



To assess the prevalence of physical inactivity among adolescents with HIV/AIDS, as well as associated factors.
MethodsNinety-one adolescents (from 10 to 19 years old) with HIV/AIDS who are patients at a university follow-up service were interviewed. Anthropometric data (weight, height, and waist circumference) were measured twice; clinical information was obtained from medical records, and habitual physical activity was assessed by a questionnaire proposed by Florindo et al. The cutoff point for sedentariness was 300minutes/week.
ResultsThe prevalence of inadequate height for age, malnutrition, and overweight/obesity was 15.4%, 9.9% and 12.1%, respectively. The most common physical activities were soccer (44.4%), volleyball (14.4%) and cycling (7.8%). The median times spent with physical activity and walking/bicycling to school were 141min and 39min, respectively. Most adolescents (71.4%) were sedentary and this proportion was higher among girls (p=0.046).
ConclusionsA high prevalence of physical inactivity among adolescents with HIV/AIDS was observed, similar to the general population. Promoting physical activity among adolescents, especially among girls with HIV/AIDS, as well as monitoring it should be part of the follow-up routine of these patients.
Verificar a prevalência de sedentarismo entre adolescentes com HIV/Aids e seus fatores associados.
MétodosForam entrevistados 91 adolescentes de 10 a 19 anos, com HIV/Aids, em acompanhamento em uma unidade de infectologia universitária. Foram coletados dados antropométricos (peso, altura e circunferência da cintura) em duplicata, informações clínicas foram obtidas nos prontuários médicos e a prática de atividade física habitual foi medida por meio do questionário proposto por Florindo et al. O ponto de corte para sedentarismo foi de 300 minutos/semana.
ResultadosAs prevalências de altura inadequada para idade, desnutrição e sobrepeso/obesidade foram de 15,4%, 9,9% e 12,1%, respectivamente. As atividades físicas mais citadas foram: futebol (44,4%), voleibol (14,4%) e andar de bicicleta (7,8%). Os tempos medianos dispendidos com a prática de atividade física e caminhando/andando de bicicleta até a escola foram de 141 minutos e 39 minutos, respectivamente. A maioria dos adolescentes (71,4%) era sedentária, proporção maior entre as meninas (p=0,046).
ConclusõesFoi observada alta prevalência de sedentarismo entre adolescentes com HIV/Aids, prevalência essa semelhante àquela observada na população geral. Promover a prática de atividade física entre adolescentes – especialmente entre meninas – com HIV/Aids, assim como monitorá-la, deve fazer parte da rotina de acompanhamento desses pacientes.
Approximately 9% of premature deaths (about 5.3 million of the 57 million deaths in 2008) and 6–10% of major non-communicable chronic diseases such as diabetes, coronary heart disease and breast and colon cancer can be attributed to physical inactivity. If sedentary individuals became physically active, it is estimated that worldwide life expectancy would increase by 0.68 years.1 A study carried out in the United States with individuals aged 50 years or older and physically inactive showed that becoming physically active would represent a gain of approximately 1.3–4.7 years in life expectancy. Thus, physical inactivity is comparable to other important modifiable risk factors, such as smoking and obesity.2
In patients with HIV/AIDS, physical activity practice can integrate non-pharmacological approaches to disease control. Since the introduction of highly active antiretroviral therapy (HAART), metabolic and morphological changes started to be of concern for patients undergoing treatment and health professionals. These changes include loss of fat in the facial region, the upper and lower limbs (lipoatrophy) and fat accumulation in the abdominal and cervical regions as well as breasts (lipohypertrophy), in addition to increase in levels of total cholesterol and serum triglycerides and increased peripheral insulin resistance.3
Physical activity, however, can help mitigate the side effects of this type therapy. Such is the importance of this issue that the Ministry of Health (MH) launched in 2012, the booklet “Physical activity recommendations for individuals with HIV and AIDS.” According to the MH, some of the practical benefits of physical activity by this population are the immune system stimulation and depression relief, preventing or reducing side effects of the use of antiretroviral therapy.4 Other institutions such as the Federal Council of Physical Education (Conselho Federal de Educação Física) also recommend physical activity for this population.5
In spite of its importance for individuals with HIV/AIDS, few studies have assessed the practice of physical activity by the adolescent population. The aim of this study was to determine the prevalence of physical inactivity among adolescents with HIV/AIDS and associated factors.
