

Medical Insurance Siglo XXI (MISXXI) in Mexico provides funds for the medical and preventive care of children from households lacking any health insurance, thus seeking to reduce impoverishing due to health problems. This paper analyzes mortality of children <2 years of age affiliated with this program and out-of-pocket expenses attributable to this event.
MethodsAn in-home survey addressed to determine the health conditions of children affiliated with MISXXI was carried out in all Mexican states. If the infant had died, information was collected with emphasis on diagnosis (death certificate), medical attention and out-of-pocket expenses. Diagnoses were classified in agreement with ICD-10.
ResultsOf 9181 children, 74 died by the time during which the survey was gathered; 51% of children died before 28 days. Deaths were attributable to short gestation, low birth weight, asphyxia, or sepsis. In newborns who died before 7 days of age, 95.7% received medical care; however, among those who died between 7 and 28 days, only 58% received medical care. During the neonatal period, medical care was predominantly given in the Ministry of Health facilities. During the post-neonatal period, almost all children received medical care, predominantly in private facilities, a reason for households incurring in out-of-pocket expenditures.
ConclusionsMortality of infants who are beneficiaries of MISXXI mainly occurs during the neonatal period; however, households incurred in out-of-pocket expenditures, especially in the post-neonatal period. It seems convenient to boost the access of users to benefits provided by this medical insurance.
“That day of highest risk for dying is, with the exception of the day of one's actual death, the day in which one is born”. Jesús Kumate
Children's mortality rate including number and causes is probably the indicator that most accurately reflects the quality of child healthcare.1,2 To reduce inequality levels among nations and within regions in a country, the United Nations has proposed that, during the period from 1990 to 2015, the community of nations should achieve eight Millennium Development Goals (MDG).3 Goal number four focuses on reducing the under-5 mortality rate by two-thirds. To achieve this goal, all the nations concerned, including Mexico, are working to improve their socioeconomic development and implement public healthcare measures appropriate for their needs. Since this initiative was launched, the under-5 mortality rate in developing countries has decreased from 100 to 72/1000 live births (–28%), although there are wide variations among countries depending on the level of development and success of the programs implemented.4 In Mexico, from 1980 to 1990, the mortality rate of children <5 years of age was reduced from 64.3 to 44.2/1000 live births.5 According to this latter figure the expected death rates to fulfill the MDG4 in 2015 is 15/1000 live births.6
Children <5 years of age are a vulnerable segment of the population because their health care depends entirely on adults. However, adults’ capability for taking care of children's health is associated with their education, employment and income levels and in small communities with their access opportunities to health care facilities as well as social protection systems.
In this context, a child <5 years of age who belongs to a family lacking access to health insurance or social security has a higher risk of acquiring diseases and dying than children with better standards of living.7
In order to provide healthcare services to children <5 years of age through a universal health insurance system, which includes a comprehensive medical and preventive care for those persons who are not entitled to any social security, and to contribute to the reduction of poverty of families due to health reasons, the Mexican Government created the program Medical Insurance “Siglo XXI” (MISXXI) to guarantee free healthcare services such as prevention, diagnosis, treatment and rehabilitation of diseases.8 Similarly, grant funding for those children includes a health insurance scheme with wide coverage, additional to that contained in the Universal Catalogue of Health Services (CAUSES)9 and Fund for Protection against Catastrophic Expenses (FPGC).10
MISXXI is interactive with other programs such as Healthy Pregnancy, PROSPERA (former “Oportunidades”); similarly ensuring immediate enrollment of the entire family to the System of Social Protection in Health.11 All of these programs have the purpose of reducing the risks associated with neonatal mortality and other conditions originating during the perinatal period and the prevention of damage to health and disabilities occurring in greater numbers in the course of this period of life, as well as reducing other associated illnesses, such as infections and malnutrition.
In this context, in 2009, three years after starting, an evaluation of MISXXI was undertaken, and the results have been published elsewhere.12–15
The present report is a subchapter of the above evaluation, in which infant mortality is analyzed in terms of number as a fraction of the total sample, causes, and the household's out-of-pocket (OOP) expenditures attributable to this event, by socioeconomic status.
