measuring 14×8cm. The patient underwent surgery in order to remove this hydatid cyst, by using the cardiopulmonary bypass, and his postoperative course was unremarkable.
El quiste hidatídico cardiaco es una manifestación muy rara de la enfermedad hidatídica y potencialmente mortal, caracterizada por su polimorfismo clínico, lo que dificulta su diagnóstico preoperatorio temprano. La cirugía sigue siendo el único tratamiento curativo del quiste hidatídico cardiaco. Este debe ser tratado lo más pronto posible después del diagnóstico, ya que minimiza el riesgo de complicaciones graves como embolia y anafilaxia.
Presentamos el caso de un varón de 22 años que presenta una formación de quiste multivesicular en la pared libre del ventrículo izquierdo de 14×8cm. El paciente fue intervenido quirúrgicamente mediante bypass cardiopulmonar para extirpar el quiste hidatídico de la pared libre del ventrículo izquierdo, con un resultado satisfactorio para el curso postoperatorio.
The cardiac hydatid cyst is a very rare manifestation of hydatid disease.1 It is potentially life threatening, and characterized by its clinical polymorphism, thus making an early preoperative diagnosis challenging.
The aim of this case report is to present a successful therapeutic management of cardiac hydatid.
Case presentationWe report a case of a 22 years old male who presented to the cardiac surgery department with a history of left-sided chest pain and palpitation. The physical examination on his admission was unremarkable. The electrocardiogram showed T wave inversion in leads V5 and V6. The transthoracic echocardiography revealed the presence of multivesicular cystic formation in the left ventricular free wall, which was measuring 14×8cm. The continuous-wave doppler ultrasound with color-flow mapping showed no connections between the cyst and the blood flow. Moreover, the thoracoabdominal computed tomography did not show other cystic formations beside the cardiac involvement (Fig. 1).
.")
In addition, hydatid serology was performed using western blot technic and enzyme-linked immunosorbent assay which came back negative.
Based on the World Health Organization (WHO) classification of ultrasound features of cystic lesion, the cardiac cystic was identified as type 2 active hydatid lesion.2
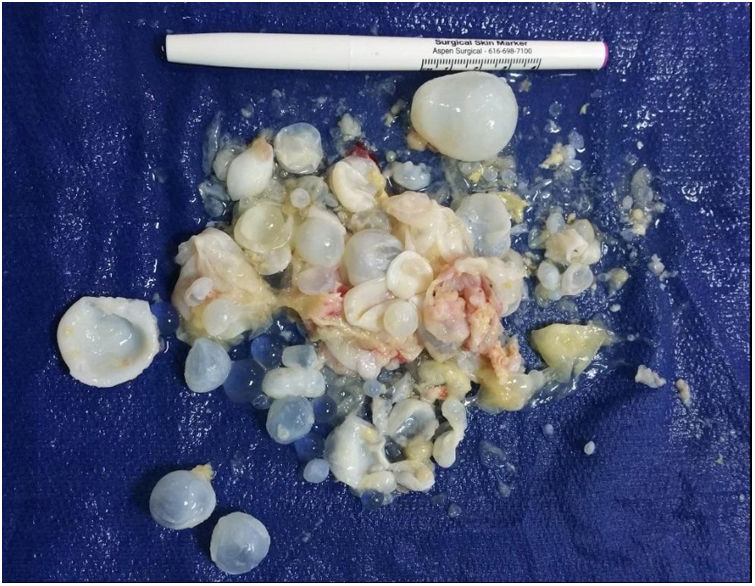
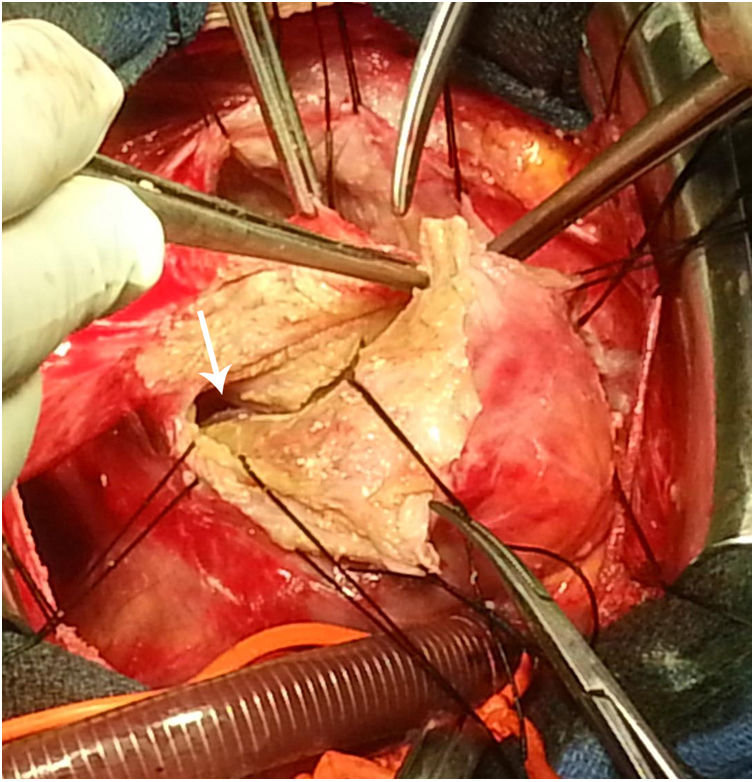
We undertook an emergent removal of the hydatid cyst in order to rule out embolism and reduce the risk thereof. Minimal cardiac manipulation was done throughout the procedure to prevent migration of vesicles and anaphylaxis. After pericardiotomy, the cyst was identified, adhering to the pericardium and taking up the free wall of the left ventricle. The ascending aorta was cannulated and a single two-stage venous cannula was placed into the right atrium. Then the cardiopulmonary bypass was started. After aortic cross-clamping, the myocardial protection was achieved. At this time, the left vent was carefully placed through the right upper vein. The resection of the dome of the cyst was performed and several daughter vesicles were subsequently evacuated (Figs. 2 and 3).