MethodThis is a cross-sectional study nested in a cohort of children and adolescents living with HIV/AIDS treated at the Infectious Diseases Unit of Instituto da Criança of Hospital das Clínicas da Faculdade de Medicina of Universidade de São Paulo.
Between April and September 2010, 124 adolescents aged 10–19 years enrolled in that service were identified. Of these, eight had not attended the scheduled visits in the previous six months; ten were not found; ten missed the scheduled evaluation; three refused to participate; and two were excluded due to health problems that impaired the practice of physical activity.
A total of 91 adolescents were interviewed for this study, which corresponds to 73% of eligible patients. They answered the physical activity assessment questionnaire for adolescents developed and validated by Florindo et al.6
The questionnaire consists of 17 questions, divided into two sections. Section I includes sports or physical exercises. Section I questions (1–15) refer to the three main physical activities by the adolescents, the weekly frequency and duration. To calculate the weekly duration (in minutes) of physical activity practice it is necessary to multiply the duration of sports/activities by the weekly frequency. Section II questions (16 and 17) consider the physical activities related to mobility to school (walking or cycling). The score of mobility to school is the time spent on this activity multiplied by five. The sum of the scores of sections 1 and 2 generates the final score “minutes of weekly physical activity.” Based on this value, the adolescents were classified as sedentary (<300min of physical activity per week) or active (≥300min/week), according to the cutoff proposed by Pate et al.7
Biochemical tests analyzed in this study refer to the three months before or after the interview. The information was collected from medical records and socioeconomic data were obtained from a questionnaire answered by parents/tutors at the time of interview.
The anthropometric assessment of adolescents was carried out by a previously trained nutritionist. The following were measured in duplicate: weight (kg), using a digital scale; height (meters) using a stadiometer, and waist circumference (cm), using an inelastic measuring tape. WHO Anthroplus software, version 1.0.3, was used to calculate the height z-score and BMI for age.8
Measures of central tendency as well as absolute and relative frequencies were used to characterize the sample. The chi-square test was used to test the association between physical inactivity and the dichotomous independent variables. For quantitative independent variables, we first verified the normal distribution using the Kolmogorov–Smirnov test and then the mean difference test was applied according to the distribution (Mann–Whitney test for nonparametric and Student's t test for parametric variables). All variables with p<0.20 were selected for the multivariate model, using the stepwise forward strategy. The SPSS (Copyright IBM Corporation 1994, 2012. SPSS for Windows, Version 15.0., USA) was used for all statistical analyses.
This study was approved by the Research Ethics Committee of Faculdade de Saúde Pública and Faculdade de Medicina da Universidade de São Paulo (protocol #1667/2007, 0144/10 and 2239/2011). The volunteers (aged >18 years) or parents/tutors (of patients aged <18 years) signed the free and informed consent form.
ResultsMedian age was 1.7 years at the diagnosis of HIV infection and 14.9 years at the time of the interview. Most adolescents (54.9%) were females, were vertically infected (95.6%) and used antiretroviral therapy (97.8%). The median time of antiretroviral therapy use was 11 years.
Ten respondents (11.0%) lived in halfway houses. Of the adolescents living with their families, 62.5% had parents (biological/adoptive) as their caregivers and the others had other relatives (uncles/aunts, siblings or grandparents). Most of the adolescents’ families (76.9%) lived with up to one minimum wage per capita (Table 1).
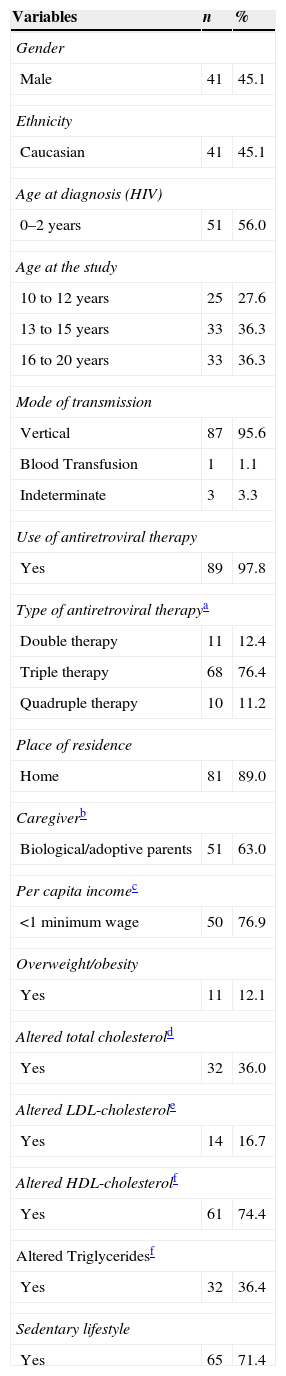
Number and percentage of adolescents, according to sociodemographic characteristics. Instituto da Criança, 2010.