2MethodsThe study protocol of the MISXXI Survey was approved by the Research and Ethics Committees of the Hospital Infantil de México Federico Gómez. The design was based on four main program domains described elsewhere.14 Although the survey originally contained no questions on child mortality, these were added as domain subchapter two after the pilot study performed to identify problems regarding quality of household records showed that some children had died. Questions about the death of children constituted Chapter 13 of the survey.14
After careful training of the pollsters and an exhaustive localization of the households, the survey was performed from March 16 to April 10, 2009 in Mexico, although complete information was obtained only in 9181 children out of 12,240 cases for reasons such as moving from the location or imprecise address. If during the visit to the household of the child beneficiary of the MISXXI the information was that the child died between December 2006 and September 2008, this was considered a case for the survey. The interview for gathering information about the deceased infant was done after obtaining written informed consent in accordance with the Helsinki Declaration.
To fulfill the question regarding death at ages <2 years, the following data were collected: (1) birth date, (2) birth weight, (3) gestational age, (4) date of death, (5) diseases which caused the infant's death, (6) medical care received during the disease, (7) institution in which medical care was given, (8) time elapsed between the onset of the illness and death, (9) who provided the medical services, (10) family income, and (if applicable) (11) how much money the family spent on the child's illness (OOP). No questions were addressed to explore preferences or administrative deficiencies in hospitals. The sources of information were the death certificate, when available, plus information given by parents or family members. The information obtained was analyzed as follows.
2.1Mortality of the childrenAlthough it would have been preferable to obtain mortality rates, limitations to achieve appropriate denominators in terms of cognizance of all live newborns in the study period, the information was described in percentages according to the following four categories1: (1) early neonatal (<7 days), (2) late neonatal (7–28 days), (3) postneonatal (29 to <1 year), and (4) mortality between 1 and 2 years of age. Additionally, for each category, demographic characteristics and the profile of medical care were analyzed.
2.2Out-of-pocket health expendituresThis refers to all health care payments made by households during the time they received health services from the MISXXI program. Expenditures included consultations, allopathic and homeopathic medication or expenses for alternative medicine, as well as hospital expenses, laboratory and imaging studies, or blood tests conducted during the period. The total amount of health care expenses of households was estimated from the beginning of the disease until the infant's death.
2.3Socioeconomic level of household of children who diedThe households were classified by socioeconomic level using deciles of annual per capita household expenditures. Cutoff points were taken from the National Income Expenditure Survey in Mexico 200816 (ENIGH 2008) and these were updated to 2009 prices. In this article, the level of household expenditures per capita is used because the household income tends to be under-reported. Furthermore, the latter could be subject to significant seasonal variations in rural areas.
2.4Leading causes of infant mortalityDiagnosis of the cause of death was obtained from death certificates. The disease that caused the infant's death was classified following the International Classification of Diseases (ICD), v. 2007 (ICD-10).2 If the family did not have the death certificate, the cause of death was assigned as unknown.
2.5Statistical analysesDeceased children were categorized according to the age in which death occurred. Using STATA SE 11.0 software from each parameter in each one of steps in which death occurred, statistics for reporting central and dispersion values were obtained, as well as percentages, proportions, and deciles of annual expenditure/per capita, and according to age in which the infant died, the median of household expenditure for medical attention was abstained.