.")
Afterwards, a longitudinal left ventriculotomy was performed in order to remove vesicles from the free wall of the left ventricle. The residual pericystic cavity was destroyed with a combination of mechanical abrasion and chemical agents. The ventriculotomy incision was closed using patch and pledged sutures.
After deairing maneuvers, we released the aortic cross-clamp. Then spontaneous cardiac contractility resumed, and the patient successfully weaned from cardiopulmonary bypass. In what concerns the pathological and the microbiological analysis of the operative specimen, they confirmed the initial diagnosis.
The immediate postoperative course was uneventful. A follow up transthoracic echocardiograph showed normal values for left ventricular chamber dimensions, volumes and ejection fraction without any residual image. The patient was discharged from hospital on the 10th postoperative day.
Moreover, adjuvant therapy using oral albendazole was continued for three additional cycles of 28-days each, with a 14-day window between each cycle. Outcome was favorable six weeks after surgery without any signs of recurrence on physical examination and transthoracic echocardiography.
DiscussionThe cardiac hydatid cyst is a very rare manifestation of hydatid disease.1 It is potentially life threatening, characterized by its clinical polymorphism, thus making an early preoperative diagnosis challenging. Dyspnea, palpitations, chest pain and arrhythmia are common symptoms.3
The most common localizations of cardiac echinococcosis are the left ventricle (55–60%) because of its high myocardial mass and greater blood supply, followed by the right ventricle (15%), although the inter ventricular septum (5–9%) and the right atrium can also be affected (4%).4
Even though transthoracic echocardiography is gradually gaining popularity as first line imaging technic. The computed tomography remains the gold standard in cardiac localizations because it allows the preoperative workup of multi visceral localization. Besides, the magnetic resonance imaging, and especially the T2-weighted series have greater sensibility compared to computed tomography.
The transthoracic echocardiography is used to classify lesions into six types assigned to three clinical groups, the ‘active’, the ‘transitional’ and the ‘inactive’ group2:
- -
The ‘active’ group includes developing cysts, which may be unilocular (type 1 of cyclic echinococcosis) or multi-vesicular with daughter vesicles, called type 2 (cystic echinococcosis 2) and which are usually found to be viable.
- -
The ‘transitional’ group includes type 3 (cystic echinococcosis 3) includes both cysts with detachment of endocyst (cystic echinococcosis 3a) and predominantly solid cysts with daughter vesicles (cystic echinococcosis 3b).
- -
The ‘inactive’ group includes type 4 and type 5 (cystic echinococcosis 4 and cystic echinococcosis 5) seen as involution and solidification of cyst content with increasing degrees of calcification and which are mostly found to be non-viable.
Surgery remains the sole curative treatment of cardiac hydatid cyst. It should be as emergent as possible after diagnosis in order to minimize the risk of fatal complications like embolism and anaphylaxis.5 Besides, minimal cardiac manipulation is recommended during surgery.6 Furthermore, the surgical resection should be followed with adjuvant albendazole or mebendazole in order to reduce the risk of local recurrence of the cyst.5
ConclusionCardiac echinococcosis is a rare manifestation of cystic echinococcosis caused by the tapeworm, also called echinococcus granulosus. A combination of surgical removal and drug treatment for cardiac hydatid disease should be applied to symptomatic as well as asymptomatic patients in order to improve prognosis as soon as its diagnosis is made.
Ethics approvalIRB and clinical trial registration approval are not required for case reports.
Constant of the use of medical data is obtained verbally and in written form from the patient.
FundingThe authors report no involvement in the research by the sponsor that could have influenced the outcome of this work.
Conflicts of interestThe authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.