| Variables | n | % |
|---|---|---|
| Gender | ||
| Male | 41 | 45.1 |
| Ethnicity | ||
| Caucasian | 41 | 45.1 |
| Age at diagnosis (HIV) | ||
| 0–2 years | 51 | 56.0 |
| Age at the study | ||
| 10 to 12 years | 25 | 27.6 |
| 13 to 15 years | 33 | 36.3 |
| 16 to 20 years | 33 | 36.3 |
| Mode of transmission | ||
| Vertical | 87 | 95.6 |
| Blood Transfusion | 1 | 1.1 |
| Indeterminate | 3 | 3.3 |
| Use of antiretroviral therapy | ||
| Yes | 89 | 97.8 |
| Type of antiretroviral therapya | ||
| Double therapy | 11 | 12.4 |
| Triple therapy | 68 | 76.4 |
| Quadruple therapy | 10 | 11.2 |
| Place of residence | ||
| Home | 81 | 89.0 |
| Caregiverb | ||
| Biological/adoptive parents | 51 | 63.0 |
| Per capita incomec | ||
| <1 minimum wage | 50 | 76.9 |
| Overweight/obesity | ||
| Yes | 11 | 12.1 |
| Altered total cholesterold | ||
| Yes | 32 | 36.0 |
| Altered LDL-cholesterole | ||
| Yes | 14 | 16.7 |
| Altered HDL-cholesterolf | ||
| Yes | 61 | 74.4 |
| Altered Triglyceridesf | ||
| Yes | 32 | 36.4 |
| Sedentary lifestyle | ||
| Yes | 65 | 71.4 |
The prevalence of inadequate height for age, malnutrition and overweight/obesity were 15.4% (95% CI=8.0, 22.8), 9.9% (95% CI=3.8; 16.0) and 12.1% (95% CI=5.4, 18.8), respectively.
Regarding laboratory tests, 74.4% of the adolescents had low HDL-cholesterol and 36.4% had alerted levels of triglycerides. Of the total, 32 (36.4%) adolescents had an undetectable viral load.
The physical activities most frequently mentioned by the adolescents were: soccer (44.4%), volleyball (14.4%) and cycling (7.8%). The median times spent on the practice of physical activity and walking/cycling to school were, respectively, 141min and 39min. Of the interviewed adolescents, 29 (31.9%) said they did not practice any type of physical activity.
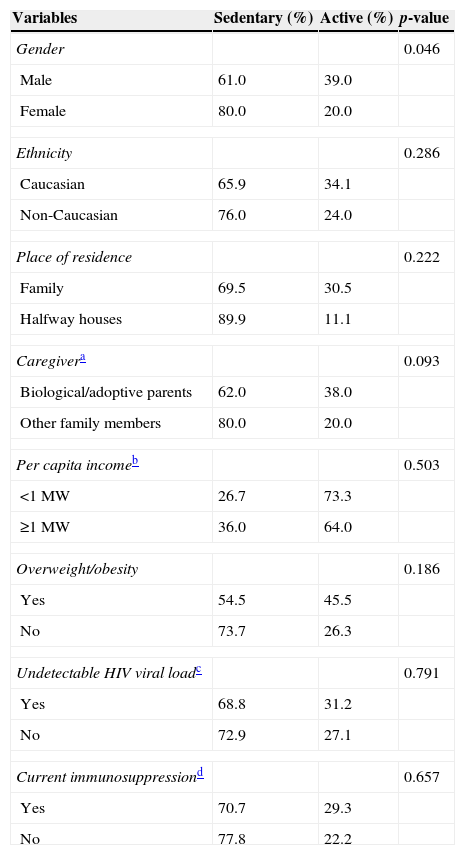
High prevalence of physical inactivity was observed among the adolescents: 71.4% (95% CI=62.1; 80.7), with a higher proportion of girls (girls 80.0% versus 61.0% boys; p=0.046). The univariate analysis between physical inactivity and the other independent variables found no statistically significant associations (Table 2).