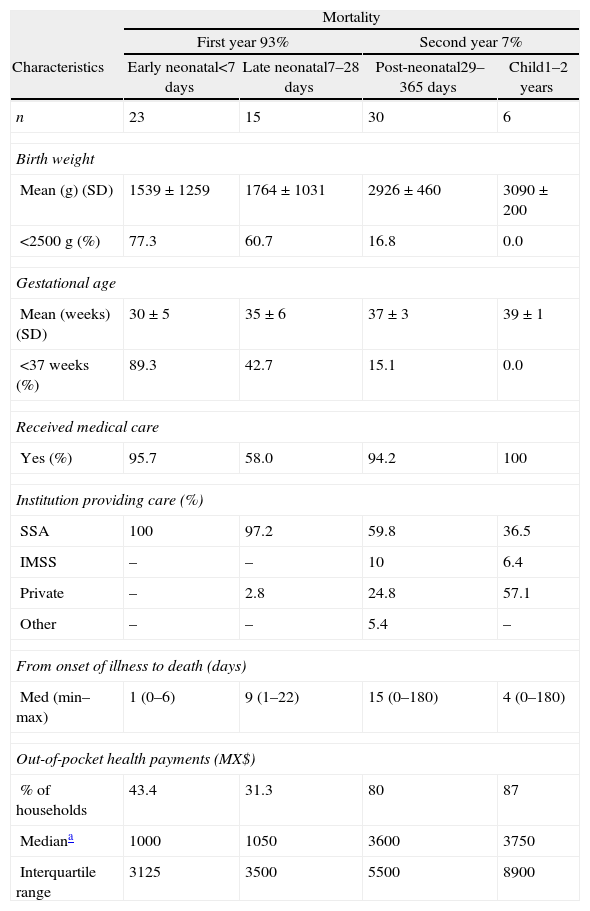
3Results3.1Mortality of childrenSeventy-four out of 9181 children were deceased by the time of the visit: 41 in rural and 33 in urban areas. Table 1 shows some demographic and socioeconomic characteristics of the MISXXI deceased beneficiaries. Of the 68 children who died in the first year of life, 23 died before 7 days (33.82%) and 15 died between 7 and 28 days (22.0%), which means that during the neonatal period 55.8% of deaths occurred. In the lapse from 29 to 365 days, 30 children died. Only six children died in the second year of life. The same table depicts the birth weight (g) of children who died, showing an inverse association between birth weight and gestational age with the number of children who died in the different periods elapsed in the first 2 years of life.
Demographic and socioeconomic characteristics of children affiliated with Medical Insurance SXXI according to age at time of death.
| Mortality | ||||
| First year 93% | Second year 7% | |||
| Characteristics | Early neonatal<7 days | Late neonatal7–28 days | Post-neonatal29–365 days | Child1–2 years |
| n | 23 | 15 | 30 | 6 |
| Birth weight | ||||
| Mean (g) (SD) | 1539±1259 | 1764±1031 | 2926±460 | 3090±200 |
| <2500g (%) | 77.3 | 60.7 | 16.8 | 0.0 |
| Gestational age | ||||
| Mean (weeks) (SD) | 30±5 | 35±6 | 37±3 | 39±1 |
| <37 weeks (%) | 89.3 | 42.7 | 15.1 | 0.0 |
| Received medical care | ||||
| Yes (%) | 95.7 | 58.0 | 94.2 | 100 |
| Institution providing care (%) | ||||
| SSA | 100 | 97.2 | 59.8 | 36.5 |
| IMSS | – | – | 10 | 6.4 |
| Private | – | 2.8 | 24.8 | 57.1 |
| Other | – | – | 5.4 | – |
| From onset of illness to death (days) | ||||
| Med (min–max) | 1 (0–6) | 9 (1–22) | 15 (0–180) | 4 (0–180) |
| Out-of-pocket health payments (MX$) | ||||
| % of households | 43.4 | 31.3 | 80 | 87 |
| Mediana | 1000 | 1050 | 3600 | 3750 |
| Interquartile range | 3125 | 3500 | 5500 | 8900 |
The survey was conducted in March and April of 2009 in a representative sample of all Mexican states.
SSA, Ministry of Health; IMSS, Instituto Mexicano del Seguro Social.
In relation to medical care provided to children while they were ill, Table 1 shows the percentage of children who received the care as well as facilities in which the medical care was given. In the first 7 days, 4.3% of all infants who died did not receive medical attention; the remaining received care at Ministry of Health facilities. Among children who died between 7 and 28 days, only 58% of newborns had medical care provided mainly at clinics of the Ministry of Health (97.2%). Subsequently until up to 2 years, almost all children received medical care; however, the number of children who received medical care in Ministry of Health units declined, whereas the number of children who sought care at private institutions increased. During the first year, the median number of days elapsed since the onset of illness to the child's death were 1, 9 and 15, for the first week, 7–28 days and postneonatal period, respectively. For children who died in the second year the time elapsed was 4 days.
3.2OOP payments for health careConcerning expenses incurred in the attempt to cure children's diseases, Table 1 also shows that in each one of the stages throughout the 2 years, the percent of households that spent money was less during the neonatal period and almost double in postneonatal periods.