Prevalence of adolescents according to independent variables and physical activity. Instituto da Criança, 2010.
| Variables | Sedentary (%) | Active (%) | p-value |
|---|---|---|---|
| Gender | 0.046 | ||
| Male | 61.0 | 39.0 | |
| Female | 80.0 | 20.0 | |
| Ethnicity | 0.286 | ||
| Caucasian | 65.9 | 34.1 | |
| Non-Caucasian | 76.0 | 24.0 | |
| Place of residence | 0.222 | ||
| Family | 69.5 | 30.5 | |
| Halfway houses | 89.9 | 11.1 | |
| Caregivera | 0.093 | ||
| Biological/adoptive parents | 62.0 | 38.0 | |
| Other family members | 80.0 | 20.0 | |
| Per capita incomeb | 0.503 | ||
| <1 MW | 26.7 | 73.3 | |
| ≥1 MW | 36.0 | 64.0 | |
| Overweight/obesity | 0.186 | ||
| Yes | 54.5 | 45.5 | |
| No | 73.7 | 26.3 | |
| Undetectable HIV viral loadc | 0.791 | ||
| Yes | 68.8 | 31.2 | |
| No | 72.9 | 27.1 | |
| Current immunosuppressiond | 0.657 | ||
| Yes | 70.7 | 29.3 | |
| No | 77.8 | 22.2 | |
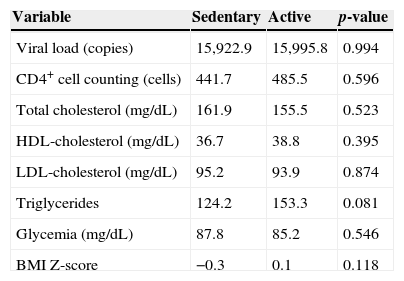
There was no statistical difference between the means of biochemical tests and BMI z-score when comparing sedentary adolescents and active ones (Table 3).
Comparison of biochemical parameters between sedentary and active adolescents. Instituto da Criança, 2010.
| Variable | Sedentary | Active | p-value |
|---|---|---|---|
| Viral load (copies) | 15,922.9 | 15,995.8 | 0.994 |
| CD4+ cell counting (cells) | 441.7 | 485.5 | 0.596 |
| Total cholesterol (mg/dL) | 161.9 | 155.5 | 0.523 |
| HDL-cholesterol (mg/dL) | 36.7 | 38.8 | 0.395 |
| LDL-cholesterol (mg/dL) | 95.2 | 93.9 | 0.874 |
| Triglycerides | 124.2 | 153.3 | 0.081 |
| Glycemia (mg/dL) | 87.8 | 85.2 | 0.546 |
| BMI Z-score | −0.3 | 0.1 | 0.118 |
The final model chosen was the univariate model (sedentary lifestyle versus gender) – as the other dependent variables were not statistically significant in the tested multivariate models – using the stepwise forward technique (Table 4).
DiscussionThe present study found a high prevalence of physical inactivity among adolescents living with HIV/AIDS, which was higher in girls. Other assessed factors, such as place of residence, caregiver and income, as well as anthropometric data, were not associated with the sedentary lifestyle. Regarding the type of exercise practiced by the adolescents, the most common were soccer, volleyball and cycling.