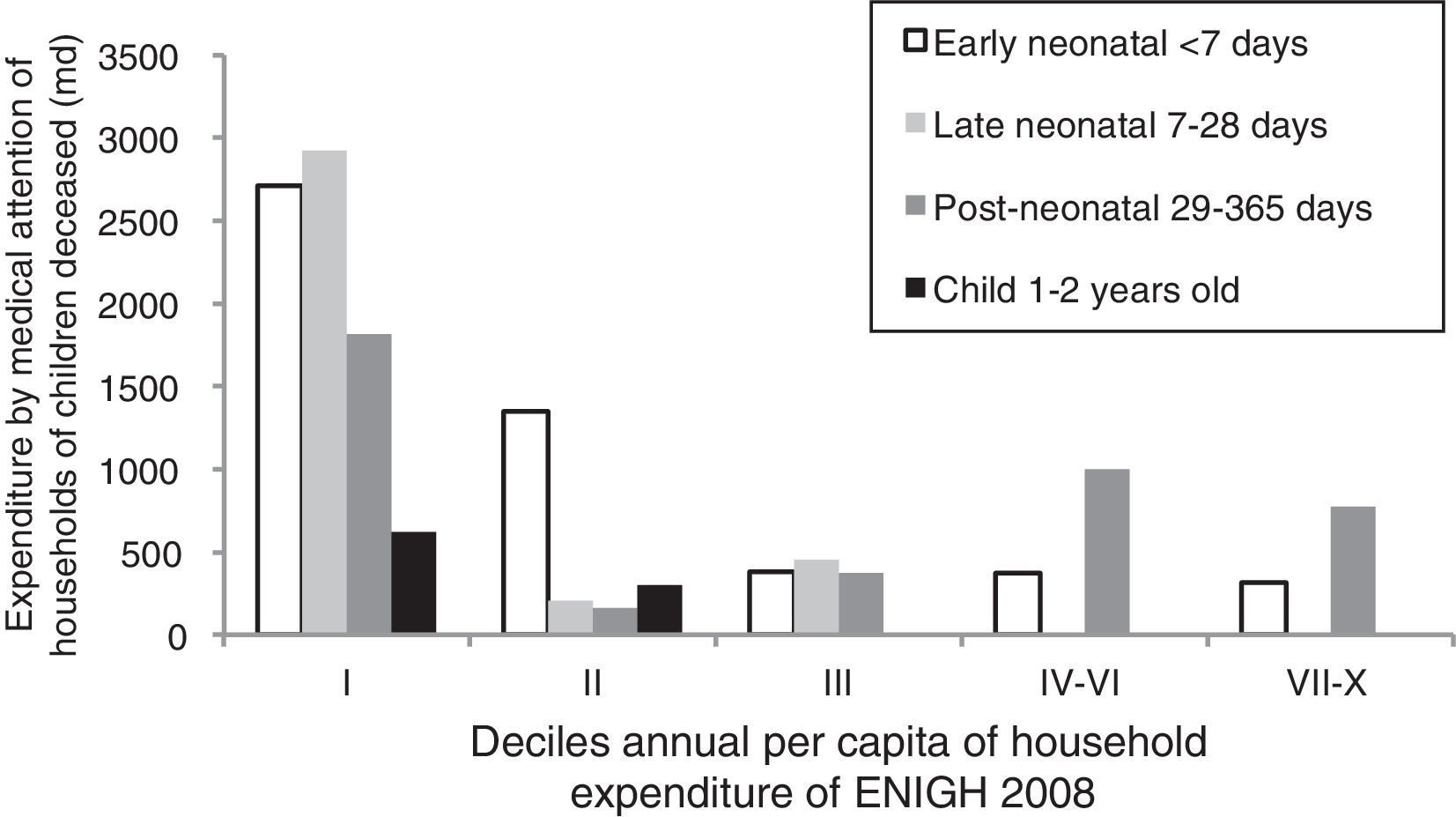
3.3Socioeconomic level of householdsEighty-two percent of households were concentrated in the first three deciles of per capita expenditure of ENIGH 2008. Fig. 1 shows the households classified by expenditure per capita according to the age when the infant died. Fig. 1 depicts the households according to annual deciles per capita of expenditure. In each one of the deciles are shown the stages in which the child's death occurs, finding that households who spend more money in an attempt to cure the children belong to the lowest deciles and are the poorest families.
3.4Leading causes of infant death
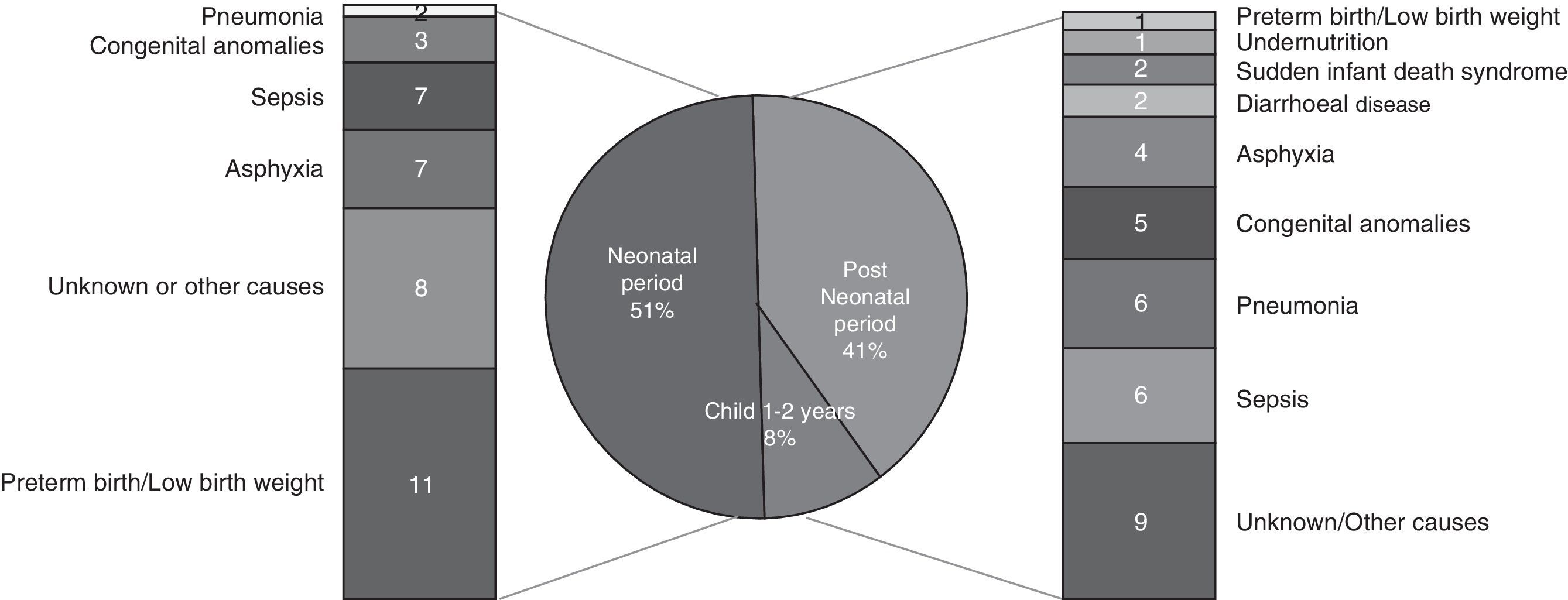
In ∼76% of children, death certificates were the source of information in regard to the causes of death. Fig. 2 shows that 51% occurred during the neonatal period, short gestation being the main cause, along with low birth weight, asphyxia, sepsis, and congenital anomalies being the leading causes of death. In the post-neonatal period, 41% of deceases occurred. The causes of infant mortality included sequelae or consequences of neonatal diseases and other infectious conditions such as sepsis, pneumonia, and diarrhea. Likewise, although not in a large proportion, protein-energy malnutrition and sudden infant death syndrome were also reported.
4Discussion
Almost 70% of deaths of children <5 years of age that occur worldwide are preventable. However, there has been widespread recognition that improvement of children's health and reduction of their mortality are not strictly dependent on medical reasons. Socioeconomic inequalities in child health care, poverty, fewer opportunities for female education, lack of potable water, and poor sanitation remain as barriers to a successful reduction of infant mortality.17
In Mexico, mortality rates of children both at <1 year and <5 years as well as of those during the neonatal stages have been reduced from 1980 to 2010 as a result of the implementation of various public health measures.18 In December 2006, the Mexican government initiated the MISXXI program with the expectation that in conjunction with other measures that tackle poverty this could reduce even more the under-five mortality rate.8
In this survey from all deaths that occurred in the first year of life, 55.8% occur before the 28th day of life and 33.8% before the 7th day. As far as the diseases that cause deaths in the neonatal period, low birth weight, premature birth associated with asphyxia, sepsis and congenital anomalies persist as leading causes,19,20 which indicates that high mortality in the first month of life has remained virtually unchanged for decades in Mexico.5,21,22
As mentioned above, seventy-four out 9181 children had died by the time in which the survey was gathered, and considering the study's limitations this represents a rate of 8.1 deaths per thousand households visited; figure which is below of the national average.