The findings of the present study are similar to those found in other publications that investigated the practice of physical activity among adolescents in the general population in Brazil and worldwide.9–15
The National Survey on Schoolchildren's Health (Pesquisa Nacional de Saúde do Escolar – PeNSE) carried out in the capitals and the Federal District of Brazil evaluated the physical activity practice on the seven days prior to the interview. The cutoff used was also 300min of physical activity/week. Of the total, 56.9% of the adolescents were sedentary, with this behavior being more prevalent among girls (68.7% girls versus 43.8% boys). Another association identified by the survey was a higher prevalence of physical inactivity among public school students when compared to students from private schools.13
It is noteworthy that in the study by Guthold et al,9 which analyzed data on physical activity of adolescents aged 13–15 years from 34 countries and did include Brazil, observed only one exception regarding the proportion of sedentary girls versus boys: in Zambia, where there was a higher proportion of sedentary boys. A study of 177 adolescents (100 girls and 77 boys) investigated the perception of physical activity behavior among girls, through focal groups. Both boys and girls described active girls as “too aggressive”. Boys often considered physically active girls as “too athletic”. This type of perception may negatively influence the practice of physical activity by girls.16
However, due to the use of different tools, both in data collection and their subsequent classification, comparison between studies becomes limited. In spite of this limitation and based on the above data, it can be concluded that physical inactivity is a global problem, which is prevalent in both developing and developed countries.9–14
We found two studies carried out in Brazil on the practice of physical activity among adolescents with HIV/AIDS. One of these studies investigated children and adolescents (7–14 years) orphaned by AIDS, of which only 5.5% of the sample had positive serology for HIV. The study used the same questionnaire and cutoff used in the present study, allowing direct comparison of results. The prevalence of sedentary lifestyle was 42%. Two findings are similar to those found in this study: association between physical inactivity and gender and sports that were more often practiced (soccer and volleyball).11
The other study was carried out in Florianopolis and its primary objective was to evaluate bone density of 48 adolescents with HIV/AIDS, with physical activity being used as the control variable. Physical activity was measured using pedometers, applied for five days, including two days at the weekend. The step count of 10,000 steps/day was used to classify the level of physical activity in adolescents. Approximately 70% of respondents had inadequate levels of physical activity. The authors found no statistically significant difference in the mean step count between genders.17
Physical activity practice may be an important strategy for the prevention or control of metabolic and morphological alterations associated with infection and also the use of HAART. The review article by Fillipas et al18 analyzed nine randomized controlled trials comparing the intervention group (aerobic exercise) to the control group. The results showed decreased body mass index, triceps skinfold, total body fat, waist circumference and waist-to-hip ratio. The present study found no association between anthropometric variables and the practice of physical activity. It is noteworthy that skinfold thickness and hip circumference were not measured, limiting the nutritional assessment of the study population.
A study evaluating the effect of a structured nutrition program and physical activity in children with HIV found that after 24 physical exercise sessions, there was a significant increase in muscular strength and endurance and maximal oxygen consumption (VO2).19
Studies performed in Brazil analyzing physical activity and lipodystrophy in adult patients with HIV/AIDS also found similar associations. Florindo et al.20 observed an inverse association between duration of physical activity and accumulation of abdominal fat, whereas Segatto et al.21 observed a lower prevalence of lipodystrophy in active individuals, when compared to sedentary ones. We did not observe similar associations in the present study. One of the possible reasons for this fact is the study design. As it is a cross-sectional study, both the exposure (socioeconomic variables and laboratory tests) and the outcome (physical activity or inactivity) were measured at the same moment.
Encouraging the practice of physical activity is part of the World Health Organization (WHO)’s agenda. After the publication of the World Health Report 2002, which disclosed that 60% of all deaths could be attributed to chronic diseases, the WHO Global Strategy on Diet, Physical Activity and Health was launched. Thus, the WHO emphasized the need to reduce exposure to risk factors for the development of chronic diseases, by adopting a healthy diet and regular physical activity. According to the WHO, “at least 30min of moderate physical activity on most days reduces the risk of cardiovascular disease and diabetes, colon and breast cancer.”22 Equally concerned with questions about physical activity among adolescents, the US government launched the “2008 Physical Activity Guidelines for Americans”.23 Together with the guidelines, “The NHANES – National Youth Fitness Survey” was also created, which collected in 2012 information on the physical activity of children and adolescents aged 3–15 years living in the United States.24 The monitoring of physical activity in adolescents by the multidisciplinary team can be used as an approach to assess physical activity over time and identify changes. The habitual physical activity questionnaire is easily applied and uses simple calculations and can be incorporated into routine patient care without causing major problems.
In addition to monitoring, it is essential to promote the practice of physical activity in this population while taking into account gender issues, aiming to reduce the risk for the onset of chronic diseases and side effects of antiretroviral therapy, as well as boost the immune system and relieve depression symptoms.
FundingFundação de Amparo à Pesquisa do Estado de São Paulo – FAPESP (processes: #10/01187-9 and #08/53322-7), Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPq (process: #135885/2011-4) and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – CAPES (Master's Degree Grant in the Social Demand Program).
Conflicts of interestAline Medeiros da Silva is currently an employee at Janssen Pharmaceutical Companies, but was hired after the present study was carried out.
We thank the medical team from Instituto da Criança: Samantha Brasil Andrade, Cláudia Menezes, Vera Lúcia Moyses Borelli, Maria de Fátima Carvalho and Nádia Litvinov. We also thank the collection team: Sofia de Fátima da Silva Barbosa de Oliveira, Flávia Monique Santos and Elissa Carolina Mendes for their help.