Concerning OOP expenditures associated with the infants’ death, the expectation was that funding of medical care by MISXXI would avoid household expenditure, thus reducing impoverishment as a cause of health problems. However, families incurred in out-of-pocket expenditures for medical care, and differences appeared between the amount of these expenditures in neonatal stages and the amount of the same expenditures in other stages.
During the early neonatal period in which onset of illness and death was 1 day, it is assumed that infants were not discharged from the hospital, but even in this period 43% of families spent money, much more by those belonging to decile I of annual per capita expenditure. In the late neonatal period it is assumed that children were in their home. The elapsed mean time between onset of illness and death was 9 days and only 58% received medical care mainly in government facilities; notwithstanding, 31.3% spent money. There is no information about the 42% of children who did not receive medical care. In the following periods there was an increase in the use of private facilities and the amount of money spent. With the information of this study, it is possible to conclude that equity is an uphill climb that is necessary to reach to cope with impoverishment due to medical care.7 Similar findings have been reported for sick children who regained their health with the resources of the MISXXI program.15
Concerning the death of children affiliated with the MISXXI, this study has a number of limitations. The first is that gender of the deceased children failed to be reported, an issue that in the first months of life has significant biological and social implications.
The second is that 25% of diagnoses were not taken from death certificates because the family lacked such documents. An explanation for this lack could be that, in remote villages, the national registry offices are often missing or as has been reported, families are unaware that they must notify this office about the infant's death.23,24
The third is that mortality is reported in terms of percentages instead of rates because we do not have reliable information regarding all births and all deaths of children enrolled in the MISXXI during the study period. However, these results could provide a window of opportunity to assess the weight of this insurance on decreasing infant mortality.
The fourth is that out-of-pocket expenditures were not broken down into lodging, transportation or meals, nor were other motives considered regarding why the families attended private health facilities.
After implementation of public health measures to reduce infant mortality as discussed herein,5,20 the question is whether Mexico will be able to achieve the MDG4. Since 1990, the Mesoamerican region has shown an annual reduction of 4.2% in the mortality rate of children <5 years of age, whereas the overall reduction is about 2.1% or half of the former.25 This suggests that countries of this region to which Mexico belongs will be able to fulfill the MDG4 by 2015.6 The MISXXI program would help to reduce the mortality rate of children <5 years of age if it fought to decrease the factors causing neonatal mortality.
Although MISXXI is just a financing enterprise not providing medical care to its beneficiaries, the program has comprehensive preventive and medical care components in its core, in which are included the increasing the sense of families’ self-care of health. Similarly, exerting synergistic actions with other programs should be requested from institutions in charge of giving medical attention, as well as implementing all preventive and educational measures during the key moments of human life, such as gestation and the perinatal period which should last for at least the first two years of life, in order to fulfill the program's objectives.
In the realm of the population covered by the MISXXI, an actual contribution is that all newborns who require medical attention are cared for in highly qualified government medical facilities; therefore, all surviving infant beneficiaries of MISXXI should be considered as contributions in the reduction of under-five mortality rates.26
Therefore, the MISXXI program deserves wider promotion among the population lacking medical insurance so that these persons will seek affiliation with this insurance. Families should as well be encouraged to learn about the program's coverage in order to receive the accruing benefits for their health care. It is also pertinent to conduct periodic assessments about the program accomplishments and move forward to cover all poor families with the benefits of this insurance as an important goal.
Mortality of children beneficiaries of MISXXI mainly occurs in the neonatal period, however, household beneficiaries of this health insurance incur in OOP expenditures, especially during the post-neonatal period. This program can contribute to reduce mortality of children under five years old, through the increased awareness of the benefits provided by this medical insurance and an increased capability to profit from it.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestNone of the authors reports any conflicts of interest.